中国全科医学 ›› 2024, Vol. 27 ›› Issue (06): 679-684.DOI: 10.12114/j.issn.1007-9572.2023.0338
所属专题: 儿科最新文章合辑
郑奎1,2, 刘露3, 王永丽1,2, 李会1,2, 王璇1,2, 李博1, 郝京霞1, 张英谦1,*( )
)
ZHENG Kui1,2, LIU Lu3, WANG Yongli1,2, LI Hui1,2, WANG Xuan1,2, LI Bo1, HAO Jingxia1, ZHANG Yingqian1,*()
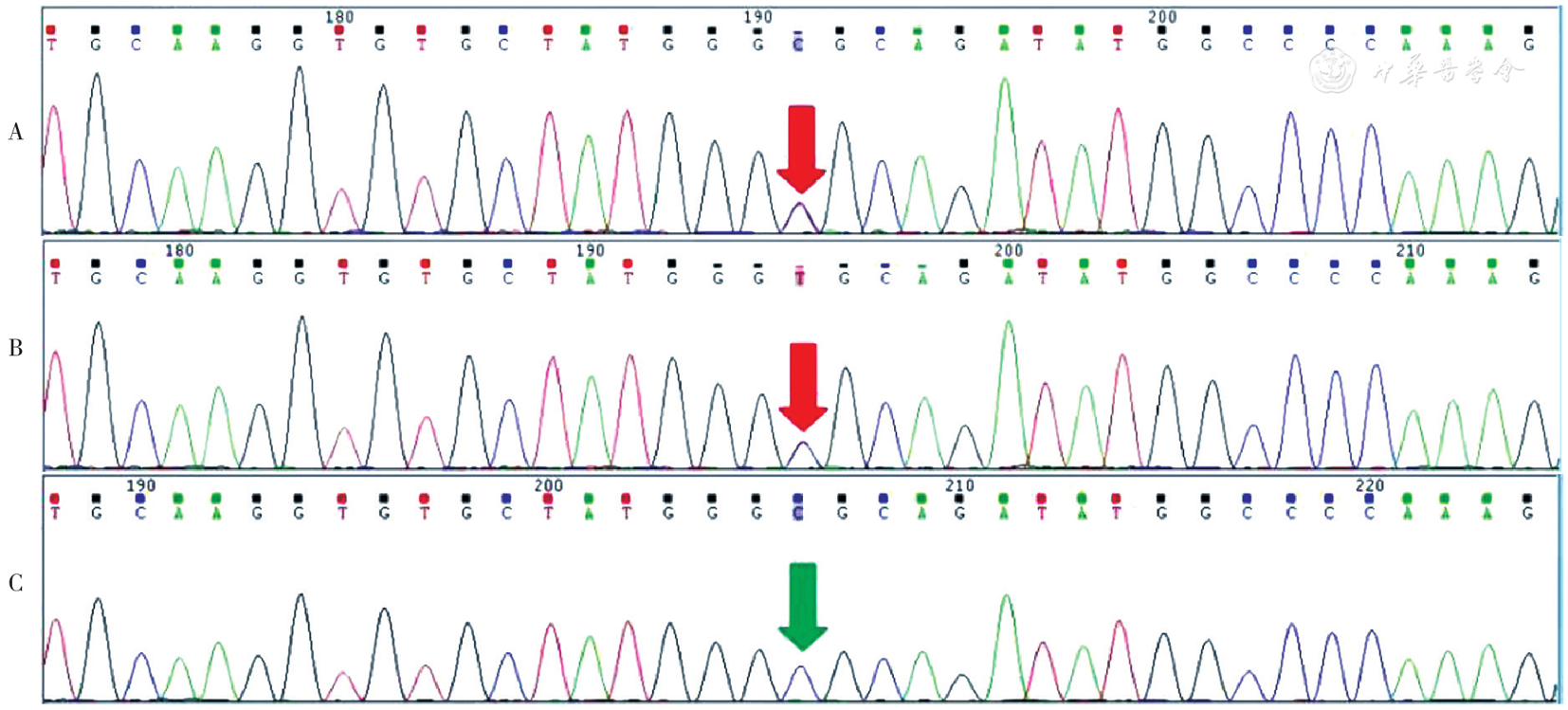
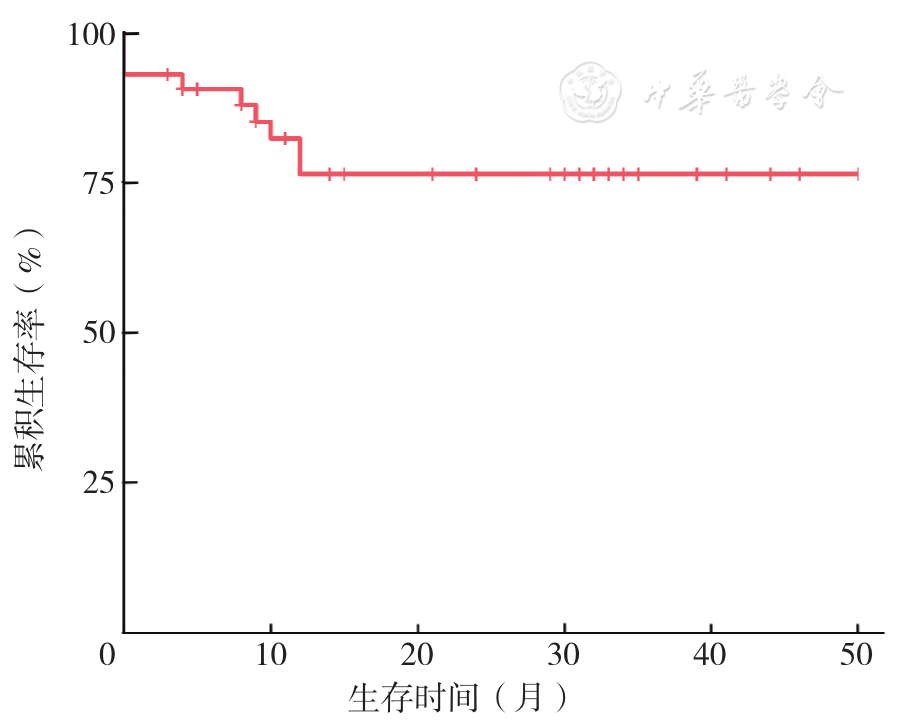
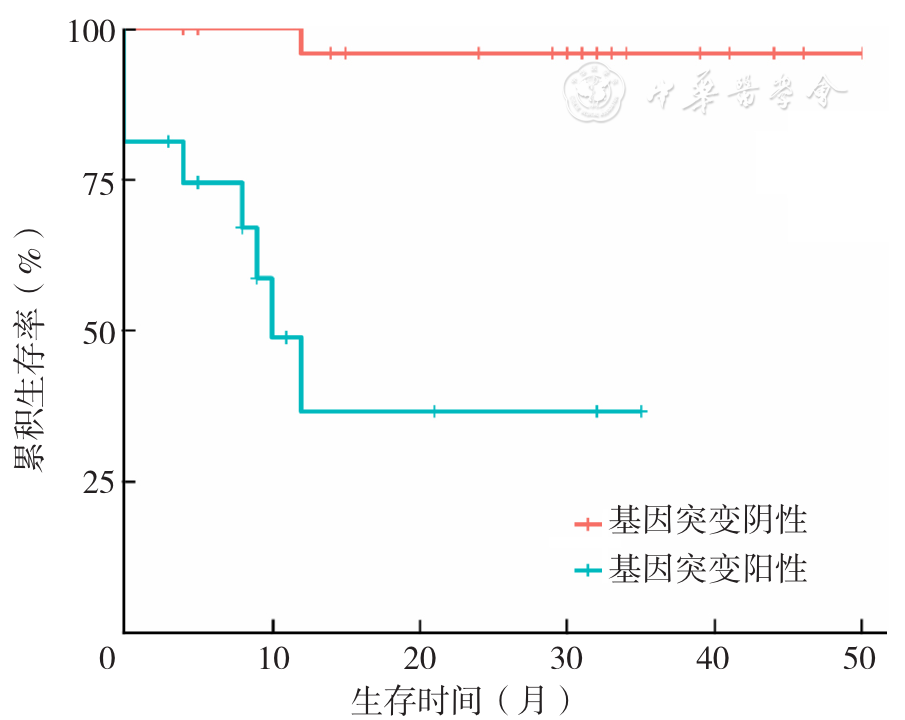
摘要: 背景 扩张型心肌病(DCM)是儿童心源性猝死和心力衰竭的常见原因之一,不同病因与DCM患儿的预后显著相关。其中原发性DCM的占比最高且预后相对较差,特别是与遗传因素相关的患儿预后更差。因此基于遗传背景下的死亡危险因素分析将有利于DCM患儿的精准预后评估及危险分层。 目的 探讨儿童原发性DCM的遗传病因占比、遗传学特征及死亡危险因素。 方法 回顾性纳入2018年7月—2022年12月在河北省儿童医院住院治疗并完成基因检测的42例原发性DCM患儿的临床资料,收集患儿的基因检测结果。出院后定期于河北省儿童医院心内科门诊随访。以患儿死亡时间或2022-12-31为随访终点,根据随访结局将患儿分为死亡组(9例)与存活组(33例)。采用Kaplan-Meier法绘制患儿的生存曲线,生存曲线比较采用Log-rank检验。采用多因素COX比例风险模型分析患儿死亡的危险因素。 结果 患儿中位首诊年龄12(7,96)个月,中位随访时间24(9,36)个月。死亡组患儿中位随访时间8(0,11)个月,存活组中位随访时间30(12,39)个月,差异有统计学意义(Z=-2.19,P<0.05)。死亡组患儿男性、心功能分级Ⅲ/Ⅳ级、基因突变阳性占比高于生存组,左心室短轴缩短率(LVFS)低于生存组(P<0.05)。患儿基因突变阳性率为38.1%(16/42),其中自发突变占25.0%(4/16),基因突变阴性为61.9%(26/42)。死亡组9例患儿均在诊断后1年内死亡。基因突变阳性患儿死亡8例(50.0%,8/16),基因突变阴性患儿死亡1例(3.8%,1/26),组间死亡率差异有统计学意义(P<0.05)。基因突变阴性死亡患儿CSRP3(c.190C>T)杂合变异,致病分类为临床意义未明。绘制患儿Kaplan-Meier生存曲线,Log-rank检验结果显示基因突变阴性患儿生存率高于基因突变阳性患儿(χ2=18.1,P<0.001)。多因素COX比例风险模型分析结果显示基因突变[HR=23.91,95%CI=(1.80~317.21),P=0.016]、心功能分级Ⅲ/Ⅳ级[HR=11.29,95%CI(1.13~112.68),P=0.039]为DCM患儿死亡的危险因素。 结论 本研究38.1%的原发性DCM患儿与遗传病因相关,诊断后第1年内是DCM患儿死亡的高发期,基因突变阳性的患儿预后更差。存在致病基因突变、首诊心功能分级Ⅲ/Ⅳ级是患儿死亡的独立危险因素。