
中国全科医学 ›› 2024, Vol. 27 ›› Issue (02): 208-216.DOI: 10.12114/j.issn.1007-9572.2023.0396
所属专题: 老年人群健康最新文章合辑; 共病最新文章合辑; 老年问题最新文章合辑
李林瑾1, 肖丽勤2, 张丹1,*( )
)
收稿日期:2023-06-16
修回日期:2023-08-15
出版日期:2024-01-15
发布日期:2023-10-23
通讯作者:
张丹
基金资助:
LI Linjin1, XIAO Liqin2, ZHANG Dan1,*()
Received:2023-06-16
Revised:2023-08-15
Published:2024-01-15
Online:2023-10-23
Contact:
ZHANG Dan
摘要: 背景 近年来我国老年共病患者数是持续上升。随着慢性疾病数量的增加,会给老年人带来不同程度的健康损失。目前分析老年共病患者患慢性病数量的多层次因素研究尚少。 目的 结合慢性病的病因和发病特点,利用健康生态学模型,从不同层面探讨影响老年共病患者患慢性病数量的因素,为我国社区老年共病患者管理和防治提供依据。 方法 2023年2月,采用多阶段分层整群随机抽样的方法,抽取广东省社区老年(≥60岁)共病患者为调查对象。采用《老年共病患者现况及影响因素调查问卷》进行面对面询问调查,该问卷基于健康生态学模型包含个人特质层、行为特征层、人际关系层、生活和工作条件层、政策环境层。以老年共病患者患慢性病数量为因变量,根据5个层次纳入自变量,进行无序多因素Logistic回归分析。 结果 共发放问卷1 000份,回收有效问卷987份,有效回收率为98.7%。987例老年共病患者中,同时患2种慢性病346例(35.1%),同时患3种慢性病456例(46.2%),同时患>3种慢性病185例(18.7%)。无序多因素Logistic回归分析结果显示,以同时患2种慢性病的老年共病患者为对照,患慢性病的时间<6年和6~10年、本地城镇户口是老年共病患者患3种慢性病的危险因素(P<0.05),OR(95%CI)分别为2.100(1.284~3.435)、1.948(1.201~3.158)、4.103(1.496~11.250);每天均可以保证至少6 h睡眠、自评健康状况比较好、每天服药1~3种类型、经常参加社会活动、初中及以下和高中/中专学历、有城镇职工医疗保险/城乡居民医疗保险是老年共病患者患3种慢性病的保护因素(P<0.05),OR(95%CI)分别为0.528(0.322~0.867)、0.570(0.325~0.998)、0.385(0.261~0.569)、0.348(0.208~0.582)、0.412(0.175~0.972)、0.486(0.298~0.790)、0.392(0.242~0.634);男性、1周运动3次以下是老年共病患者患3种以上慢性病的危险因素(P<0.05),OR(95%CI)分别为2.563(1.634~4.021)、2.990(1.429~6.256);每天均可以保证至少6 h睡眠、自评健康状况比较好和一般、每天服药1~3种类型、年平均收入≤3万元和>3~5万元、有城镇职工医疗保险/城乡居民医疗保险是老年共病患者患3种以上的慢性病的保护因素(P<0.05),OR(95%CI)分别为0.300(0.159~0.565)、0.247(0.125~0.487)、0.448(0.240~0.837)、0.288(0.178~0.467)、0.318(0.155~0.654)、0.489(0.293~0.816)、0.416(0.229~0.755)。 结论 广东省老年共病患者同时患2~3种慢性病的比例较高(占80%以上)。影响老年共病患者患慢性病数量的因素复杂,包括性别、患慢性病时间、运动情况、睡眠情况、自评健康状况、服药情况、户籍类型、子女或家人督促吃药或锻炼情况、收入情况、受教育程度和医保类型,且不同共病数量的危险因素差异较大。因此,应该从不同层面采取相应的干预措施,减少老年共病患者患慢性病数量,提高其健康水平。
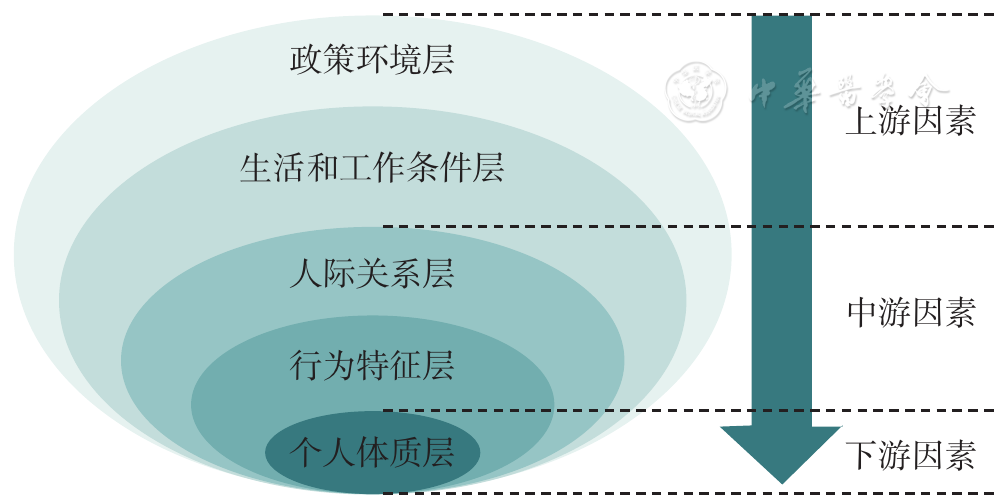
图1 健康生态学模型构架
Figure 1 Health ecology model frame
| 自变量 | 赋值 |
|---|---|
| 个人特质层 | |
| 性别 | 男=1,女=2 |
| 年龄 | 60~64岁=1,65~69岁=2,70~74岁=3,≥75岁=4 |
| BMI | 低体质量=1,正常体质量=2,超重=3,肥胖=4 |
| 行为特征层 | |
| 患慢性病的时间 | <6年=1,6~10年=2,>10年=3 |
| 吸烟 | 否=1,是=2 |
| 饮酒 | 否=1,是=2 |
| 运动频率 | 1周3次以下=1,1周3~5次=2,每天运动=3 |
| 能否保证每天至少6 h睡眠 | 每天均可以=1,1周5~6 d=2,1周4 d及以下=3 |
| 自评健康状况 | 比较好=1,一般=2,不太好=3 |
| 对自身病情的了解 | 非常了解=1,大部分了解=2,比较了解=3 |
| 每天服药的种类 | 1~3种=1,>3种=2 |
| 服药的时长 | <3年=1,3~5年=2,6~10年=3,>10年=4 |
| 是否服用保健品 | 是=1,否=2 |
| 人际关系层 | |
| 婚姻状况 | 已婚=1,丧偶=2,分居/离异=3 |
| 户籍类型 | 本地城镇户口=1,本地农村户口=2 |
| 居住情况 | 独居=1,配偶两人居住=2,与子女共同居住=3,和其他亲友居住=4 |
| 子女或家人是否会督促吃药或者锻炼 | 是=1,否=2 |
| 是否经常参与社会活动 | 是=1,否=2 |
| 生活和工作条件层 | |
| 工作状态 | 退休=1,工作=2,无业=3 |
| 年平均收入 | <1万元=1,1~3万元=2,>3~5万元=3,>5~10万元=4,>10~20万元=5 |
| 受教育程度 | 初中及以下=1,高中/中专=2,大专=3,大学本科及以上=4 |
| 看病方式 | 去社区医院找固定医生=1,去社区医院但无固定医生=2,去大医院找固定医生=3,去大医院但无固定医生=4 |
| 主要就诊的医疗机构 | 三级医院=1,二级医院=2,社区卫生服务中心=3 |
| 是否签约了家庭医生 | 是=1,否=2 |
| 社区是否有社工/志愿者帮助生活 | 经常=1,偶尔=2,没有=3 |
| 政策环境层 | |
| 医疗保险类型 | 城镇职工医疗保险/城乡居民医疗保险=1,城镇职工医疗保险/城乡居民医疗保险+商业保险=2 |
表1 基于健康生态学模型选取的自变量及赋值情况
Table 1 Selection and assignment of independent variables based on health ecology model
| 自变量 | 赋值 |
|---|---|
| 个人特质层 | |
| 性别 | 男=1,女=2 |
| 年龄 | 60~64岁=1,65~69岁=2,70~74岁=3,≥75岁=4 |
| BMI | 低体质量=1,正常体质量=2,超重=3,肥胖=4 |
| 行为特征层 | |
| 患慢性病的时间 | <6年=1,6~10年=2,>10年=3 |
| 吸烟 | 否=1,是=2 |
| 饮酒 | 否=1,是=2 |
| 运动频率 | 1周3次以下=1,1周3~5次=2,每天运动=3 |
| 能否保证每天至少6 h睡眠 | 每天均可以=1,1周5~6 d=2,1周4 d及以下=3 |
| 自评健康状况 | 比较好=1,一般=2,不太好=3 |
| 对自身病情的了解 | 非常了解=1,大部分了解=2,比较了解=3 |
| 每天服药的种类 | 1~3种=1,>3种=2 |
| 服药的时长 | <3年=1,3~5年=2,6~10年=3,>10年=4 |
| 是否服用保健品 | 是=1,否=2 |
| 人际关系层 | |
| 婚姻状况 | 已婚=1,丧偶=2,分居/离异=3 |
| 户籍类型 | 本地城镇户口=1,本地农村户口=2 |
| 居住情况 | 独居=1,配偶两人居住=2,与子女共同居住=3,和其他亲友居住=4 |
| 子女或家人是否会督促吃药或者锻炼 | 是=1,否=2 |
| 是否经常参与社会活动 | 是=1,否=2 |
| 生活和工作条件层 | |
| 工作状态 | 退休=1,工作=2,无业=3 |
| 年平均收入 | <1万元=1,1~3万元=2,>3~5万元=3,>5~10万元=4,>10~20万元=5 |
| 受教育程度 | 初中及以下=1,高中/中专=2,大专=3,大学本科及以上=4 |
| 看病方式 | 去社区医院找固定医生=1,去社区医院但无固定医生=2,去大医院找固定医生=3,去大医院但无固定医生=4 |
| 主要就诊的医疗机构 | 三级医院=1,二级医院=2,社区卫生服务中心=3 |
| 是否签约了家庭医生 | 是=1,否=2 |
| 社区是否有社工/志愿者帮助生活 | 经常=1,偶尔=2,没有=3 |
| 政策环境层 | |
| 医疗保险类型 | 城镇职工医疗保险/城乡居民医疗保险=1,城镇职工医疗保险/城乡居民医疗保险+商业保险=2 |
| 变量 | 例数 | 患2种慢性病 | 患3种慢性病 | 患>3种慢性病 | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 性别 | 30.318 | <0.001 | ||||
| 男 | 510 | 159(31.2) | 222(43.5) | 129(25.3) | ||
| 女 | 477 | 187(39.2) | 234(49.1) | 56(11.7) | ||
| 年龄(岁) | 11.333 | 0.078 | ||||
| 60~64 | 373 | 147(39.4) | 164(44.0) | 62(16.6) | ||
| 65~69 | 526 | 175(33.3) | 251(47.7) | 100(19.0) | ||
| 70~74 | 67 | 18 (26.9) | 34(50.7) | 15(22.4) | ||
| ≥75 | 21 | 6(28.6) | 7(33.3) | 8(38.1) | ||
| BMI | 17.55 | 0.007 | ||||
| 低体质量 | 58 | 21(36.2) | 21(36.2) | 16(27.6) | ||
| 正常体质量 | 624 | 240(38.5) | 278(44.6) | 106(17.0) | ||
| 超重 | 251 | 72(28.7) | 132(52.6) | 47(18.7) | ||
| 肥胖 | 54 | 13(24.1) | 25(46.3) | 16(29.6) | ||
| 患慢性病的时间(年) | 12.731 | 0.013 | ||||
| <6 | 382 | 144(37.7) | 175(45.8) | 63(16.5) | ||
| 6~10 | 448 | 143(31.9) | 224(50.0) | 81(18.1) | ||
| >10 | 157 | 59(37.6) | 57(36.3) | 41(26.1) | ||
| 吸烟 | 8.819 | 0.012 | ||||
| 否 | 841 | 291(34.6) | 403(47.9) | 147(17.5) | ||
| 是 | 146 | 55(37.7) | 53(36.3) | 38(26.0) | ||
| 饮酒 | 5.568 | 0.062 | ||||
| 否 | 748 | 265(35.4) | 355(47.5) | 128(17.1) | ||
| 是 | 239 | 81(33.9) | 101(42.3) | 57(23.8) | ||
| 运动频率 | 33.836 | <0.001 | ||||
| 1周3次以下 | 495 | 163(32.9) | 225(45.5) | 107(21.6) | ||
| 1周3~5次 | 241 | 77(32.0) | 103(42.7) | 61(25.3) | ||
| 每天运动 | 251 | 106(42.2) | 128(51.0) | 17(6.8) | ||
| 能否保证每天至少6 h睡眠 | 36.403 | <0.001 | ||||
| 每天均可以 | 419 | 177(42.2) | 195(46.5) | 47(11.2) | ||
| 1周5~6 d | 370 | 117(31.6) | 171(46.2) | 82(22.2) | ||
| 1周4 d及以下 | 198 | 52(26.3) | 90(45.5) | 56(37.1) | ||
| 自评健康状况 | 35.705 | <0.001 | ||||
| 比较好 | 370 | 151(40.8) | 177(47.8) | 42(11.4) | ||
| 一般 | 482 | 165(34.2) | 218(45.2) | 99(20.5) | ||
| 不太好 | 135 | 30(22.2) | 61(45.2) | 44(32.6) | ||
| 对自身病情的了解 | 14.730 | 0.005 | ||||
| 非常了解 | 423 | 172(40.7) | 184(43.5) | 67(15.8) | ||
| 大部分了解 | 406 | 130(32.0) | 186(45.8) | 90(22.2) | ||
| 比较了解 | 158 | 44(27.8) | 86(54.4) | 28(17.7) | ||
| 每天服药的种类(种) | 68.089 | <0.001 | ||||
| 1~3 | 679 | 293(43.2) | 287(42.3) | 99(14.6) | ||
| 4~5 | 308 | 53(17.2) | 169(54.9) | 86(27.9) | ||
| 服药的时长(年) | 19.605 | <0.05 | ||||
| <3 | 68 | 34(50.0) | 22(32.4) | 12(17.6) | ||
| 3~5 | 314 | 110(35.0) | 153(48.7) | 51(16.2) | ||
| 6~10 | 448 | 143(31.9) | 224(50.0) | 81(18.1) | ||
| >10 | 157 | 59(37.6) | 57(36.3) | 41(26.1) | ||
| 是否服用保健品 | 16.253 | <0.001 | ||||
| 是 | 230 | 71(30.9) | 95(41.3) | 64(27.8) | ||
| 否 | 757 | 275(36.3) | 361(47.7) | 121(16.0) | ||
| 婚姻状况 | 5.590 | 0.172 | ||||
| 已婚 | 926 | 322(34.8) | 433(46.8) | 171(18.5) | ||
| 丧偶 | 58 | 21(36.2) | 23(39.7) | 14(24.1) | ||
| 分居/离异 | 3 | 0 | 0 | 3(100.0) | ||
| 户籍类型 | 15.438 | <0.001 | ||||
| 本地城镇户口 | 814 | 263(32.3) | 393(48.3) | 158(19.4) | ||
| 本地农村户口 | 173 | 83(48.0) | 63(36.4) | 27(15.6) | ||
| 居住情况 | 9.219 | 0.122 | ||||
| 独居 | 53 | 21(39.6) | 17(32.1) | 15(28.3) | ||
| 配偶两人居住 | 749 | 269(35.9) | 343(45.8) | 137(18.3) | ||
| 与子女共同居住 | 184 | 56(30.4) | 95(51.6) | 33(17.9) | ||
| 和其他亲友居住 | 1 | 0 | 1(100.0) | 0 | ||
| 子女或家人是否会督促吃药或者锻炼 | 15.438 | <0.001 | ||||
| 是 | 753 | 252(33.5) | 350(46.5) | 151(20.1) | ||
| 否 | 229 | 91(39.7) | 104(45.4) | 34(14.8) | ||
| 是否经常参与社会活动 | 8.110 | 0.017 | ||||
| 是 | 845 | 311(36.8) | 378(44.7) | 156(18.5) | ||
| 否 | 142 | 35(24.6) | 78(54.9) | 29(20.4) | ||
| 工作状态 | 23.996 | <0.001 | ||||
| 退休 | 662 | 203(30.7) | 318(48.0) | 141(21.3) | ||
| 工作 | 157 | 78(49.7) | 59(37.6) | 20(12.7) | ||
| 无业 | 168 | 65(38.7) | 79(47.0) | 24(14.3) | ||
| 年平均收入(万元) | 24.539 | <0.001 | ||||
| <3 | 170 | 76(44.7) | 72(42.4) | 22(12.9) | ||
| 3~5 | 350 | 140(40.0) | 154(44.0) | 56(16.0) | ||
| >5 | 467 | 130(27.8) | 230(49.3) | 107(22.9) | ||
| 受教育程度 | 55.053 | <0.001 | ||||
| 初中及以下 | 214 | 90(42.1) | 93(43.5) | 31(40.1) | ||
| 高中/中专 | 299 | 130(43.5) | 119(39.8) | 50(16.7) | ||
| 大专 | 250 | 77(30.8) | 103(41.2) | 70(28.0) | ||
| 大学本科及以上 | 224 | 49(21.9) | 141(62.9) | 34(15.2) | ||
| 看病方式 | 11.507 | 0.059 | ||||
| 去社区医院找固定医生 | 709 | 235(33.1) | 343(48.4) | 131(18.5) | ||
| 去社区医院但无固定医生 | 172 | 64(37.2) | 78(45.3) | 30(17.4) | ||
| 去大医院找固定医生 | 100 | 44(44.0) | 32(32.0) | 24(24.0) | ||
| 去大医院但无固定医生 | 6 | 3(50.0) | 3(50.0) | 0 | ||
| 主要就诊的医疗机构 | 15.576 | 0.016 | ||||
| 三级医院 | 227 | 64(28.2) | 118(52.0) | 45(19.8) | ||
| 二级医院 | 359 | 141(39.3) | 162(45.1) | 56(15.6) | ||
| 社区卫生服务中心 | 401 | 141(35.2) | 176(43.9) | 84(20.9) | ||
| 是否签约了家庭医生 | 13.275 | 0.001 | ||||
| 是 | 638 | 202(31.7) | 299(46.9) | 137(21.5) | ||
| 否 | 349 | 144(41.3) | 157(45.0) | 48(13.8) | ||
| 社区是否有社工/志愿者帮助生活 | 9.453 | 0.051 | ||||
| 经常 | 647 | 212(32.8) | 308(47.6) | 127(19.6) | ||
| 偶尔 | 265 | 97(36.6) | 118(44.5) | 50(18.9) | ||
| 没有 | 75 | 37(49.3) | 30(40.0) | 8(10.7) | ||
| 医疗保险类型 | 27.167 | <0.001 | ||||
| 城镇职工医疗保险/城乡居民医疗保险 | 807 | 313(38.8) | 353(43.7) | 141(17.5) | ||
| 城镇职工医疗保险/城乡居民医疗保险+商业保险 | 180 | 33(18.3) | 103(57.2) | 44(24.4) | ||
表2 不同资料的老年共病患者患病种数比较[例(%)]
Table 2 Comparison of the number of chronic conditions in the elderly comorbidity patients with different characteristics
| 变量 | 例数 | 患2种慢性病 | 患3种慢性病 | 患>3种慢性病 | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 性别 | 30.318 | <0.001 | ||||
| 男 | 510 | 159(31.2) | 222(43.5) | 129(25.3) | ||
| 女 | 477 | 187(39.2) | 234(49.1) | 56(11.7) | ||
| 年龄(岁) | 11.333 | 0.078 | ||||
| 60~64 | 373 | 147(39.4) | 164(44.0) | 62(16.6) | ||
| 65~69 | 526 | 175(33.3) | 251(47.7) | 100(19.0) | ||
| 70~74 | 67 | 18 (26.9) | 34(50.7) | 15(22.4) | ||
| ≥75 | 21 | 6(28.6) | 7(33.3) | 8(38.1) | ||
| BMI | 17.55 | 0.007 | ||||
| 低体质量 | 58 | 21(36.2) | 21(36.2) | 16(27.6) | ||
| 正常体质量 | 624 | 240(38.5) | 278(44.6) | 106(17.0) | ||
| 超重 | 251 | 72(28.7) | 132(52.6) | 47(18.7) | ||
| 肥胖 | 54 | 13(24.1) | 25(46.3) | 16(29.6) | ||
| 患慢性病的时间(年) | 12.731 | 0.013 | ||||
| <6 | 382 | 144(37.7) | 175(45.8) | 63(16.5) | ||
| 6~10 | 448 | 143(31.9) | 224(50.0) | 81(18.1) | ||
| >10 | 157 | 59(37.6) | 57(36.3) | 41(26.1) | ||
| 吸烟 | 8.819 | 0.012 | ||||
| 否 | 841 | 291(34.6) | 403(47.9) | 147(17.5) | ||
| 是 | 146 | 55(37.7) | 53(36.3) | 38(26.0) | ||
| 饮酒 | 5.568 | 0.062 | ||||
| 否 | 748 | 265(35.4) | 355(47.5) | 128(17.1) | ||
| 是 | 239 | 81(33.9) | 101(42.3) | 57(23.8) | ||
| 运动频率 | 33.836 | <0.001 | ||||
| 1周3次以下 | 495 | 163(32.9) | 225(45.5) | 107(21.6) | ||
| 1周3~5次 | 241 | 77(32.0) | 103(42.7) | 61(25.3) | ||
| 每天运动 | 251 | 106(42.2) | 128(51.0) | 17(6.8) | ||
| 能否保证每天至少6 h睡眠 | 36.403 | <0.001 | ||||
| 每天均可以 | 419 | 177(42.2) | 195(46.5) | 47(11.2) | ||
| 1周5~6 d | 370 | 117(31.6) | 171(46.2) | 82(22.2) | ||
| 1周4 d及以下 | 198 | 52(26.3) | 90(45.5) | 56(37.1) | ||
| 自评健康状况 | 35.705 | <0.001 | ||||
| 比较好 | 370 | 151(40.8) | 177(47.8) | 42(11.4) | ||
| 一般 | 482 | 165(34.2) | 218(45.2) | 99(20.5) | ||
| 不太好 | 135 | 30(22.2) | 61(45.2) | 44(32.6) | ||
| 对自身病情的了解 | 14.730 | 0.005 | ||||
| 非常了解 | 423 | 172(40.7) | 184(43.5) | 67(15.8) | ||
| 大部分了解 | 406 | 130(32.0) | 186(45.8) | 90(22.2) | ||
| 比较了解 | 158 | 44(27.8) | 86(54.4) | 28(17.7) | ||
| 每天服药的种类(种) | 68.089 | <0.001 | ||||
| 1~3 | 679 | 293(43.2) | 287(42.3) | 99(14.6) | ||
| 4~5 | 308 | 53(17.2) | 169(54.9) | 86(27.9) | ||
| 服药的时长(年) | 19.605 | <0.05 | ||||
| <3 | 68 | 34(50.0) | 22(32.4) | 12(17.6) | ||
| 3~5 | 314 | 110(35.0) | 153(48.7) | 51(16.2) | ||
| 6~10 | 448 | 143(31.9) | 224(50.0) | 81(18.1) | ||
| >10 | 157 | 59(37.6) | 57(36.3) | 41(26.1) | ||
| 是否服用保健品 | 16.253 | <0.001 | ||||
| 是 | 230 | 71(30.9) | 95(41.3) | 64(27.8) | ||
| 否 | 757 | 275(36.3) | 361(47.7) | 121(16.0) | ||
| 婚姻状况 | 5.590 | 0.172 | ||||
| 已婚 | 926 | 322(34.8) | 433(46.8) | 171(18.5) | ||
| 丧偶 | 58 | 21(36.2) | 23(39.7) | 14(24.1) | ||
| 分居/离异 | 3 | 0 | 0 | 3(100.0) | ||
| 户籍类型 | 15.438 | <0.001 | ||||
| 本地城镇户口 | 814 | 263(32.3) | 393(48.3) | 158(19.4) | ||
| 本地农村户口 | 173 | 83(48.0) | 63(36.4) | 27(15.6) | ||
| 居住情况 | 9.219 | 0.122 | ||||
| 独居 | 53 | 21(39.6) | 17(32.1) | 15(28.3) | ||
| 配偶两人居住 | 749 | 269(35.9) | 343(45.8) | 137(18.3) | ||
| 与子女共同居住 | 184 | 56(30.4) | 95(51.6) | 33(17.9) | ||
| 和其他亲友居住 | 1 | 0 | 1(100.0) | 0 | ||
| 子女或家人是否会督促吃药或者锻炼 | 15.438 | <0.001 | ||||
| 是 | 753 | 252(33.5) | 350(46.5) | 151(20.1) | ||
| 否 | 229 | 91(39.7) | 104(45.4) | 34(14.8) | ||
| 是否经常参与社会活动 | 8.110 | 0.017 | ||||
| 是 | 845 | 311(36.8) | 378(44.7) | 156(18.5) | ||
| 否 | 142 | 35(24.6) | 78(54.9) | 29(20.4) | ||
| 工作状态 | 23.996 | <0.001 | ||||
| 退休 | 662 | 203(30.7) | 318(48.0) | 141(21.3) | ||
| 工作 | 157 | 78(49.7) | 59(37.6) | 20(12.7) | ||
| 无业 | 168 | 65(38.7) | 79(47.0) | 24(14.3) | ||
| 年平均收入(万元) | 24.539 | <0.001 | ||||
| <3 | 170 | 76(44.7) | 72(42.4) | 22(12.9) | ||
| 3~5 | 350 | 140(40.0) | 154(44.0) | 56(16.0) | ||
| >5 | 467 | 130(27.8) | 230(49.3) | 107(22.9) | ||
| 受教育程度 | 55.053 | <0.001 | ||||
| 初中及以下 | 214 | 90(42.1) | 93(43.5) | 31(40.1) | ||
| 高中/中专 | 299 | 130(43.5) | 119(39.8) | 50(16.7) | ||
| 大专 | 250 | 77(30.8) | 103(41.2) | 70(28.0) | ||
| 大学本科及以上 | 224 | 49(21.9) | 141(62.9) | 34(15.2) | ||
| 看病方式 | 11.507 | 0.059 | ||||
| 去社区医院找固定医生 | 709 | 235(33.1) | 343(48.4) | 131(18.5) | ||
| 去社区医院但无固定医生 | 172 | 64(37.2) | 78(45.3) | 30(17.4) | ||
| 去大医院找固定医生 | 100 | 44(44.0) | 32(32.0) | 24(24.0) | ||
| 去大医院但无固定医生 | 6 | 3(50.0) | 3(50.0) | 0 | ||
| 主要就诊的医疗机构 | 15.576 | 0.016 | ||||
| 三级医院 | 227 | 64(28.2) | 118(52.0) | 45(19.8) | ||
| 二级医院 | 359 | 141(39.3) | 162(45.1) | 56(15.6) | ||
| 社区卫生服务中心 | 401 | 141(35.2) | 176(43.9) | 84(20.9) | ||
| 是否签约了家庭医生 | 13.275 | 0.001 | ||||
| 是 | 638 | 202(31.7) | 299(46.9) | 137(21.5) | ||
| 否 | 349 | 144(41.3) | 157(45.0) | 48(13.8) | ||
| 社区是否有社工/志愿者帮助生活 | 9.453 | 0.051 | ||||
| 经常 | 647 | 212(32.8) | 308(47.6) | 127(19.6) | ||
| 偶尔 | 265 | 97(36.6) | 118(44.5) | 50(18.9) | ||
| 没有 | 75 | 37(49.3) | 30(40.0) | 8(10.7) | ||
| 医疗保险类型 | 27.167 | <0.001 | ||||
| 城镇职工医疗保险/城乡居民医疗保险 | 807 | 313(38.8) | 353(43.7) | 141(17.5) | ||
| 城镇职工医疗保险/城乡居民医疗保险+商业保险 | 180 | 33(18.3) | 103(57.2) | 44(24.4) | ||
| 影响因素 | 患3种慢性病 | 患>3种慢性病 | ||||
|---|---|---|---|---|---|---|
| OR值 | 95%CI | P值 | OR值 | 95%CI | P值 | |
| 个人特质层 | ||||||
| 性别(对照=女性) | ||||||
| 男性 | 1.046 | (0.753~1.453) | 0.790 | 2.563 | (1.634~4.021) | <0.001 |
| BMI(对照=肥胖) | ||||||
| 低体质量 | 0.571 | (0.209~1.555) | 0.273 | 1.190 | (0.360~3.927) | 0.776 |
| 正常体质量 | 0.562 | (0.257~1.230) | 0.149 | 0.470 | (0.177~1.247) | 0.129 |
| 超重 | 0.945 | (0.417~2.141) | 0.891 | 0.917 | (0.328~2.568) | 0.869 |
| 行为特征层 | ||||||
| 患慢性病的时间(对照=>10年) | ||||||
| <6年 | 2.100 | (1.284~3.435) | 0.003 | 0.963 | (0.508~1.758) | 0.903 |
| 6~10年 | 1.948 | (1.201~3.158) | 0.007 | 1.154 | (0.634~2.100) | 0.640 |
| 运动频率(对照=每天运动) | ||||||
| 1周运动3次以下 | 1.072 | (0.665~1.727) | 0.776 | 2.990 | (1.429~6.256) | 0.004 |
| 1周运动3~5次 | 0.853 | (0.523~1.392) | 0.525 | 2.739 | (1.304~5.754) | 0.008 |
| 能否保证每天至少6 h睡眠(对照=1周4 d及以下) | ||||||
| 每天可以 | 0.528 | (0.322~0.867) | 0.012 | 0.300 | (0.159~0.565) | <0.001 |
| 1周5~6 d | 0.805 | (0.506~1.281) | 0.360 | 0.574 | (0.326~1.010) | 0.054 |
| 自评健康状况(对照=不太好) | ||||||
| 比较好 | 0.570 | (0.325~0.998) | 0.049 | 0.247 | (0.125~0.487) | <0.001 |
| 一般 | 0.718 | (0.416~1.240) | 0.235 | 0.448 | (0.240~0.837) | 0.012 |
| 每天服药的种类(对照=>3种) | ||||||
| 1~3种 | 0.385 | (0.261~0.569) | <0.001 | 0.288 | (0.178~0.467) | <0.001 |
| 人际关系层 | ||||||
| 户籍类型(对照=本地农村户口) | ||||||
| 本地城镇户口 | 4.103 | (1.496~11.250) | 0.006 | 0.827 | (0.220~3.113) | 0.779 |
| 子女或家人是否会督促吃药或锻炼(对照=否) | ||||||
| 是 | 1.329 | (0.908~1.945) | 0.143 | 2.357 | (1.371~4.050) | 0.002 |
| 是否经常参加社会活动(对照=否) | ||||||
| 是 | 0.348 | (0.208~0.582) | <0.001 | 0.655 | (0.343~1.248) | 0.198 |
| 生活和工作条件层 | ||||||
| 工作状态(对照=无业) | ||||||
| 退休 | 0.576 | (0.254~1.302) | 0.185 | 1.761 | (0.534~5.806) | 0.353 |
| 工作 | 1.153 | (0.404~3.288) | 0.791 | 0.359 | (0.099~1.307) | 0.120 |
| 年平均收入(对照=>5万元) | ||||||
| ≤3万元 | 0.704 | (0.430~1.153) | 0.163 | 0.318 | (0.155~0.654) | 0.002 |
| >3~5万元 | 0.795 | (0.539~1.171) | 0.245 | 0.489 | (0.293~0.816) | 0.006 |
| 受教育程度(对照=大学本科及以上) | ||||||
| 初中及以下 | 0.412 | (0.175~0.972) | 0.043 | 2.141 | (0.659~6.954) | 0.205 |
| 高中/中专 | 0.486 | (0.298~0.790) | 0.004 | 0.998 | (0.522~1.911) | 0.996 |
| 大专 | 0.691 | (0.417~1.145) | 0.151 | 1.798 | (0.947~3.413) | 0.073 |
| 政策环境层 | ||||||
| 医疗保险类型(对照=城镇职工医疗保险/城乡居民医疗保险+商业保险) | ||||||
| 城镇职工医疗保险/城乡居民医疗保险 | 0.392 | (0.242~0.634) | <0.001 | 0.416 | (0.229~0.755) | 0.004 |
表3 老年共病患者患慢性病数量影响因素的无序多因素Logistic回归分析
Table 3 Unordered multivariate Logistic regression analysis of factors influencing the number of chronic conditions in elderly comorbidity patients
| 影响因素 | 患3种慢性病 | 患>3种慢性病 | ||||
|---|---|---|---|---|---|---|
| OR值 | 95%CI | P值 | OR值 | 95%CI | P值 | |
| 个人特质层 | ||||||
| 性别(对照=女性) | ||||||
| 男性 | 1.046 | (0.753~1.453) | 0.790 | 2.563 | (1.634~4.021) | <0.001 |
| BMI(对照=肥胖) | ||||||
| 低体质量 | 0.571 | (0.209~1.555) | 0.273 | 1.190 | (0.360~3.927) | 0.776 |
| 正常体质量 | 0.562 | (0.257~1.230) | 0.149 | 0.470 | (0.177~1.247) | 0.129 |
| 超重 | 0.945 | (0.417~2.141) | 0.891 | 0.917 | (0.328~2.568) | 0.869 |
| 行为特征层 | ||||||
| 患慢性病的时间(对照=>10年) | ||||||
| <6年 | 2.100 | (1.284~3.435) | 0.003 | 0.963 | (0.508~1.758) | 0.903 |
| 6~10年 | 1.948 | (1.201~3.158) | 0.007 | 1.154 | (0.634~2.100) | 0.640 |
| 运动频率(对照=每天运动) | ||||||
| 1周运动3次以下 | 1.072 | (0.665~1.727) | 0.776 | 2.990 | (1.429~6.256) | 0.004 |
| 1周运动3~5次 | 0.853 | (0.523~1.392) | 0.525 | 2.739 | (1.304~5.754) | 0.008 |
| 能否保证每天至少6 h睡眠(对照=1周4 d及以下) | ||||||
| 每天可以 | 0.528 | (0.322~0.867) | 0.012 | 0.300 | (0.159~0.565) | <0.001 |
| 1周5~6 d | 0.805 | (0.506~1.281) | 0.360 | 0.574 | (0.326~1.010) | 0.054 |
| 自评健康状况(对照=不太好) | ||||||
| 比较好 | 0.570 | (0.325~0.998) | 0.049 | 0.247 | (0.125~0.487) | <0.001 |
| 一般 | 0.718 | (0.416~1.240) | 0.235 | 0.448 | (0.240~0.837) | 0.012 |
| 每天服药的种类(对照=>3种) | ||||||
| 1~3种 | 0.385 | (0.261~0.569) | <0.001 | 0.288 | (0.178~0.467) | <0.001 |
| 人际关系层 | ||||||
| 户籍类型(对照=本地农村户口) | ||||||
| 本地城镇户口 | 4.103 | (1.496~11.250) | 0.006 | 0.827 | (0.220~3.113) | 0.779 |
| 子女或家人是否会督促吃药或锻炼(对照=否) | ||||||
| 是 | 1.329 | (0.908~1.945) | 0.143 | 2.357 | (1.371~4.050) | 0.002 |
| 是否经常参加社会活动(对照=否) | ||||||
| 是 | 0.348 | (0.208~0.582) | <0.001 | 0.655 | (0.343~1.248) | 0.198 |
| 生活和工作条件层 | ||||||
| 工作状态(对照=无业) | ||||||
| 退休 | 0.576 | (0.254~1.302) | 0.185 | 1.761 | (0.534~5.806) | 0.353 |
| 工作 | 1.153 | (0.404~3.288) | 0.791 | 0.359 | (0.099~1.307) | 0.120 |
| 年平均收入(对照=>5万元) | ||||||
| ≤3万元 | 0.704 | (0.430~1.153) | 0.163 | 0.318 | (0.155~0.654) | 0.002 |
| >3~5万元 | 0.795 | (0.539~1.171) | 0.245 | 0.489 | (0.293~0.816) | 0.006 |
| 受教育程度(对照=大学本科及以上) | ||||||
| 初中及以下 | 0.412 | (0.175~0.972) | 0.043 | 2.141 | (0.659~6.954) | 0.205 |
| 高中/中专 | 0.486 | (0.298~0.790) | 0.004 | 0.998 | (0.522~1.911) | 0.996 |
| 大专 | 0.691 | (0.417~1.145) | 0.151 | 1.798 | (0.947~3.413) | 0.073 |
| 政策环境层 | ||||||
| 医疗保险类型(对照=城镇职工医疗保险/城乡居民医疗保险+商业保险) | ||||||
| 城镇职工医疗保险/城乡居民医疗保险 | 0.392 | (0.242~0.634) | <0.001 | 0.416 | (0.229~0.755) | 0.004 |
| [1] |
|
| [2] |
关于印发"十四五"健康老龄化规划的通知[EB/OL]. [2023-05-22].
|
| [3] |
World Health Organization. The world health report 2008 :primary health care now more than ever[R]. Geneva:WHO,2008.
|
| [4] |
原温佩,薛雅卿,蔡圆,等. 老年人多重慢病患病现状及生活自理能力调查[J]. 现代预防医学,2021,48(14):2590-2593,2598.
|
| [5] |
闫巍,王杰萍,张洪波,等. 老年共病患者在诊疗中面临的问题及应对策略[J]. 中国全科医学,2018,21(3):261-264. DOI:10.3969/j.issn.1007-9572.2017.00.207.
|
| [6] |
杜金,袁玫,齐元涛,等. 基于健康生态学模型的中国老年人糖尿病患病影响因素研究[J]. 中国慢性病预防与控制,2022,30(6):457-460,464. DOI:10.16386/j.cjpccd.issn.1004-6194.2022.06.012.
|
| [7] |
雷普超,吴洋洋,李玲玲,等. 健康生态学视角下我国中老年慢性病患者抑郁的影响因素分析[J]. 现代预防医学,2021,48(7):1253-1258.
|
| [8] |
毛瑛,朱斌,刘锦林,等. 健康生态学视角下中老年人群慢性病影响因素实证[J]. 西安交通大学学报:社会科学版,2015,35(5):15-24. DOI:10.15896/j.xjtuskxb.201505003.
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] | |
| [13] |
李鲁,王红妹,沈毅. SF-36健康调查量表中文版的研制及其性能测试[J]. 中华预防医学杂志,2002,36(2):109-113. DOI:10.3760/j:issn:0253-9624.2002.02.011.
|
| [14] |
曹文君,郭颖,平卫伟,等. HPLP-Ⅱ健康促进生活方式量表中文版的研制及其性能测试[J]. 中华疾病控制杂志,2016,20(3):286-289. DOI:10.16462/j.cnki.zhjbkz.2016.03.018.
|
| [15] |
王洁,莫永珍,卞茸文,等. 中文版8条目Morisky用药依从性问卷在老年2型糖尿病患者中应用信效度[J]. 中国老年学杂志,2015,35(21):6242-6244. DOI:10.3969/j.issn.1005-9202.2015.21.115.
|
| [16] |
张露文,陆翘楚,赵洋. 中国中老年人慢病共病组合及其健康结局差异[J]. 中山大学学报(医学科学版),2023,44(1):159-168. DOI:10.13471/j.cnki.j.sun.yat-sen.univ(med.sci).20221215.001.
|
| [17] |
张丽,李耘,钱玉英,等. 老年共病的现状及研究进展[J]. 中华老年多器官疾病杂志,2021,20(1):67-71. DOI:10.11915/j.issn.1671-5403.2021.01.015.
|
| [18] |
|
| [19] |
|
| [20] |
刘贵浩,薛允莲. 广东省老年人慢性病共病现状及影响因素研究[J]. 中国医院统计,2022,29(2):103-107. DOI:10.3969/j.issn.1006-5253.2022.02.005.
|
| [21] |
|
| [22] |
王浩,张琳,方晓雅,等. 中国中老年人慢性病共病现状及其空间分布研究[J]. 中国全科医学,2022,25(10):1186-1190,1196. DOI:10.12114/j.issn.1007-9572.2022.0127.
|
| [23] |
张家泳,丛守婧,麦勇强,等. 广东省中山市中老年人慢性病共病现状调查及流行病学分析[J]. 现代医药卫生,2018,34(9):1320-1323. DOI:10.3969/j.issn.1009-5519.2018.09.013.
|
| [24] |
范利,邹晓. 我国老年慢性病管理及预防保健的重要意义[J]. 中国临床保健杂志,2020,23(2):145-147. DOI:10.3969/J.issn.1672-6790.2020.02.001.
|
| [25] |
|
| [26] |
李越,李颖菲,郭丽芳,等. 河南省老年人常见慢性病共病现状分析[J]. 现代预防医学,2020,47(15):2797-2800.
|
| [27] |
程杨杨,曹志,侯洁,等. 中国中老年人群慢性病现状调查与共病关联分析[J]. 中华疾病控制杂志,2019,23(6):625-629. DOI:10.16462/j.cnki.zhjbkz.2019.06.002.
|
| [28] |
孙雨丹,杨林,刘洁,等. 基于健康生态学模型的慢性病影响因素分析[J]. 现代预防医学,2020,47(15):2700-2702,2784.
|
| [29] |
蔡芳,符秀梅,张万英,等. 有氧运动对老年慢性病患者健康管理效果的影响[J]. 中国老年学杂志,2019,39(19):4762-4765. DOI:10.3969/j.issn.1005-9202.2019.19.042.
|
| [30] |
|
| [31] |
齐元涛,柳言,杜金,等. 基于健康生态学模型的我国老年人慢性病共病影响因素研究[J]. 中国全科医学,2023,26(1):50-57. DOI:10.12114/j.issn.1007-9572.2022.0458.
|
| [32] |
|
| [33] |
段思宇,杨占基,孙健,等. 中国中老年人睡眠时间与高血压患病率的相关性——基于健康与养老追踪调查[J]. 中华疾病控制杂志,2021,25(9):1054-1059. DOI:10.16462/j.cnki.zhjbkz.2021.09.011.
|
| [34] |
张可人,姜云芳,刘乐正. 贵阳市老年人自评健康现状及影响因素分析[J]. 中国初级卫生保健,2021,35(11):10-13. DOI:10.3969/j.issn.1001-568X.2021.11.0004.
|
| [35] |
幸晓琼,王红梅,杨佳丹,等. 某院心内科住院患者严重和禁忌的潜在药物相互作用横断面研究[J]. 中国药学杂志,2021,56(8):694-698.
|
| [36] |
|
| [37] |
郭小榕. 中国老年人慢性病共病现况及主要影响因素的研究[D]. 厦门:厦门大学,2019.
|
| [38] |
程学娟. 高血压患者自我管理行为及影响因素的健康生态学模型解释[D]. 济南:山东大学,2014.
|
| [39] |
范涛,曹乾,蒋露露,等. 老年人慢性病影响因素的健康生态学模型解释[J]. 中国全科医学,2012,15(1):33-36,40. DOI:10.3969/j.issn.1007-9572.2012.01.011.
|
| [40] |
中国老年保健医学研究会老龄健康服务与标准化分会,《中国老年保健医学》杂志编辑委员会. 居家(养护)老年人共病综合评估和防控专家共识[J]. 中国老年保健医学,2018,16(3):28-31. DOI:10.3969/j.issn.1672-2671.2018.03.007.
|
| [41] |
张勇,白雅敏,邵月琴,等. 新千年发展目标框架下的全球慢性病防控政策的回顾与建议[J]. 中国慢性病预防与控制,2016,24(8):629-632. DOI:10.16386/j.cjpccd.issn.1004-6194.2016.08.021.
|
| [42] |
章轶立,黄馨懿,齐保玉,等. 老年人群共病问题现状挑战与应对策略[J]. 中国全科医学,2022,25(35):4363-4368. DOI:10.12114/j.issn.1007-9572.2022.0514.
|
| [43] |
许明璐,徐旺来,张彦,等. 我国老年人慢性病和抑郁关系研究[J]. 中国卫生统计,2020,37(6):929-931. DOI:10.3969/j.issn.1002-3674.2020.06.034.
|
| [1] | 徐百川, 王艳, 张彭, 李艺婷, 刘飞来, 谢洋. 慢性阻塞性肺疾病共病肺癌筛查工具分析[J]. 中国全科医学, 2025, 28(30): 3847-3852. |
| [2] | 罗新宇, 刘瑾, 陈海龙. 1990—2021年中国和全球胰腺炎疾病负担趋势分析及2022—2031年预测研究[J]. 中国全科医学, 2025, 28(26): 3321-3327. |
| [3] | 余孜孜, 刘杜丽, 李熙敏, 阮春怡, 尹向阳, 蔡乐. 农村高血压患病和自我管理现状及影响因素研究[J]. 中国全科医学, 2025, 28(25): 3137-3143. |
| [4] | 蒋世华, 朱政, 任盈盈, 朱垚磊, 王越, 高希彬. 中国儿童青少年近视患病率及影响因素的Meta分析[J]. 中国全科医学, 2025, 28(24): 3043-3052. |
| [5] | 扶蓉, 石磊, 何飞英. 中老年人糖尿病与抑郁状态共病:睡眠和运动及社交活动的影响研究[J]. 中国全科医学, 2025, 28(20): 2491-2500. |
| [6] | 郝爱华, 曾子莹, 金爱琼, 唐玲玲, 郑梓悫, 马景泰, 赵建国, 曾韦霖, 肖建鹏, 聂辉, 杨颖. 老年高血压患者可避免住院的影响因素研究[J]. 中国全科医学, 2025, 28(19): 2370-2375. |
| [7] | 韩正, 孙梦, 傅方琳, 潘姚佳, 王为强. 50岁及以上人群三酰甘油葡萄糖指数与心血管代谢性共病关系的研究[J]. 中国全科医学, 2025, 28(18): 2278-2284. |
| [8] | 王碧晴, 张萍, 杨红霞, 王倩, 鞠春晓, 赵俊男, 梅俊, 张颖, 徐凤芹. 中国老年高血压患者轻度认知障碍患病率及发展趋势的Meta分析[J]. 中国全科医学, 2025, 28(17): 2186-2192. |
| [9] | 陈兴超, 高振华, 徐生刚, 邹永刚, 钱军, 魏建仝. 1990—2021年全球和中国及不同社会人口学指数地区骨关节炎疾病负担趋势分析[J]. 中国全科医学, 2025, 28(17): 2172-2178. |
| [10] | 黄志杰, 麦志华, 王皓翔, 何煜明, 邓巧妍, 戴燃然, 周志衡. 老年"三高"共患情况和家庭功能的现状及影响因素研究[J]. 中国全科医学, 2025, 28(16): 2001-2010. |
| [11] | 宋明莎, 王宥匀, 李春生, 乔慧. 基于潜在类别分析的宁夏回族自治区南部山区农村老年人慢性病共病对日常生活活动能力的影响研究[J]. 中国全科医学, 2025, 28(16): 2033-2038. |
| [12] | 曹晨晨, 郑吕云, 王琳, 刘静. 高血压与2型糖尿病共病患者家庭医生签约服务偏好研究[J]. 中国全科医学, 2025, 28(16): 2011-2016. |
| [13] | 令垚, 张文滨, 王仕鸿, 陈永泽, 董文娇, 邓星妤, 丁元林. 1990—2021年中国类风湿关节炎疾病负担变化趋势分析及预测研究[J]. 中国全科医学, 2025, 28(15): 1914-1922. |
| [14] | 张滢, 姜欣彤, 王萍玉. 基于健康生态学模型的中国女性老年人群抑郁症状影响因素研究[J]. 中国全科医学, 2025, 28(13): 1595-1600. |
| [15] | 孙清, 吴玉霄, 崔立敏. 中国2型糖尿病患者肌少-骨质疏松症患病率的Meta分析[J]. 中国全科医学, 2025, 28(12): 1520-1526. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










