中国全科医学 ›› 2023, Vol. 26 ›› Issue (17): 2125-2131.DOI: 10.12114/j.issn.1007-9572.2022.0832
所属专题: 儿科最新文章合辑; 呼吸疾病文章合辑; 脑健康最新研究合辑
薛婧如, 孙素真*( )
)
XUE Jingru, SUN Suzhen*()
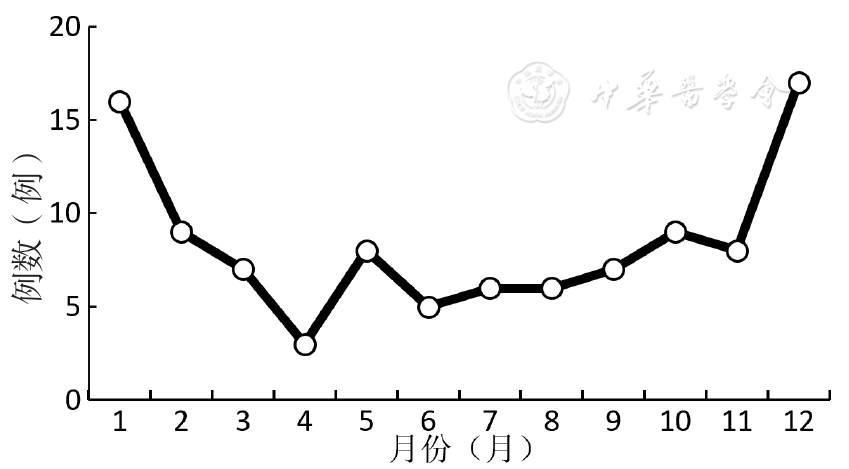
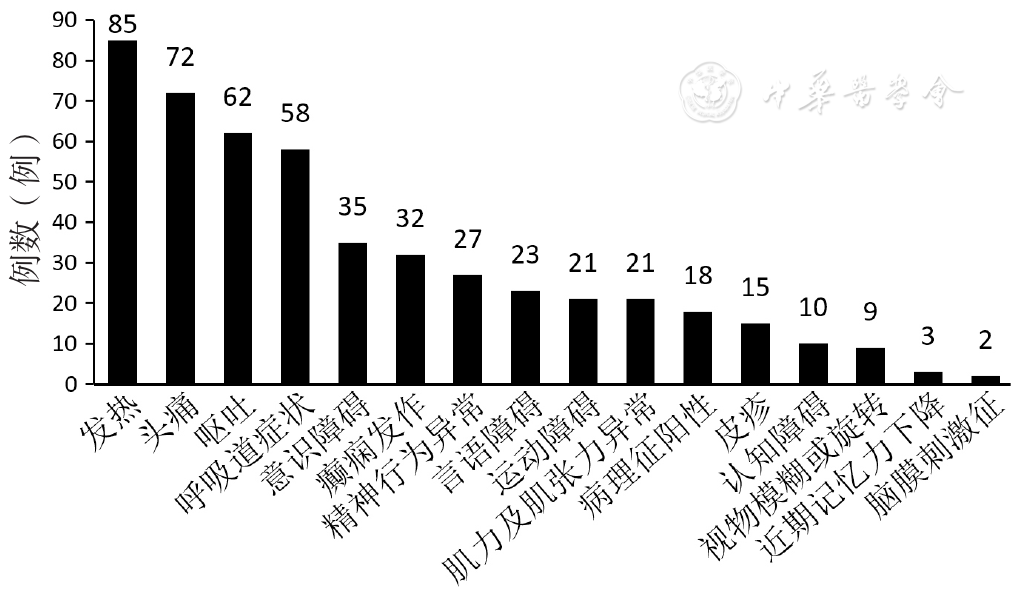
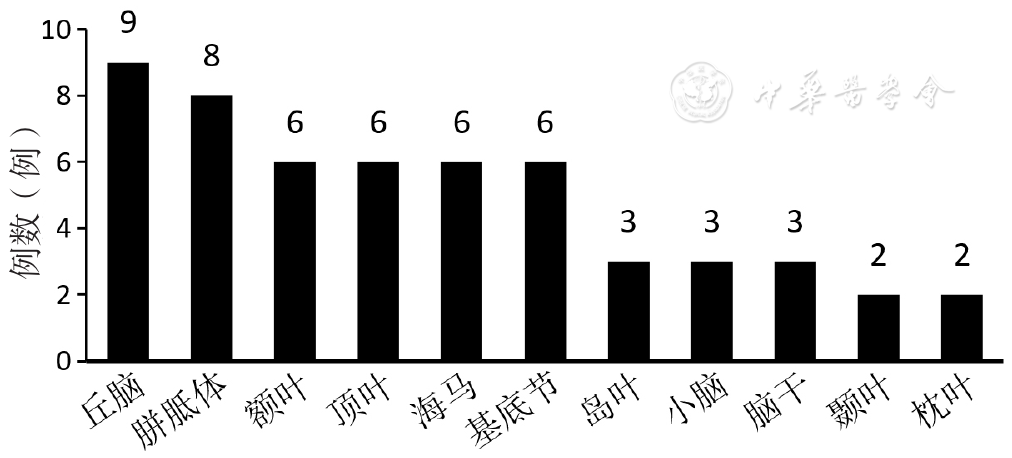
摘要: 背景 近年儿童肺炎支原体脑炎(MPIE)发病趋势有所增加,临床表现异质性和诊断手段局限性使得临床医生认识不足。 目的 分析儿童MPIE的临床特征并探讨患儿预后不良的独立危险因素,为降低MPIE神经后遗症的发生率和病死率提供理论依据。 方法 回顾性分析2020年1月至2022年6月于河北省儿童医院神经内科住院治疗的101例MPIE患儿的临床资料,采用格拉斯哥预后分级(GOS)评估患儿出院时情况,分为预后良好组(73例)和预后不良组(28例)。分析两组MPIE患儿的临床特征,包括一般资料(性别、年龄等)、临床症状及体征、辅助检查结果〔肺炎支原体(MP)、脑脊液、脑电图、影像学及免疫学等相关实验室检查指标〕及治疗情况并进行比较。采用多因素Logistic回归分析探讨儿童MPIE预后不良的独立危险因素。 结果 MPIE患儿预后良好率为72.3%(73/101),预后不良率为27.7%(28/101)。患儿多急性起病,学龄期儿童为主,全年散发,冬春季占比较高,最常见的症状是发热,神经系统表现以言语障碍和运动障碍等局灶性损害较多见,部分出现癫痫发作,甚至发展为难治性癫痫持续状态。脑脊液肺炎支原体-聚合酶链式反应阳性率为26.7%(27/101)。脑电图主要表现为背景节律的慢化,而颅脑磁共振成像(MRI)主要表现为受累部位的长T1、长T2信号,两者的异常率分别为68.3%(69/101)和44.6%(45/101)。结合细胞免疫和体液免疫指标以及部分患儿的血或脑脊液可检测到抗N-甲基-D-天冬氨酸受体、髓鞘少突胶质细胞糖蛋白等免疫性脑炎和脱髓鞘相关抗体。预后良好组与预后不良组患儿精神行为异常、意识障碍、癫痫发作、癫痫持续状态、局灶性神经功能障碍、脑脊液白细胞计数、脑电图异常、颅脑MRI异常、糖皮质激素治疗、丙种球蛋白治疗比较,差异有统计学意义(P<0.05)。多因素Logistic回归分析结果显示,局灶性神经系统功能障碍〔OR=6.292,95%CI(1.188,33.327),P=0.035〕、癫痫持续状态〔OR=18.031,95%CI(1.231,264.082),P=0.031〕、脑电图异常〔OR=7.379,95%CI(1.077,50.548),P=0.042〕、颅脑MRI异常〔OR=5.757,95%CI(1.105,30.003),P=0.038〕和需糖皮质激素治疗〔OR=12.441,95%CI(1.082,143.114),P=0.043〕是儿童MPIE预后不良的独立危险因素。 结论 局灶性神经系统功能障碍、癫痫持续状态、脑电图异常、颅脑MRI异常和需糖皮质激素治疗可能是儿童MPIE预后不良的独立危险因素,临床医师应高度重视,早期识别以降低儿童MPIE神经后遗症的发生率和病死率。