
中国全科医学 ›› 2026, Vol. 29 ›› Issue (15): 1998-2005.DOI: 10.12114/j.issn.1007-9572.2025.0236
刘帆1, 陈秋雨2, 李婧3,*( )
)
收稿日期:2025-07-01
修回日期:2025-12-01
出版日期:2026-05-20
发布日期:2026-04-14
通讯作者:
李婧
刘帆与陈秋雨为共同第一作者
作者贡献:
刘帆负责论文数据搜集、论文撰写;陈秋雨负责论文格式、图表制作;李婧负责论文设计、撰写指导,对文章整体负责。
基金资助:
LIU Fan1, CHEN Qiuyu2, LI Jing3,*()
Received:2025-07-01
Revised:2025-12-01
Published:2026-05-20
Online:2026-04-14
Contact:
LI Jing
About author:LIU Fan and CHEN Qiuyu are co-first authors
摘要: 背景 夜间高血压(NH)是心脑肾等多器官损伤的重要因素,为全因死亡的预测因子,其预测价值高于日间血压及诊室血压,因其在夜间睡眠中发生的隐蔽特点被归为隐匿性高血压的一种,早日筛查并给予个体化治疗能够降低心脑肾疾病的患病风险。 目的 基于常规体检的实验室检查指标、个人健康资料探究NH患者的相关危险因素,建立NH的临床预测Nomogram模型。 方法 纳入2021-01-01—2024-06-30于内蒙古医科大学附属医院就诊的完善24 h动态血压监测的406例患者为研究对象,收集患者临床基线资料、实验室检查结果、心脏超声结果,进行动态血压监测。将患者按7∶3比例随机划分为训练集(n=284)和验证集(n=122)。采用LASSO回归分析与多因素Logistic回归分析构建NH风险预测模型并绘制列线图,绘制ROC曲线,计算ROC曲线下面积(AUC)验证预测模型的准确性。绘制校准曲线衡量模型的预测能力,反映预测风险与实际风险的一致性。 结果 依据24 h动态血压监测结果将患者分为NH组(n=254)和非NH组(n=152)。以LASSO回归分析筛选出的4个预测变量[体质量、总胆固醇(TC)、高血压、脑卒中]为自变量进行多因素Logistic回归分析,结果显示,体质量增大(OR=1.029,95%CI=1.006~1.053)、TC升高(OR=1.496,95%CI=1.136~1.972)、高血压(OR=2.372,95%CI=1.214~4.632)、脑卒中(OR=7.850,95%CI=4.157~14.824)均为NH的危险因素(P<0.05)。绘制列线图,脑卒中(得分0或62)和高血压(得分0或26)对诊断率的影响显著高于体质量和TC(得分随变量值线性变化),模型满分240分,当得分超过176分时,NH的风险为95%。绘制ROC曲线对上述预测模型进行评价,训练集AUC为0.791(95%CI=0.739~0.843),灵敏度为0.698,特异度为0.786;验证集AUC为0.820(95%CI=0.742~0.899),灵敏度为0.817,特异度为0.725。Hosmer-Lemeshow校准曲线显示模型拟合度较好,决策曲线分析结果显示验证集在阈值概率范围为0.2~0.6表现出较高的净收益,具有最佳的临床实用性。 结论 本研究建立了包含体质量、TC、高血压、脑卒中4项临床指标的NH风险预测模型,可用于预测筛查疑似患者的NH发生风险,模型具有良好的拟合度、区分度和临床应用价值。
| 组别 | 例数 | 年龄[M(P25,P75),岁] | 体质量[M(P25,P75),kg] | Cr[M(P25,P75),μmol/L] | Hcy[M(P25,P75),μmol/L] | LPA[M(P25,P75),g/L] | TC[M(P25,P75),mmol/L] | LDL-C[M(P25,P75),mmol/L] | G[M(P25,P75),mmol/L] | |
|---|---|---|---|---|---|---|---|---|---|---|
| 非NH组 | 152 | 64(58,70) | 68(60,77) | 64(55,77) | 13.38(10.63,17.25) | 0.14(0.07,0.25) | 4.09(3.31,4.49) | 2.32(1.71,2.94) | 4.93(4.60,5.66) | |
| NH组 | 254 | 63(54,69) | 70(64,80) | 62(55,74) | 14.42(11.04,18.34) | 0.15(0.08,0.30) | 4.42(3.60,5.22) | 2.50(1.97,3.15) | 5.16(4.47,7.12) | |
| Z(χ2)值 | -1.874 | 3.380 | -1.066 | 2.157 | 2.142 | 3.315 | 2.730 | 1.144 | ||
| P值 | 0.061 | <0.001 | 0.286 | 0.031 | 0.032 | <0.001 | 0.006 | 0.150 | ||
| 组别 | TG[M(P25,P75),mmol/L] | UA[M(P25,P75),μmol/L] | HDL-C[M(P25,P75),mmol/L] | WBC[M(P25,P75),×109/L] | NEUT[M(P25,P75),×109/L] | LYM[M(P25,P75),×109/L] | 高血压病史[M(P25,P75),年] | LA[M(P25,P75),mm] | IVS[M(P25,P75),mm] | |
| 非NH组 | 1.40(0.98,1.67) | 327.0(260.8,405.0) | 1.04(0.88,1.20) | 5.99(4.97,7.17) | 3.42(2.86,4.31) | 1.89(1.58,2.32) | 7(0,15) | 34(32,38) | 9(9,10) | |
| NH组 | 1.41(1.05,2.08) | 333.5(265.8,422.0) | 1.03(0.88,1.20) | 6.51(5.34,7.57) | 3.91(2.95,4.71) | 1.77(1.43,2.26) | 10(2,20) | 35(32,38) | 9(9,10) | |
| Z(χ2)值 | 1.691 | 1.063 | -0.626 | 1.428 | 1.730 | -0.093 | 4.089 | 1.290 | 2.029 | |
| P值 | 0.091 | 0.288 | 0.531 | 0.153 | 0.084 | 0.926 | <0.001 | 0.197 | 0.042 | |
| 组别 | EF[M(P25,P75),%] | PWTd[M(P25,P75),mm] | LVEDD[M(P25,P75),mm] | 性别(男/女) | 高血压[例(%)] | 糖尿病[例(%)] | 冠心病[例(%)] | 植入支架[例(%)] | 吸烟史[例(%)] | 脑卒中[例(%)] |
| 非NH组 | 65(60,70) | 9(8,9) | 46(42,48) | 67/85 | 107(70.4) | 39(25.7) | 65(42.8) | 40(26.5) | 42(27.8) | 20(13.2) |
| NH组 | 64(61,69) | 9(8,10) | 47(44,49) | 147/107 | 217(85.4) | 78(30.7) | 80(31.5) | 39(15.4) | 90(35.4) | 139(54.7) |
| Z(χ2)值 | 0.099 | 1.650 | 2.314 | 7.260a | 13.343a | 1.183a | 5.258a | 7.479a | 2.502a | 68.328a |
| P值 | 0.921 | 0.099 | 0.021 | 0.007 | <0.001 | 0.277 | 0.022 | 0.006 | 0.114 | <0.001 |
表1 非NH组与NH组患者基线资料比较
Table 1 Comparison of baseline data between non-NH group and NH group
| 组别 | 例数 | 年龄[M(P25,P75),岁] | 体质量[M(P25,P75),kg] | Cr[M(P25,P75),μmol/L] | Hcy[M(P25,P75),μmol/L] | LPA[M(P25,P75),g/L] | TC[M(P25,P75),mmol/L] | LDL-C[M(P25,P75),mmol/L] | G[M(P25,P75),mmol/L] | |
|---|---|---|---|---|---|---|---|---|---|---|
| 非NH组 | 152 | 64(58,70) | 68(60,77) | 64(55,77) | 13.38(10.63,17.25) | 0.14(0.07,0.25) | 4.09(3.31,4.49) | 2.32(1.71,2.94) | 4.93(4.60,5.66) | |
| NH组 | 254 | 63(54,69) | 70(64,80) | 62(55,74) | 14.42(11.04,18.34) | 0.15(0.08,0.30) | 4.42(3.60,5.22) | 2.50(1.97,3.15) | 5.16(4.47,7.12) | |
| Z(χ2)值 | -1.874 | 3.380 | -1.066 | 2.157 | 2.142 | 3.315 | 2.730 | 1.144 | ||
| P值 | 0.061 | <0.001 | 0.286 | 0.031 | 0.032 | <0.001 | 0.006 | 0.150 | ||
| 组别 | TG[M(P25,P75),mmol/L] | UA[M(P25,P75),μmol/L] | HDL-C[M(P25,P75),mmol/L] | WBC[M(P25,P75),×109/L] | NEUT[M(P25,P75),×109/L] | LYM[M(P25,P75),×109/L] | 高血压病史[M(P25,P75),年] | LA[M(P25,P75),mm] | IVS[M(P25,P75),mm] | |
| 非NH组 | 1.40(0.98,1.67) | 327.0(260.8,405.0) | 1.04(0.88,1.20) | 5.99(4.97,7.17) | 3.42(2.86,4.31) | 1.89(1.58,2.32) | 7(0,15) | 34(32,38) | 9(9,10) | |
| NH组 | 1.41(1.05,2.08) | 333.5(265.8,422.0) | 1.03(0.88,1.20) | 6.51(5.34,7.57) | 3.91(2.95,4.71) | 1.77(1.43,2.26) | 10(2,20) | 35(32,38) | 9(9,10) | |
| Z(χ2)值 | 1.691 | 1.063 | -0.626 | 1.428 | 1.730 | -0.093 | 4.089 | 1.290 | 2.029 | |
| P值 | 0.091 | 0.288 | 0.531 | 0.153 | 0.084 | 0.926 | <0.001 | 0.197 | 0.042 | |
| 组别 | EF[M(P25,P75),%] | PWTd[M(P25,P75),mm] | LVEDD[M(P25,P75),mm] | 性别(男/女) | 高血压[例(%)] | 糖尿病[例(%)] | 冠心病[例(%)] | 植入支架[例(%)] | 吸烟史[例(%)] | 脑卒中[例(%)] |
| 非NH组 | 65(60,70) | 9(8,9) | 46(42,48) | 67/85 | 107(70.4) | 39(25.7) | 65(42.8) | 40(26.5) | 42(27.8) | 20(13.2) |
| NH组 | 64(61,69) | 9(8,10) | 47(44,49) | 147/107 | 217(85.4) | 78(30.7) | 80(31.5) | 39(15.4) | 90(35.4) | 139(54.7) |
| Z(χ2)值 | 0.099 | 1.650 | 2.314 | 7.260a | 13.343a | 1.183a | 5.258a | 7.479a | 2.502a | 68.328a |
| P值 | 0.921 | 0.099 | 0.021 | 0.007 | <0.001 | 0.277 | 0.022 | 0.006 | 0.114 | <0.001 |
| 组别 | 例数 | 年龄[M(P25,P75),岁] | 体质量[M(P25,P75),kg] | Cr[M(P25,P75),μmol/L] | Hcy[M(P25,P75),μmol/L] | LPA[M(P25,P75),g/L] | TC[M(P25,P75),mmol/L] | LDL-C[M(P25,P75),mmol/L] | G[M(P25,P75),mmol/L] | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 训练集 | 284 | 63(55,70) | 70.0(62.0,78.0) | 64(56,76) | 13.31(10.61,17.32) | 0.15(0.08,0.27) | 4.38(3.57,5.06) | 2.48(1.94,3.11) | 5.04(4.46,6.49) | ||
| 验证集 | 122 | 64(58,68) | 70.0(62.0,78.5) | 63(53,74) | 15.02(11.46,20.72) | 0.13(0.08,0.30) | 3.94(3.34,4.77) | 2.34(1.70,2.82) | 5.13(4.50,6.25) | ||
| Z(χ2)值 | -0.516 | -1.260 | -1.027 | -2.624 | -0.137 | -2.505 | -2.176 | -0.006 | |||
| P值 | 0.606 | 0.208 | 0.304 | 0.009 | 0.891 | 0.012 | 0.030 | 0.996 | |||
| 组别 | TG[M(P25,P75),mmol/L] | UA[M(P25,P75),μmol/L] | HDL-C[M(P25,P75),mmol/L] | WBC[M(P25,P75),×109/L] | NEUT[M(P25,P75),×109/L] | LYM[M(P25,P75),×109/L] | 高血压[M(P25,P75),年] | LA[M(P25,P75),mm] | IVS[M(P25,P75),mm] | ||
| 训练集 | 1.40(1.03,2.00) | 329.0(260.0,405.0) | 1.05(0.90,1.21) | 6.33(5.37,7.35) | 3.82(3.06,4.66) | 1.78(1.44,2.23) | 7(1,16) | 35(32,38) | 9(9,10) | ||
| 验证集 | 1.42(0.99,1.86) | 335.0(268.0,422.0) | 1.03(0.88,1.19) | 6.13(5.27,7.46) | 3.67(2.93,4.51) | 1.77(1.51,2.20) | 9(1,15) | 35(33,39) | 9(8,10) | ||
| Z(χ2)值 | -0.812 | -0.701 | -1.168 | -0.720 | -1.160 | -0.442 | -0.433 | -1.278 | -0.252 | ||
| P值 | 0.417 | 0.484 | 0.243 | 0.472 | 0.246 | 0.695 | 0.665 | 0.201 | 0.801 | ||
| 组别 | EF[M(P25,P75),%] | PWTd[M(P25,P75),mm] | LVEDD[M(P25,P75),mm] | NH[例(%)] | 性别(男/女) | 高血压[例(%)] | 糖尿病[例(%)] | 冠心病[例(%)] | 植入支架[例(%)] | 吸烟史[例(%)] | 脑卒中[例(%)] |
| 训练集 | 65(61,69) | 9(8,10) | 46(43,49) | 172(60.6) | 142/142 | 224(78.9) | 81(28.5) | 97(34.2) | 57(20.1) | 85(29.9) | 112(39.4) |
| 验证集 | 64(60,68) | 9(8,10) | 46(43,49) | 82(67.2) | 72/50 | 100(82.0) | 36(29.5) | 48(39.3) | 22(18.0) | 47(38.5) | 47(38.5) |
| Z(χ2)值 | -1.041 | -0.049 | -0.045 | 1.611a | 2.783a | 0.507a | 0.041a | 1.001a | 0.226a | 2.873a | 0.030a |
| P值 | 0.298 | 0.961 | 0.964 | 0.204 | 0.095 | 0.477 | 0.840 | 0.317 | 0.634 | 0.090 | 0.863 |
表2 训练集与验证集患者基线资料比较
Table 2 Comparison results of baseline data between training group and the validation group
| 组别 | 例数 | 年龄[M(P25,P75),岁] | 体质量[M(P25,P75),kg] | Cr[M(P25,P75),μmol/L] | Hcy[M(P25,P75),μmol/L] | LPA[M(P25,P75),g/L] | TC[M(P25,P75),mmol/L] | LDL-C[M(P25,P75),mmol/L] | G[M(P25,P75),mmol/L] | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 训练集 | 284 | 63(55,70) | 70.0(62.0,78.0) | 64(56,76) | 13.31(10.61,17.32) | 0.15(0.08,0.27) | 4.38(3.57,5.06) | 2.48(1.94,3.11) | 5.04(4.46,6.49) | ||
| 验证集 | 122 | 64(58,68) | 70.0(62.0,78.5) | 63(53,74) | 15.02(11.46,20.72) | 0.13(0.08,0.30) | 3.94(3.34,4.77) | 2.34(1.70,2.82) | 5.13(4.50,6.25) | ||
| Z(χ2)值 | -0.516 | -1.260 | -1.027 | -2.624 | -0.137 | -2.505 | -2.176 | -0.006 | |||
| P值 | 0.606 | 0.208 | 0.304 | 0.009 | 0.891 | 0.012 | 0.030 | 0.996 | |||
| 组别 | TG[M(P25,P75),mmol/L] | UA[M(P25,P75),μmol/L] | HDL-C[M(P25,P75),mmol/L] | WBC[M(P25,P75),×109/L] | NEUT[M(P25,P75),×109/L] | LYM[M(P25,P75),×109/L] | 高血压[M(P25,P75),年] | LA[M(P25,P75),mm] | IVS[M(P25,P75),mm] | ||
| 训练集 | 1.40(1.03,2.00) | 329.0(260.0,405.0) | 1.05(0.90,1.21) | 6.33(5.37,7.35) | 3.82(3.06,4.66) | 1.78(1.44,2.23) | 7(1,16) | 35(32,38) | 9(9,10) | ||
| 验证集 | 1.42(0.99,1.86) | 335.0(268.0,422.0) | 1.03(0.88,1.19) | 6.13(5.27,7.46) | 3.67(2.93,4.51) | 1.77(1.51,2.20) | 9(1,15) | 35(33,39) | 9(8,10) | ||
| Z(χ2)值 | -0.812 | -0.701 | -1.168 | -0.720 | -1.160 | -0.442 | -0.433 | -1.278 | -0.252 | ||
| P值 | 0.417 | 0.484 | 0.243 | 0.472 | 0.246 | 0.695 | 0.665 | 0.201 | 0.801 | ||
| 组别 | EF[M(P25,P75),%] | PWTd[M(P25,P75),mm] | LVEDD[M(P25,P75),mm] | NH[例(%)] | 性别(男/女) | 高血压[例(%)] | 糖尿病[例(%)] | 冠心病[例(%)] | 植入支架[例(%)] | 吸烟史[例(%)] | 脑卒中[例(%)] |
| 训练集 | 65(61,69) | 9(8,10) | 46(43,49) | 172(60.6) | 142/142 | 224(78.9) | 81(28.5) | 97(34.2) | 57(20.1) | 85(29.9) | 112(39.4) |
| 验证集 | 64(60,68) | 9(8,10) | 46(43,49) | 82(67.2) | 72/50 | 100(82.0) | 36(29.5) | 48(39.3) | 22(18.0) | 47(38.5) | 47(38.5) |
| Z(χ2)值 | -1.041 | -0.049 | -0.045 | 1.611a | 2.783a | 0.507a | 0.041a | 1.001a | 0.226a | 2.873a | 0.030a |
| P值 | 0.298 | 0.961 | 0.964 | 0.204 | 0.095 | 0.477 | 0.840 | 0.317 | 0.634 | 0.090 | 0.863 |
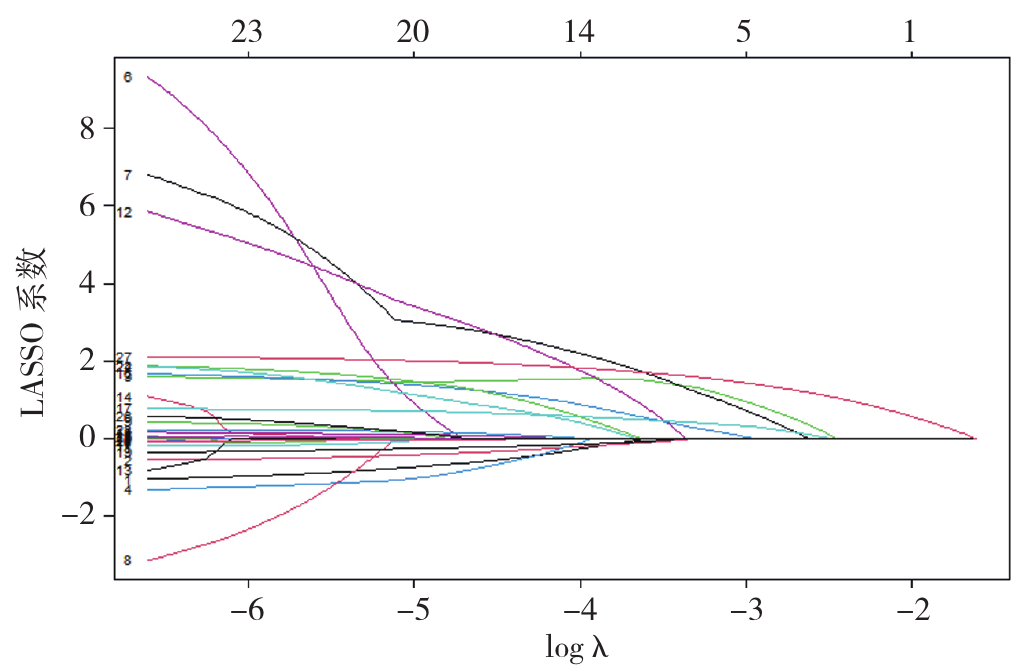
图1 LASSO系数曲线
Figure 1 LASSO coefficient curve
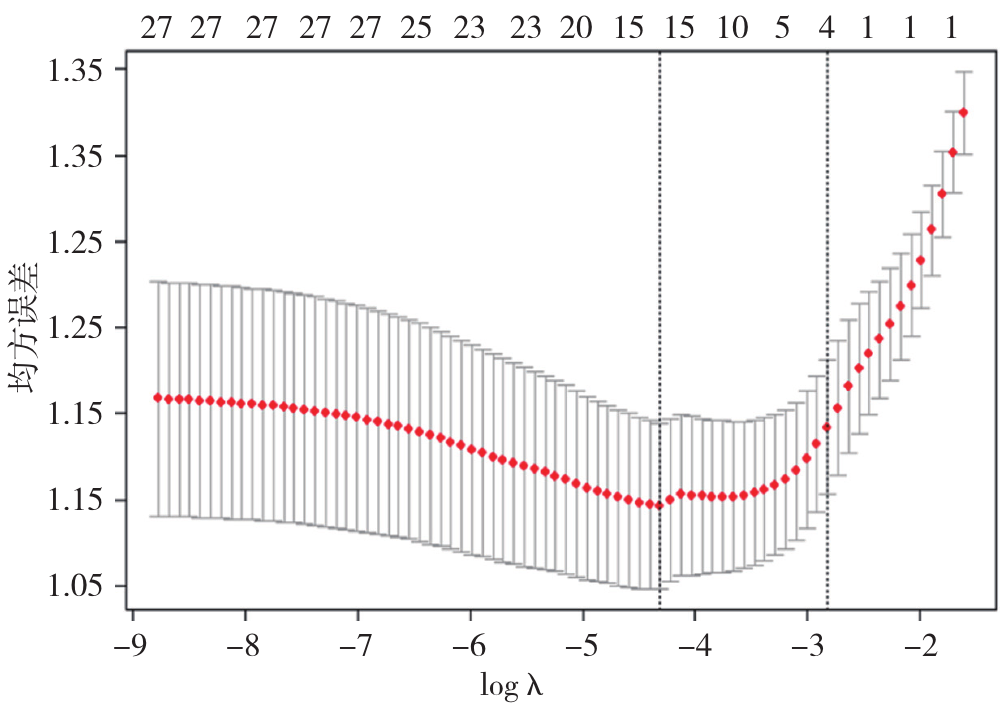
图2 LASSO回归分析交叉验证
Figure 2 LASSO regression cross-validation
| 预测变量 | B | SE | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 体质量 | 0.029 | 0.012 | 5.912 | 0.015 | 1.029(1.006~1.053) |
| TC | 0.403 | 0.141 | 8.197 | 0.004 | 1.496(1.136~1.972) |
| 高血压 | 0.864 | 0.341 | 6.395 | 0.011 | 2.372(1.214~4.632) |
| 脑卒中 | 2.060 | 0.324 | 40.352 | <0.001 | 7.850(4.157~14.824) |
表3 发生NH影响因素的多因素Logistic回归分析
Table 3 Multivariate Logistic regression analysis of factors influencing in patients with NH
| 预测变量 | B | SE | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 体质量 | 0.029 | 0.012 | 5.912 | 0.015 | 1.029(1.006~1.053) |
| TC | 0.403 | 0.141 | 8.197 | 0.004 | 1.496(1.136~1.972) |
| 高血压 | 0.864 | 0.341 | 6.395 | 0.011 | 2.372(1.214~4.632) |
| 脑卒中 | 2.060 | 0.324 | 40.352 | <0.001 | 7.850(4.157~14.824) |
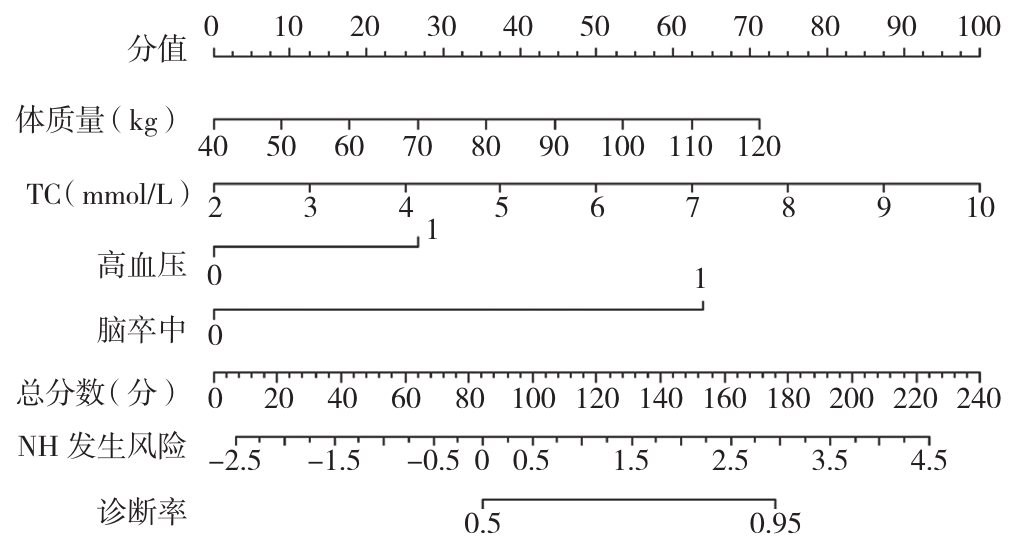
图3 NH患者风险预测模型的列线图注:TC=总胆固醇,NH=夜间高血压。
Figure 3 Nomogram of the risk prediction model forpatients with NH
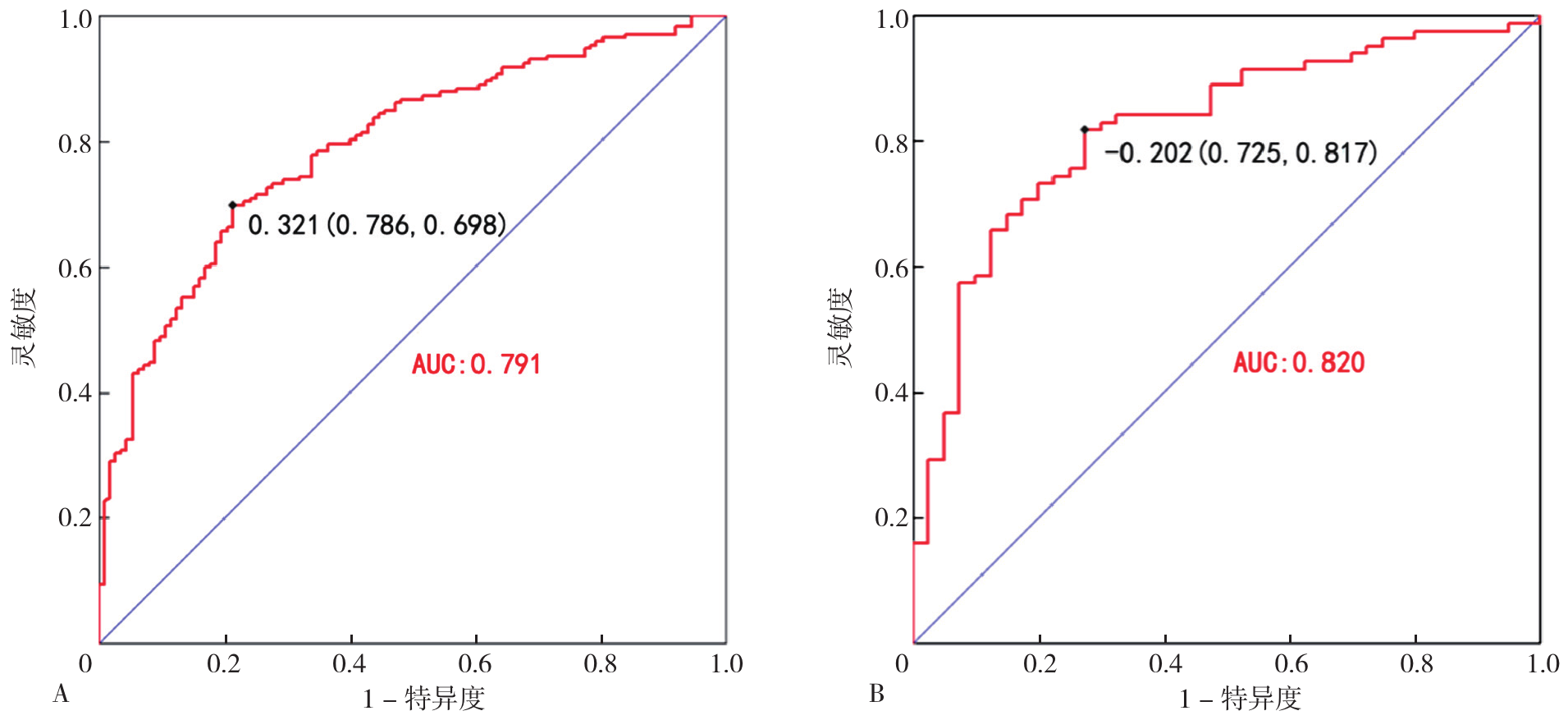
图4 预测模型的受试者工作特征曲线注:A为训练集,B为验证集;AUC=受试者工作特征曲线下面积。
Figure 4 Receiver operating characteristic curve of the prediction model
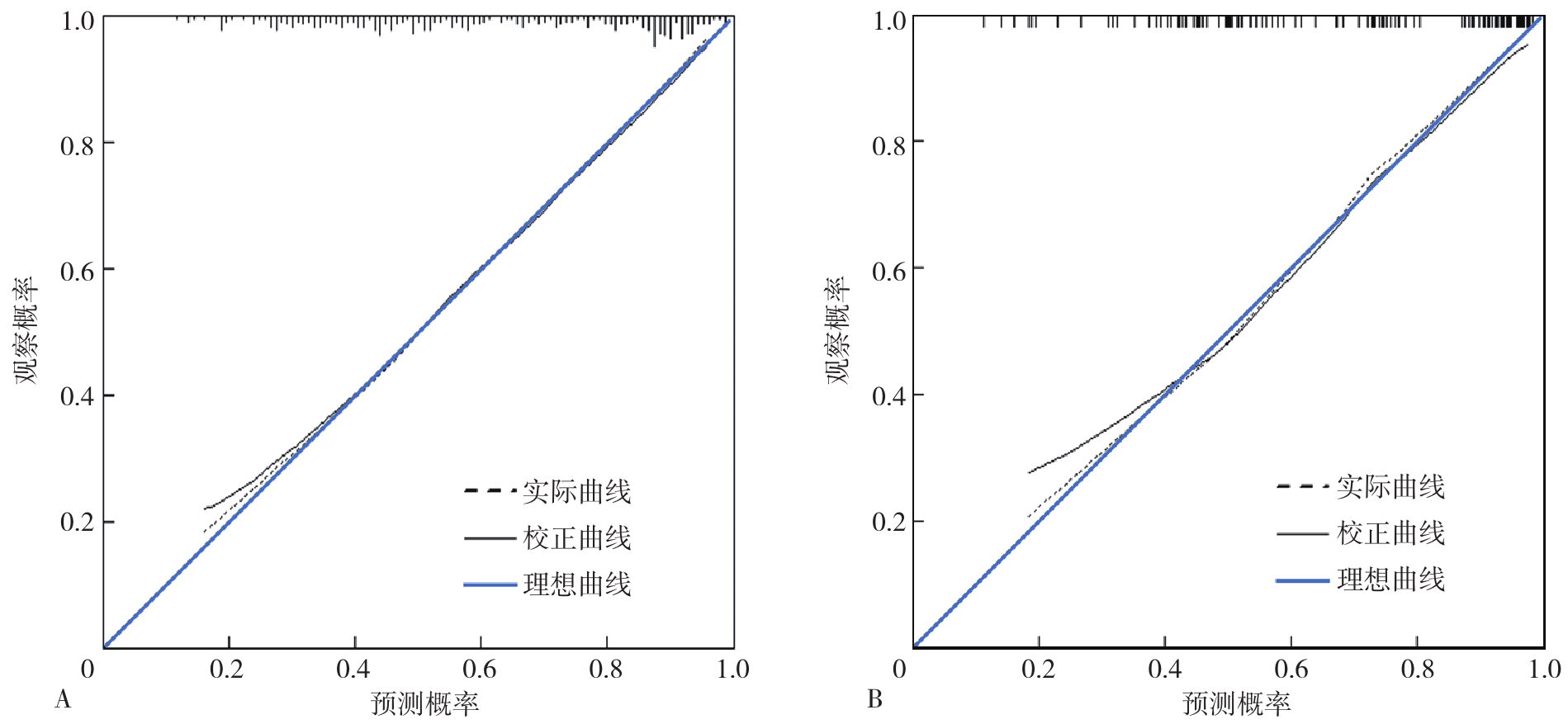
图5 预测模型的校准曲线注:A为训练集,B为验证集。
Figure 5 Calibration curve of the predictive model
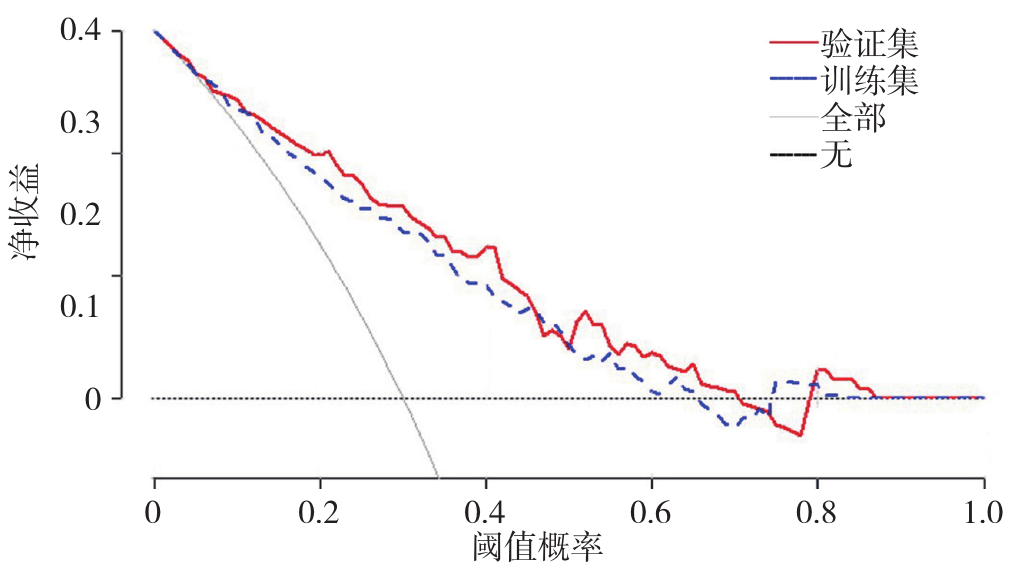
图6 预测模型的决策曲线分析
Figure 6 Decision curve analysis of the predictive model
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
Asleep blood pressure: significant prognostic marker of vascular risk and therapeutic target for prevention | European Heart Journal | Oxford Academic[EB/OL].[2025-06-26].
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
Obesity and Hypertension Induced Sleep Apnea in Men[EB/OL].[2025-06-26].
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
Artificial intelligence-enhanced electrocardiography derived body mass index as a predictor of future cardiometabolic disease | npj Digital Medicine[EB/OL].[2025-06-26].
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
The cardiovascular system's Renin-Angiotensin-Aldosterone System (RAAS)[EB/OL].[2025-06-26].
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [1] | 郑仁阔, 华飞. 代谢相关脂肪性肝病与甲状腺乳头状癌的相关性研究[J]. 中国全科医学, 2026, 29(15): 2029-2036. |
| [2] | 邱欣雨, 赵倩, 陈玉斐, 加木勒·买买提依明, 韩聪聪, 爱克丹·艾尔肯, 李晓梅, 杨毅宁. 体重状态及其代谢特征对收缩压纵向轨迹的影响:一项队列研究[J]. 中国全科医学, 2026, 29(15): 2006-2013. |
| [3] | 刘天缘, 桑婉玥, 彭继平, 程思怡, 黄伊伊, 李欧文, 江洪, 周晓亚. 神经丝轻链蛋白与夜间高血压患者左心室肥厚发生风险的相关性研究[J]. 中国全科医学, 2026, 29(15): 2014-2021. |
| [4] | 王斯曼, 张梦楚, 李文, 许艾, 徐璡, 郭睿, 燕海霞. 基于中医证候及脉图参数构建原发性高血压伴左心室肥厚风险预测模型研究[J]. 中国全科医学, 2026, 29(14): 1840-1848. |
| [5] | 吴春香, 田婕, 郭毅, 邓波, 于杰, 蔡宁, 沈莉. 高血压患者8年就医行为轨迹及影响因素分析[J]. 中国全科医学, 2026, 29(13): 1660-1665. |
| [6] | 胡嘉琦, 李端, 方昊, 樊兴颖, 杜薇, 周涵妮. 基于体检人群队列的高尿酸血症非遗传因素风险预测模型构建研究[J]. 中国全科医学, 2026, 29(10): 1324-1333. |
| [7] | 宋路, 王丽晔, 修春霞, 冯宝静, 冯丽萍, 高艳松, 李梦, 代妍. 慢性阻塞性肺疾病合并高血压患者肺功能与血压变异性的相关研究[J]. 中国全科医学, 2026, 29(10): 1311-1315. |
| [8] | 焦玺同, 刘璐, 郭嘉悦, 尤莉莉. 国内外高血压数字疗法产品的应用前景及对我国的启示[J]. 中国全科医学, 2026, 29(10): 1354-1360. |
| [9] | 余新艳, 马忠, 曹凡, 苏鹏, 林颖, 张海澄. 基于单导联可穿戴心电设备预测基层老年心血管代谢疾病患者抑郁发生风险的研究[J]. 中国全科医学, 2026, 29(10): 1300-1310. |
| [10] | 张秋雨, 胡晓咏, 唐瑞, 李红建. 中国人内脏脂肪指数与中青年夜间高血压的相关性研究[J]. 中国全科医学, 2026, 29(07): 872-878. |
| [11] | 张彦景, 周春华, 李晓东, 刘琰, 王婧, 于静. 文拉法辛血药浓度超警戒值风险预测模型的临床价值研究[J]. 中国全科医学, 2026, 29(06): 777-782. |
| [12] | 李杰, 杨昕晖, 曹黎, 张晶, 姜岳. 一例"三高"合并脂肪性肝病患者的全科诊疗案例分析[J]. 中国全科医学, 2026, 29(06): 810-816. |
| [13] | 雷莹莹, 郑锶颖, 汪文新, 姜虹. 1990—2021年全球及中国高血压心脏病流行趋势及预测研究[J]. 中国全科医学, 2026, 29(05): 641-648. |
| [14] | 江晓蕊, 闫玉瑶, 卫靖靖, 乔利杰, 彭广操, 朱明军. 冠心病患者并发心力衰竭风险预测模型的系统评价[J]. 中国全科医学, 2026, 29(03): 393-402. |
| [15] | 周文超, 梁佳琪, 姚尚满, 薛朝, 刘龙, 郭相杰. 高血压与帕金森病的共享基因位点识别研究[J]. 中国全科医学, 2026, 29(02): 201-206. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










