中国全科医学 ›› 2023, Vol. 26 ›› Issue (26): 3252-3258.DOI: 10.12114/j.issn.1007-9572.2023.0103
所属专题: 内分泌代谢性疾病最新文章合辑; 消化系统疾病最新文章合辑
孔德先1, 邢煜玲2, 孙文文3, 张智敏4, 周霏4, 马慧娟2,*( )
)
KONG Dexian1, XING Yuling2, SUN Wenwen3, ZHANG Zhimin4, ZHOU Fei4, MA Huijuan2,*()
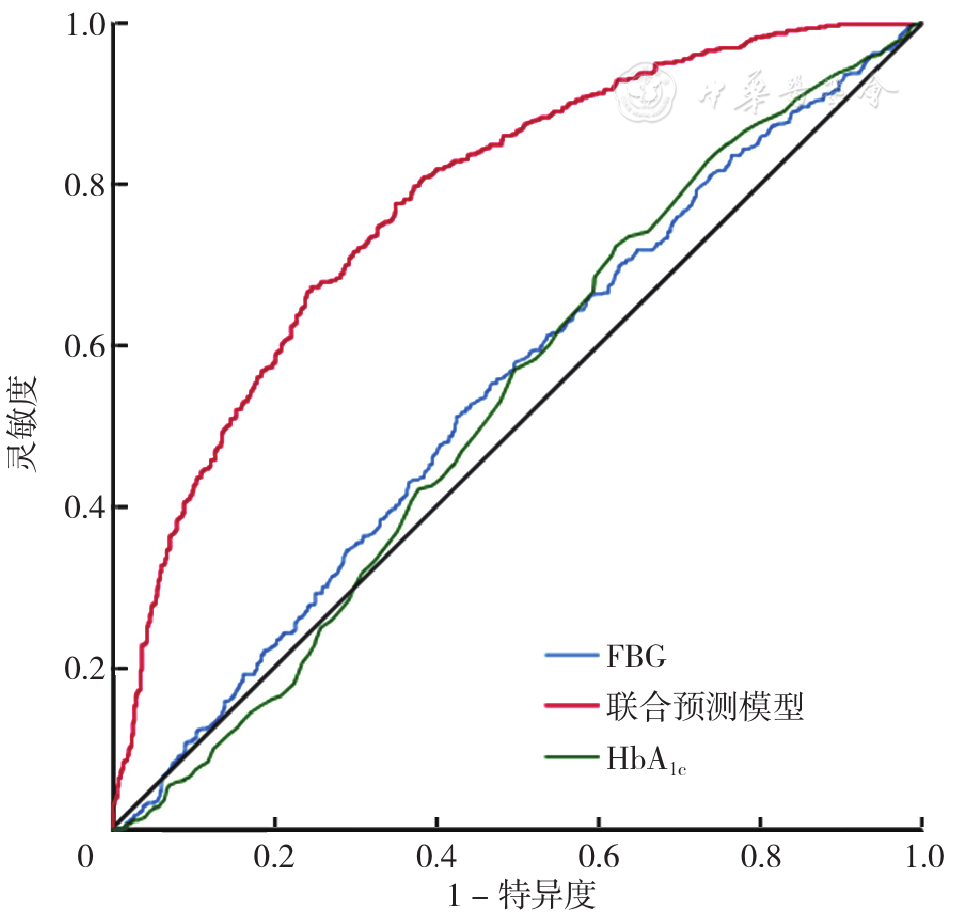
摘要: 背景 代谢相关脂肪性肝病(MAFLD)是近年来引起肝脏疾病发病率和死亡率升高的主要原因,2型糖尿病(T2DM)是MAFLD进展的驱动因素。预估葡糖糖处理率(eGDR)是T2DM患者胰岛素抵抗的简易评估指标,但与MAFLD的关系研究较少。 目的 eGDR与T2DM合并MAFLD的关系及其预测价值。 方法 选取2019年于河北省人民医院住院治疗的1 434例T2DM患者为研究对象。收集患者基本信息,采集患者肘静脉血进行实验室检查,采用腹部超声检查患者肝脏情况。根据腹部超声检查结果,将T2DM患者分为合并MAFLD组(n=734)和未合并MAFLD组(n=700)。根据eGDR三分位数将研究对象分为T1组(eGDR≤5.09,n=477)、T2组(5.09<eGDR≤7.11,n=478)、T3组(eGDR>7.11,n=479)。采用Spearman秩相关分析探讨eGDR与研究对象基线资料的相关性。采用单因素及多因素Logistic回归分析探究合并MAFLD的影响因素。评价eGDR与性别、年龄、高血压、糖化血红蛋白(HbA1c)、BMI、谷氨酰转移酶(GGT)的相乘交互作用。绘制受试者工作特征曲线(ROC)评估联合预测模型、FBG、HbA1c对T2DM合并MAFLD预测价值,计算ROC曲线下面积(AUC)并采用Delong检验进行比较。 结果 合并MAFLD组患者年龄、病程、HDL-C、eGDR低于未合并MAFLD组,BMI、饮酒、高血压及吸烟比例、空腹血糖(FBG)、尿酸(UA)、总胆固醇(TC)、TG、低密度脂蛋白胆固醇(LDL-C)、丙氨酸氨基转移酶(ALT)、天冬氨酸氨基转移酶(AST)、GGT、ALB水平高于未合并MAFLD组患者(P<0.05)。T3组高血压比例、年龄、BMI、FBG、HbA1c、血清肌酐(Scr)、TG低于T1、T2组,GGT水平低于T1组,HDL-C、ALB高于T1、T2组(P<0.05);T2组高血压比例、BMI、FBG、HbA1c、TG低于T1组(P<0.05)。合并MAFLD组eGDR与年龄、FBG、ALB水平呈负相关(P<0.05);未合并MAFLD组eGDR与年龄、病程、FBG、Scr、TG、ALB呈负相关(P<0.05),与HDL-C、AST、GGT呈正相关(P<0.05)。多因素Logistic回归分析结果显示eGDR〔OR=0.814,95%CI(0.772,0.858),P<0.001〕、T1组〔OR=1.310,95%CI(1.003,1.712),P=0.048〕、T2组〔OR=2.554,95%CI(1.941,3.359),P<0.001〕是T2DM合并MAFLD的影响因素(P<0.05)。BMI(P交互<0.001)、GGT(P交互=0.033)、高血压(P交互<0.001)与eGDR存在交互作用。联合预测模型预测T2DM合并MAFLD的AUC为0.743,大于FBG(Z=3.227,P=0.001)、HbA1c(Z=1.877,P=0.061)。 结论 合并MAFLD的T2DM患者eGDR低于未合并MAFLD患者。eGDR是T2DM合并MAFLD的危险因素。eGDR联合预测模型可以作为评估T2DM合并MAFLD发生风险的预测指标。