
中国全科医学 ›› 2024, Vol. 27 ›› Issue (08): 985-994.DOI: 10.12114/j.issn.1007-9572.2023.0454
于海搏, 张天宇, 李新, 张佳佳, 申曼, 詹晓凯, 汤然, 范斯斌, 赵凤仪, 黄仲夏*( )
)
收稿日期:2023-06-16
修回日期:2023-09-10
出版日期:2024-03-15
发布日期:2023-12-19
通讯作者:
黄仲夏
基金资助:
YU Haibo, ZHANG Tianyu, LI Xin, ZHANG Jiajia, SHEN Man, ZHAN Xiaokai, TANG Ran, FAN Sibin, ZHAO Fengyi, HUANG Zhongxia*()
Received:2023-06-16
Revised:2023-09-10
Published:2024-03-15
Online:2023-12-19
Contact:
HUANG Zhongxia
摘要: 背景 嵌合抗原受体(CAR)-T细胞免疫疗法已在多发性骨髓瘤(MM)中取得较好的疗效,最常见的靶点为B细胞成熟抗原(BCMA)。单靶点CAR-T细胞免疫疗法的缺点是会导致疾病抵抗和复发,可能与抗原逃逸有关。为此,改进开发了双靶点CAR-T细胞治疗复发难治多发性骨髓瘤(RRMM),此方面尚缺乏系统的临床分析。 目的 对RRMM患者应用双靶点CAR-T细胞免疫疗法治疗的有效性及安全性进行Meta分析。 方法 计算机检索PubMed、Embase、Cochrane Library、Web of Science、中国知网、万方数据知识服务平台、维普网7个数据库中有关双靶点CAR-T细胞治疗RRMM的单组率研究,检索时限为建库至2023-02-06。由2名研究人员使用自制的数据表单来提取收集数据,并采用非随机对照试验方法学评价指标进行文献质量评价。采用R Studio软件进行数据分析。 结果 共纳入9篇文献,包括200例既往接受过多线治疗的RRMM患者。双靶点CAR-T细胞疗法根据不同靶点可分为4类:BCMA+CD19、BCMA+CD38,BCMA+跨膜剂与钙调节亲环素配体的相互作用者(TACI)、BCMA+人信号淋巴细胞激活分子家族成员7(CS1),其中BCMA+CD19靶点的研究较多。根据输注形式不同CAR-T细胞疗法可分为4类:双特异性CAR-T细胞、联合或序贯输注两种不同CAR-T细胞、双顺反子结构、共转导。Meta分析显示,双靶点CAR-T细胞治疗RRMM的总缓解率(ORR)为90.0%(95%CI=0.849~0.943),完全缓解率(CRR)为54.6%(95%CI=0.416~0.673),微小残留病(MRD)阴性率为75.6%(95%CI=0.489~0.952),髓外病变(EMD)总缓解率为55.1%(95%CI=0.234~0.851),最后一次随访时的复发率为29.7%(95%CI=0.141~0.454),最后一次随访时的生存率为75.6%(95%CI=0.554~0.915),3~4级细胞释放因子综合征(CRS)发生率为16.4%(95%CI=0.094~0.245),神经毒性(ICANS)发生率为4.0%(95%CI=0~0.120)。敏感性分析提示结果稳定。Egger's检验结果显示,ORR(P=0.03)及EMD总缓解率(P=0.02)提示存在一定的偏倚风险;CRR(P=0.53)、MRD阴性率(P=0.79)、最后一次随访时的复发率(P=0.71)、生存率(P=0.98)、3~4级CRS发生率(P=0.90)、ICANS发生率(P=0.30)提示不存在发表偏倚。 结论 双靶点CAR-T细胞免疫治疗RRMM显示出良好的疗效和安全性,未来需要多中心、大样本、更长随访期的研究来进一步评估其疗效和安全性。
| 步骤 | 检索式 | 命中数量(篇) |
|---|---|---|
| #1 | ("Multiple Myeloma"[Mesh]) OR ((((((((((((((((Multiple Myelomas[Title/Abstract]) OR (Myelomas,Multiple[Title/Abstract])) OR (Myeloma,Multiple[Title/Abstract])) OR (Myeloma,Plasma-Cell[Title/Abstract])) OR (Myeloma,Plasma Cell[Title/Abstract])) OR (Myelomas,Plasma-Cell[Title/Abstract])) OR (Plasma-Cell Myeloma[Title/Abstract])) OR (Plasma-Cell Myelomas[Title/Abstract])) OR (Myelomatosis[Title/Abstract])) OR (Myelomatoses[Title/Abstract])) OR (Plasma Cell Myeloma[Title/Abstract])) OR (Cell Myeloma,Plasma[Title/Abstract])) OR (Cell Myelomas,Plasma[Title/Abstract])) OR (Myelomas,Plasma Cell[Title/Abstract])) OR (Plasma Cell Myelomas[Title/Abstract])) OR (Kahler Disease[Title/Abstract])) | 60 613 |
| #2 | ("Receptors,Chimeric Antigen"[Mesh]) OR (((((((((((((((((((Antigen Receptors,Chimeric[Title/Abstract]) OR (Chimeric Antigen Receptors[Title/Abstract])) OR (Chimeric Antigen Receptor[Title/Abstract])) OR (Antigen Receptor,Chimeric[Title/Abstract])) OR (Receptor,Chimeric Antigen[Title/Abstract])) OR (Chimeric T-Cell Receptors[Title/Abstract])) OR (Chimeric T Cell Receptors[Title/Abstract])) OR (Receptors,Chimeric T-Cell[Title/Abstract])) OR (T-Cell Receptors,Chimeric[Title/Abstract])) OR (Artificial T-Cell Receptors[Title/Abstract])) OR (Artificial T Cell Receptors[Title/Abstract])) OR (Receptors,Artificial T-Cell[Title/Abstract])) OR (T-Cell Receptors,Artificial[Title/Abstract])) OR (Chimeric T-Cell Receptor[Title/Abstract])) OR (Chimeric T Cell Receptor[Title/Abstract])) OR (Receptor,Chimeric T-Cell[Title/Abstract])) OR (T-Cell Receptor,Chimeric[Title/Abstract])) OR (Chimeric Immunoreceptors[Title/Abstract])) OR (Immunoreceptors,Chimeric[Title/Abstract])) | 9 389 |
| #3 | (((((combined[Title/Abstract]) ) OR (combination[Title/Abstract])) OR (Sequential[Title/Abstract])) OR (bispecific[Title/Abstract])) OR (dual targeted[Title/Abstract]) | 1 937 548 |
| #4 | #1 AND #2 AND #3 | 209 |
表1 PubMed检索策略
Table 1 PubMed search strategy
| 步骤 | 检索式 | 命中数量(篇) |
|---|---|---|
| #1 | ("Multiple Myeloma"[Mesh]) OR ((((((((((((((((Multiple Myelomas[Title/Abstract]) OR (Myelomas,Multiple[Title/Abstract])) OR (Myeloma,Multiple[Title/Abstract])) OR (Myeloma,Plasma-Cell[Title/Abstract])) OR (Myeloma,Plasma Cell[Title/Abstract])) OR (Myelomas,Plasma-Cell[Title/Abstract])) OR (Plasma-Cell Myeloma[Title/Abstract])) OR (Plasma-Cell Myelomas[Title/Abstract])) OR (Myelomatosis[Title/Abstract])) OR (Myelomatoses[Title/Abstract])) OR (Plasma Cell Myeloma[Title/Abstract])) OR (Cell Myeloma,Plasma[Title/Abstract])) OR (Cell Myelomas,Plasma[Title/Abstract])) OR (Myelomas,Plasma Cell[Title/Abstract])) OR (Plasma Cell Myelomas[Title/Abstract])) OR (Kahler Disease[Title/Abstract])) | 60 613 |
| #2 | ("Receptors,Chimeric Antigen"[Mesh]) OR (((((((((((((((((((Antigen Receptors,Chimeric[Title/Abstract]) OR (Chimeric Antigen Receptors[Title/Abstract])) OR (Chimeric Antigen Receptor[Title/Abstract])) OR (Antigen Receptor,Chimeric[Title/Abstract])) OR (Receptor,Chimeric Antigen[Title/Abstract])) OR (Chimeric T-Cell Receptors[Title/Abstract])) OR (Chimeric T Cell Receptors[Title/Abstract])) OR (Receptors,Chimeric T-Cell[Title/Abstract])) OR (T-Cell Receptors,Chimeric[Title/Abstract])) OR (Artificial T-Cell Receptors[Title/Abstract])) OR (Artificial T Cell Receptors[Title/Abstract])) OR (Receptors,Artificial T-Cell[Title/Abstract])) OR (T-Cell Receptors,Artificial[Title/Abstract])) OR (Chimeric T-Cell Receptor[Title/Abstract])) OR (Chimeric T Cell Receptor[Title/Abstract])) OR (Receptor,Chimeric T-Cell[Title/Abstract])) OR (T-Cell Receptor,Chimeric[Title/Abstract])) OR (Chimeric Immunoreceptors[Title/Abstract])) OR (Immunoreceptors,Chimeric[Title/Abstract])) | 9 389 |
| #3 | (((((combined[Title/Abstract]) ) OR (combination[Title/Abstract])) OR (Sequential[Title/Abstract])) OR (bispecific[Title/Abstract])) OR (dual targeted[Title/Abstract]) | 1 937 548 |
| #4 | #1 AND #2 AND #3 | 209 |
| 第一作者 | 研究目的明确 | 纳入患者连贯性 | 预期数据收集 | 终点指标反应研究目的 | 终点指标评估客观性 | 随访时间是否充分 | 失访率低于5% | 是否估计了样本量 | 总分 |
|---|---|---|---|---|---|---|---|---|---|
| YAN[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| RAKESH[ | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 1 | 12 |
| YAN[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| JIANG[ | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 1 | 12 |
| MEI[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| LI[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| WANG[ | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 0 | 11 |
| TANG[ | 2 | 2 | 2 | 2 | 0 | 2 | 0 | 1 | 11 |
| ZHANG[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
表2 纳入文献质量评价结果(分)
Table 2 Inclusion of the evaluation results of the quality of literature
| 第一作者 | 研究目的明确 | 纳入患者连贯性 | 预期数据收集 | 终点指标反应研究目的 | 终点指标评估客观性 | 随访时间是否充分 | 失访率低于5% | 是否估计了样本量 | 总分 |
|---|---|---|---|---|---|---|---|---|---|
| YAN[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| RAKESH[ | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 1 | 12 |
| YAN[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| JIANG[ | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 1 | 12 |
| MEI[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| LI[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
| WANG[ | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 0 | 11 |
| TANG[ | 2 | 2 | 2 | 2 | 0 | 2 | 0 | 1 | 11 |
| ZHANG[ | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 13 |
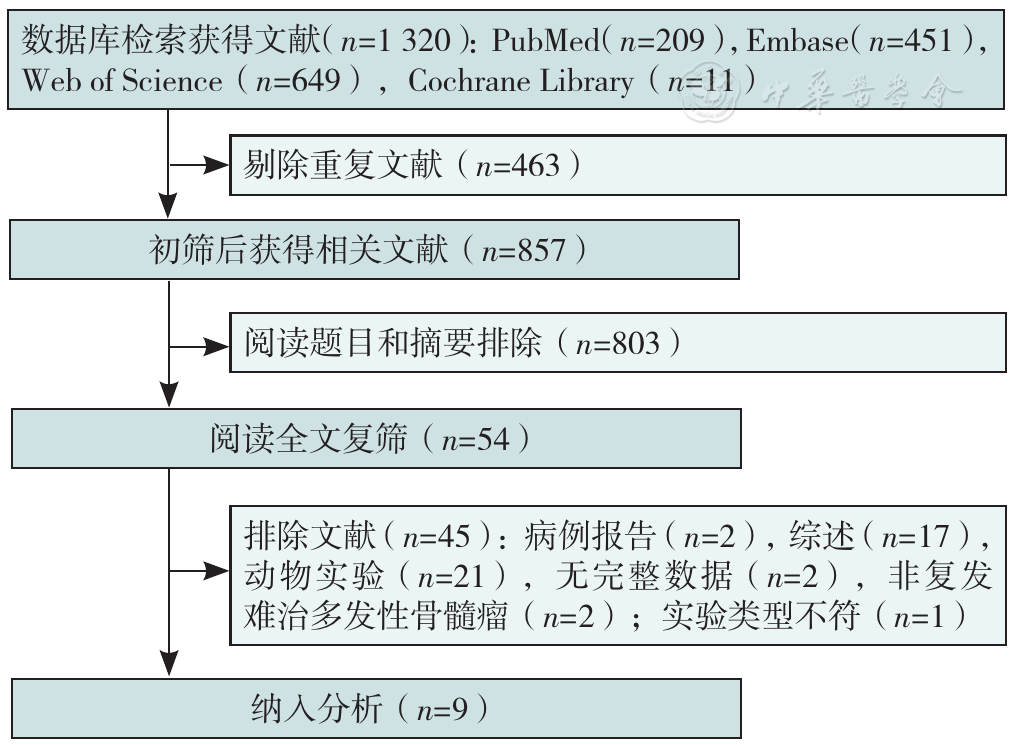
图1 文献筛选流程图
Figure 1 The literature screening flow-chart
| 第一作者 | 样本量(例) | 年龄(岁) | 既往治疗线数(线) | 既往接受ASCT | 高危遗传学异常 | 双靶点CAR-T形式 | 载体/scFv种类 | 共刺激结构 | LD | CAR-T剂量 | 随访时间 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| YAN[ | 28 | 57.5(42~69) | 3(2~8) | NA | NA | BCMA+CD19序贯 | 慢病毒/人源 | CD28+OX40 | CP/Flu | CD19(10×106/kg);BCMA(20×106/kg~68×106/kg) | 16(3~28)个月 |
| RAKESH[ | 11 | 61(45~69) | 5(3~6) | 0 | NA | BCMA+TACI双特异性 | 逆转录病毒/NA | CD28+OX40 | CP/Flu | 15×106/kg~900×106/kg | ≥4周 |
| YAN[ | 10 | NA | 4 | 60% | 50% | BCMA+CD19序贯 | 慢病毒/人源 | CD28+OX40 | CP/Flu | CD19(10×106/kg);BCMA(30×106/kg~65×106/kg) | 20个月 |
| JIANG[ | 19 | 27~71 | 5(2~7) | NA | 95% | BCMA+CD19联合 | NA | 4-1BB | CP/Flu | 分别1×106/kg~3×106/kg | 13.8(6.1~16.4)周 |
| MEI[ | 23 | 59(49~72) | 4(2~9) | 13% | 74% | BCMA+CD38双特异性 | 慢病毒/人源 | 4-1BB | CP/Flu | 0.5×106/kg~4×106/kg | 9.0(0.5~18.5)个月 |
| LI[ | 13 | NA | 5.5(2~10) | 54% | 46% | BCMA+CS1双特异性 | NA/鼠源 | 4-1BB | CP/Flu | 0.75×106/kg~3×106/kg | 290 d |
| WANG[ | 62 | 58(30~69) | 4(2~17) | 29% | 27% | BCMA+CD19联合 | 慢病毒/鼠源 | 4-1BB | CP/Flu | 分别1×106/kg | 21.3个月 |
| TANG[ | 16 | 58.5(48~78) | NA | 29% | 81% | BCMA+CD38双特异性 | 慢病毒/NA | 4-1BB | CP/Flu | 0.5×106/kg~10×106/kg | 11.5个月 |
| ZHANG[ | 22 | 56(47~68) | 8 | 86% | 86% | BCMA+CD38联合 | 慢病毒/人源(BCMA)+鼠源(CD38) | 4-1BB | CP/Flu | 分别2×106/kg | 24(0.5~33) d |
表3 纳入研究的基本特征
Table 3 Basic characteristics of the included studies
| 第一作者 | 样本量(例) | 年龄(岁) | 既往治疗线数(线) | 既往接受ASCT | 高危遗传学异常 | 双靶点CAR-T形式 | 载体/scFv种类 | 共刺激结构 | LD | CAR-T剂量 | 随访时间 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| YAN[ | 28 | 57.5(42~69) | 3(2~8) | NA | NA | BCMA+CD19序贯 | 慢病毒/人源 | CD28+OX40 | CP/Flu | CD19(10×106/kg);BCMA(20×106/kg~68×106/kg) | 16(3~28)个月 |
| RAKESH[ | 11 | 61(45~69) | 5(3~6) | 0 | NA | BCMA+TACI双特异性 | 逆转录病毒/NA | CD28+OX40 | CP/Flu | 15×106/kg~900×106/kg | ≥4周 |
| YAN[ | 10 | NA | 4 | 60% | 50% | BCMA+CD19序贯 | 慢病毒/人源 | CD28+OX40 | CP/Flu | CD19(10×106/kg);BCMA(30×106/kg~65×106/kg) | 20个月 |
| JIANG[ | 19 | 27~71 | 5(2~7) | NA | 95% | BCMA+CD19联合 | NA | 4-1BB | CP/Flu | 分别1×106/kg~3×106/kg | 13.8(6.1~16.4)周 |
| MEI[ | 23 | 59(49~72) | 4(2~9) | 13% | 74% | BCMA+CD38双特异性 | 慢病毒/人源 | 4-1BB | CP/Flu | 0.5×106/kg~4×106/kg | 9.0(0.5~18.5)个月 |
| LI[ | 13 | NA | 5.5(2~10) | 54% | 46% | BCMA+CS1双特异性 | NA/鼠源 | 4-1BB | CP/Flu | 0.75×106/kg~3×106/kg | 290 d |
| WANG[ | 62 | 58(30~69) | 4(2~17) | 29% | 27% | BCMA+CD19联合 | 慢病毒/鼠源 | 4-1BB | CP/Flu | 分别1×106/kg | 21.3个月 |
| TANG[ | 16 | 58.5(48~78) | NA | 29% | 81% | BCMA+CD38双特异性 | 慢病毒/NA | 4-1BB | CP/Flu | 0.5×106/kg~10×106/kg | 11.5个月 |
| ZHANG[ | 22 | 56(47~68) | 8 | 86% | 86% | BCMA+CD38联合 | 慢病毒/人源(BCMA)+鼠源(CD38) | 4-1BB | CP/Flu | 分别2×106/kg | 24(0.5~33) d |
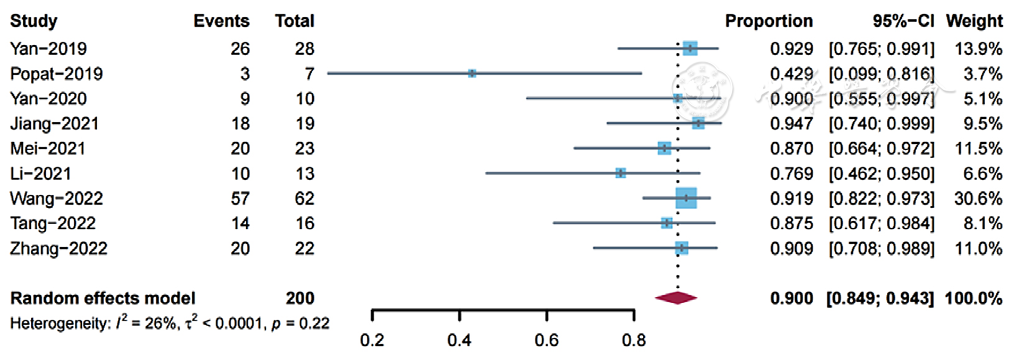
图2 双靶点CAR-T细胞治疗RRMM的ORR森林图
Figure 2 Forest plot of ORR for dual-targeted CAR-T cell therapy for RRMM
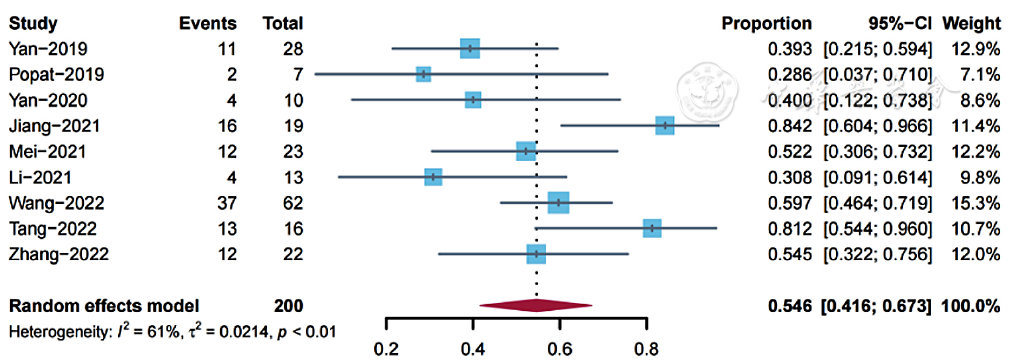
图3 双靶点CAR-T细胞治疗RRMM的CRR森林图
Figure 3 Forest plot of CRR for dual-targeted CAR-T cell therapy for RRMM
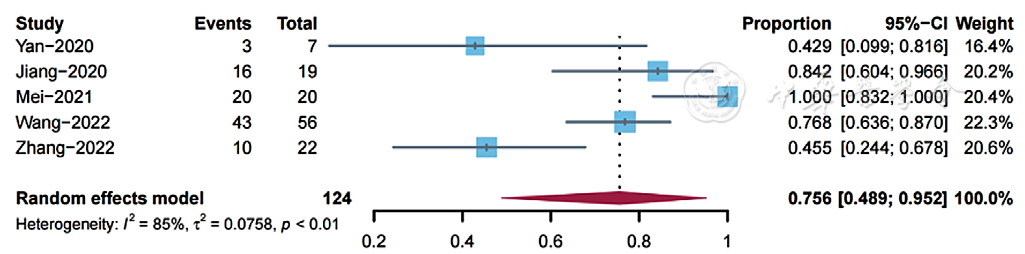
图4 双靶点CAR-T细胞治疗RRMM的MRD阴性率森林图
Figure 4 Forest plot of MRD-negative rate of dual-targeted CAR-T cell therapy for RRMM
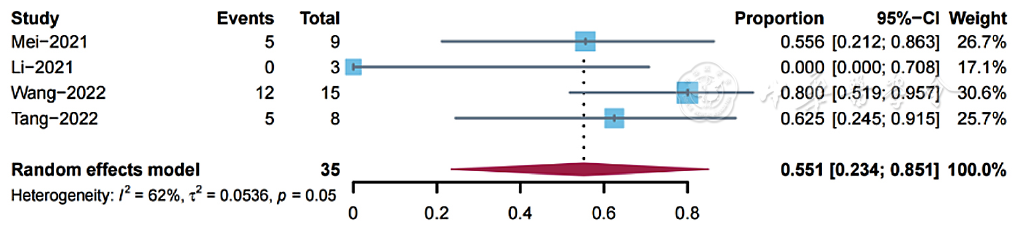
图5 双靶点CAR-T细胞治疗RRMM的EMD总缓解率森林图
Figure 5 Forest plot of overall response rate of EMD in RRMM treated with dual-targeted CAR-T cell therapy
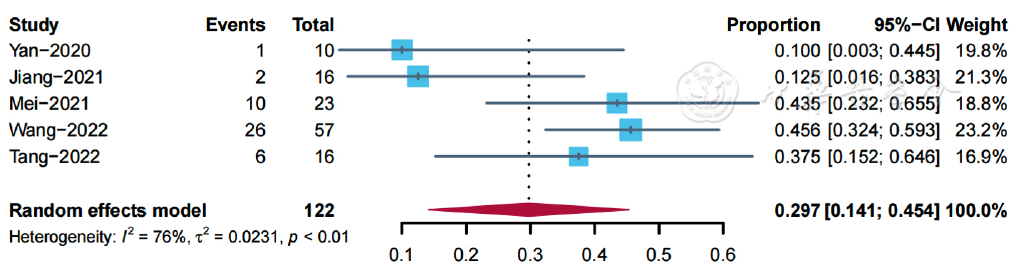
图6 双靶点CAR-T细胞治疗RRMM最后一次随访时复发率森林图
Figure 6 Forest plot of relapse rate at last follow-up for RRMM treated with dual-targeted CAR-T cell therapy
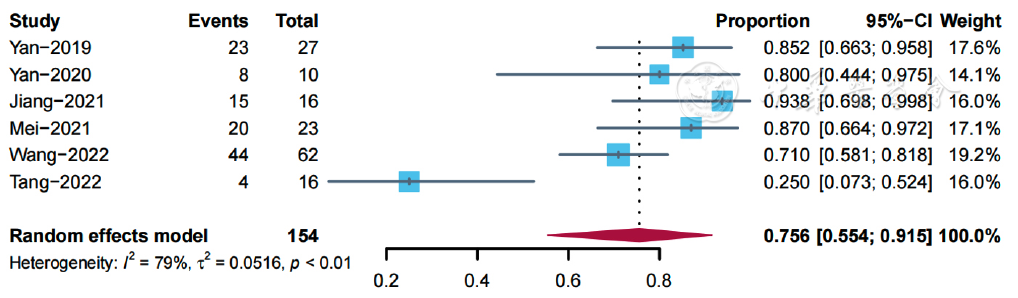
图7 双靶点CAR-T细胞治疗RRMM最后一次随访时的生存率森林图
Figure 7 Forest plot of survival at last follow-up for RRMM treated with dual-targeted CAR-T cell therapy
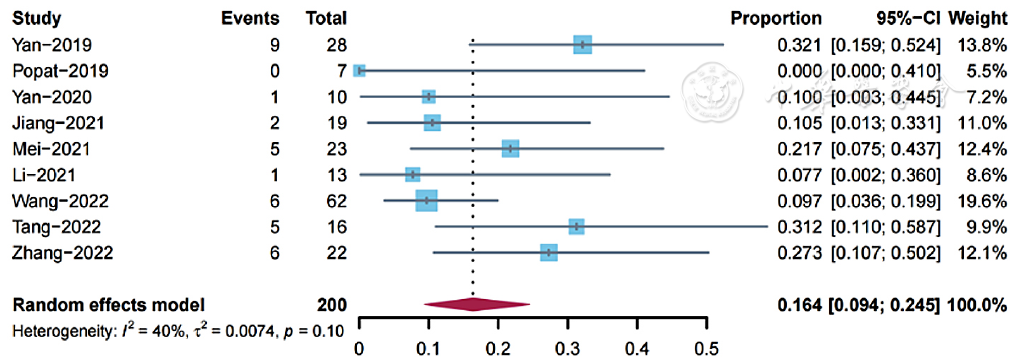
图8 双靶点CAR-T细胞治疗RRMM的3~4级CRS发生率森林图
Figure 8 Forest plot of grade 3-4 CRS incidence in RRMM treated with dual-targeted CAR-T cell therapy
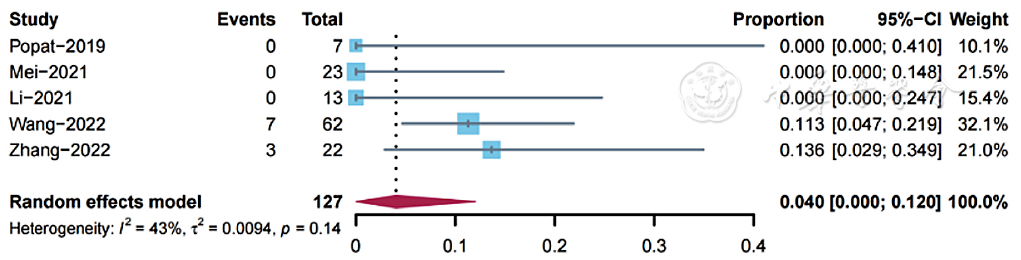
图9 双靶点CAR-T细胞治疗RRMM的ICANS发生率森林图
Figure 9 Forest plot of ICANS incidence
| 亚组 | ORR | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 纳入研究数量(篇) | 例数(n/N) | 合并比例(%) | 95%CI | I2(%) | P值 | |||||||
| 共刺激结构 | 0.42 | |||||||||||
| 4-1BB | 6[ | 139/155 | 90.4 | 0.848~0.950 | 73 | 0.03 | ||||||
| CD28+OX40 | 3[ | 38/45 | 81.2 | 0.485~0.999 | 0 | 0.71 | ||||||
| 靶点 | 0.02 | |||||||||||
| BCMA+CD19 | 4[ | 110/119 | 93.1 | 0.873~0.976 | 0 | 0.96 | ||||||
| BCMA+CD38 | 3[ | 54/61 | 88.6 | 0.788~0.960 | 0 | 0.91 | ||||||
| BCMA+TACI | 1[ | 3/7 | 42.9 | 0.099~0.816 | NA | NA | ||||||
| BCMA+CS1 | 1[ | 10/13 | 77 | 0.462~0.950 | NA | NA | ||||||
| 形式 | 0.13 | |||||||||||
| 联合/序贯输注CAR-T | 4[ | 102/115 | 92.5 | 0.865~0.970 | 0 | 0.97 | ||||||
| 双特异性CAR-T | 5[ | 82/93 | 83.5 | 0.695~0.943 | 49 | 0.1 | ||||||
| 亚组 | CRR | 3~4级CRS发生率 | ||||||||||
| 纳入研究数量(篇) | 例数(n/N) | 合并比例(%) | 95%CI | I2(%) | P值 | 纳入研究数量(篇) | 例数(n/N) | 合并比例(%) | 95%CI | I2(%) | P值 | |
| 共刺激结构 | 0.03 | 0.94 | ||||||||||
| 4-1BB | 6[ | 94/155 | 61.5 | 0.466~0.754 | 62 | 0.02 | 6[ | 25/155 | 16.2 | 0.088~0.250 | 33 | 0.19 |
| CD28+OX40 | 3[ | 17/45 | 37.5 | 0.230~0.530 | 0 | 0.89 | 3[ | 10/45 | 14.1 | 0.003~0.381 | 60 | 0.8 |
| 靶点 | 0.17 | 0.13 | ||||||||||
| BCMA+CD19 | 4[ | 68/119 | 57.2 | 0.362~0.770 | 73 | 0.1 | 4[ | 18/119 | 14.8 | 0.053~0.272 | 54 | 0.09 |
| BCMA+CD38 | 3[ | 25/61 | 62.1 | 0.439~0.788 | 49 | 0.14 | 3[ | 21/61 | 26.1 | 0.154~0.383 | 0 | 0.80 |
| BCMA+TACI | 1[ | 2/7 | 28.6 | 0.037~0.710 | NA | NA | 1[ | 0/7 | 0 | 0~0.410 | NA | NA |
| BCMA+CS1 | 1[ | 4/13 | 30.8 | 0.091~0.614 | NA | NA | 1[ | 1/13 | 7.7 | 0.002~0.360 | NA | NA |
| 形式 | 0.60 | 0.68 | ||||||||||
| 联合/序贯输注CAR-T | 4[ | 54/115 | 51.2 | 0.396~0.627 | 20 | 0.29 | 4[ | 16/115 | 18.7 | 0.077~0.326 | 62 | 0.05 |
| 双特异性CAR-T | 5[ | 57/93 | 58.4 | 0.344~0.807 | 74 | <0.01 | 5[ | 19/93 | 14.6 | 0.062~0.253 | 24 | 0.26 |
表4 双靶点CAR-T治疗RRMM疗效和不良事件的亚组分析
Table 4 Subgroup analysis of efficacy and adverse events of dual-targeted CAR-T therapy for RRMM
| 亚组 | ORR | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 纳入研究数量(篇) | 例数(n/N) | 合并比例(%) | 95%CI | I2(%) | P值 | |||||||
| 共刺激结构 | 0.42 | |||||||||||
| 4-1BB | 6[ | 139/155 | 90.4 | 0.848~0.950 | 73 | 0.03 | ||||||
| CD28+OX40 | 3[ | 38/45 | 81.2 | 0.485~0.999 | 0 | 0.71 | ||||||
| 靶点 | 0.02 | |||||||||||
| BCMA+CD19 | 4[ | 110/119 | 93.1 | 0.873~0.976 | 0 | 0.96 | ||||||
| BCMA+CD38 | 3[ | 54/61 | 88.6 | 0.788~0.960 | 0 | 0.91 | ||||||
| BCMA+TACI | 1[ | 3/7 | 42.9 | 0.099~0.816 | NA | NA | ||||||
| BCMA+CS1 | 1[ | 10/13 | 77 | 0.462~0.950 | NA | NA | ||||||
| 形式 | 0.13 | |||||||||||
| 联合/序贯输注CAR-T | 4[ | 102/115 | 92.5 | 0.865~0.970 | 0 | 0.97 | ||||||
| 双特异性CAR-T | 5[ | 82/93 | 83.5 | 0.695~0.943 | 49 | 0.1 | ||||||
| 亚组 | CRR | 3~4级CRS发生率 | ||||||||||
| 纳入研究数量(篇) | 例数(n/N) | 合并比例(%) | 95%CI | I2(%) | P值 | 纳入研究数量(篇) | 例数(n/N) | 合并比例(%) | 95%CI | I2(%) | P值 | |
| 共刺激结构 | 0.03 | 0.94 | ||||||||||
| 4-1BB | 6[ | 94/155 | 61.5 | 0.466~0.754 | 62 | 0.02 | 6[ | 25/155 | 16.2 | 0.088~0.250 | 33 | 0.19 |
| CD28+OX40 | 3[ | 17/45 | 37.5 | 0.230~0.530 | 0 | 0.89 | 3[ | 10/45 | 14.1 | 0.003~0.381 | 60 | 0.8 |
| 靶点 | 0.17 | 0.13 | ||||||||||
| BCMA+CD19 | 4[ | 68/119 | 57.2 | 0.362~0.770 | 73 | 0.1 | 4[ | 18/119 | 14.8 | 0.053~0.272 | 54 | 0.09 |
| BCMA+CD38 | 3[ | 25/61 | 62.1 | 0.439~0.788 | 49 | 0.14 | 3[ | 21/61 | 26.1 | 0.154~0.383 | 0 | 0.80 |
| BCMA+TACI | 1[ | 2/7 | 28.6 | 0.037~0.710 | NA | NA | 1[ | 0/7 | 0 | 0~0.410 | NA | NA |
| BCMA+CS1 | 1[ | 4/13 | 30.8 | 0.091~0.614 | NA | NA | 1[ | 1/13 | 7.7 | 0.002~0.360 | NA | NA |
| 形式 | 0.60 | 0.68 | ||||||||||
| 联合/序贯输注CAR-T | 4[ | 54/115 | 51.2 | 0.396~0.627 | 20 | 0.29 | 4[ | 16/115 | 18.7 | 0.077~0.326 | 62 | 0.05 |
| 双特异性CAR-T | 5[ | 57/93 | 58.4 | 0.344~0.807 | 74 | <0.01 | 5[ | 19/93 | 14.6 | 0.062~0.253 | 24 | 0.26 |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [1] | 郑博月, 付积艺, 吴佳霏, 王珺, 李慧. 卡非佐米治疗多发性骨髓瘤的疗效及安全性研究[J]. 中国全科医学, 2025, 28(30): 3806-3814. |
| [2] | 许佳兰, 阎红, 文君, 周紫彤, 王思宇. 老年癌症患者潜在不适当用药发生率的Meta分析[J]. 中国全科医学, 2025, 28(30): 3815-3822. |
| [3] | 张天宇, 于海搏, 陈飞, 李新, 张佳佳, 詹晓凯, 申曼, 汤然, 范斯斌, 赵凤仪, 黄仲夏. POEMS综合征全身系统性治疗疗效和安全性的Meta分析[J]. 中国全科医学, 2025, 28(27): 3447-3455. |
| [4] | 全家霖, 朱琳, 苏煜, 陈泽恺, 陈梓淇, 张卓凡. 运动方式对超重或肥胖儿童青少年执行功能改善效果的网状Meta分析[J]. 中国全科医学, 2025, 28(27): 3422-3431. |
| [5] | 蒋世华, 朱政, 任盈盈, 朱垚磊, 王越, 高希彬. 中国儿童青少年近视患病率及影响因素的Meta分析[J]. 中国全科医学, 2025, 28(24): 3043-3052. |
| [6] | 李浩, 李江涛, 刘丹, 王建军. 贝利尤单抗和阿尼鲁单抗及泰它西普治疗系统性红斑狼疮疗效和安全性的网状Meta分析[J]. 中国全科医学, 2025, 28(23): 2924-2933. |
| [7] | 王笑林, 李秋月, 周彦君, 张金辉, 梁涛. 转移性结直肠癌患者呋喹替尼治疗相关心血管毒性发生率和风险的Meta分析[J]. 中国全科医学, 2025, 28(23): 2934-2940. |
| [8] | 陈飞, 王金英, 于海搏, 李新, 张佳佳, 申曼, 詹晓凯, 汤然, 范斯斌, 赵凤仪, 张天宇, 黄仲夏. 中性粒细胞明胶酶相关运载蛋白、T细胞免疫球蛋白粘蛋白受体1、血管细胞黏附分子-1和激活素A升高在新诊断多发性骨髓瘤患者中的意义研究[J]. 中国全科医学, 2025, 28(22): 2740-2749. |
| [9] | 马盼盼, 王思静, 游娜, 丁大法, 鲁一兵. Danuglipron与Orforglipron治疗2型糖尿病疗效及安全性的Meta分析[J]. 中国全科医学, 2025, 28(21): 2679-2685. |
| [10] | 胡婉琴, 余深艳, 曹学华, 向凤, 贾钰. 中国儿童性早熟影响因素的Meta分析[J]. 中国全科医学, 2025, 28(21): 2661-2671. |
| [11] | 阿迪力·吐尔孙, 程刚. 非奈利酮治疗2型糖尿病肾病有效性和安全性的Meta分析[J]. 中国全科医学, 2025, 28(21): 2686-2691. |
| [12] | 郭盛滕, 张芬芬, 万迪, 于冬梅, 王庆华. 重症急性胰腺炎并发急性肺损伤危险因素的Meta分析[J]. 中国全科医学, 2025, 28(20): 2546-2554. |
| [13] | 王碧晴, 张萍, 杨红霞, 王倩, 鞠春晓, 赵俊男, 梅俊, 张颖, 徐凤芹. 中国老年高血压患者轻度认知障碍患病率及发展趋势的Meta分析[J]. 中国全科医学, 2025, 28(17): 2186-2192. |
| [14] | 樊宇, 李蓉, 龚双英, 杨小娟, 李蕊. 中国产妇配偶产后抑郁发生率的Meta分析[J]. 中国全科医学, 2025, 28(17): 2179-2185. |
| [15] | 何芸, 范焕芳, 马盼, 许绍青, 杨柳, 金明哲, 张明蕊, 陈佳琪. 不同针灸治疗方式干预乳腺癌术后上肢淋巴水肿效果的网状Meta分析[J]. 中国全科医学, 2025, 28(14): 1788-1794. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










