
中国全科医学 ›› 2026, Vol. 29 ›› Issue (14): 1840-1848.DOI: 10.12114/j.issn.1007-9572.2025.0397
• 论著 • 上一篇
王斯曼, 张梦楚, 李文, 许艾, 徐璡, 郭睿, 燕海霞*( )
)
收稿日期:2025-07-18
修回日期:2026-01-25
出版日期:2026-05-15
发布日期:2026-04-14
通讯作者:
燕海霞
作者贡献:
王斯曼负责数据分析、论文撰写及修改;张梦楚负责数据整理及分析;李文、许艾负责数据收集;徐璡、郭睿负责研究思路指导;燕海霞负责研究设计构思、思路指导、数据整体分析及论文修改指导。
基金资助:
WANG Siman, ZHANG Mengchu, LI Wen, XU Ai, XU Jin, GUO Rui, YAN Haixia*()
Received:2025-07-18
Revised:2026-01-25
Published:2026-05-15
Online:2026-04-14
Contact:
YAN Haixia
摘要: 背景 原发性高血压伴左心室肥厚(EH-LVH)的早期风险评估对临床干预至关重要,但现有预测模型常忽视中医证候、脉图参数等中医临床信息。因此,整合上述特色指标构建EH-LVH风险预测模型,将为中西医结合的风险分层与临床决策提供新依据。 目的 基于中医证候和脉图参数构建EH-LVH风险预测列线图模型。 方法 选取2018年8月—2021年6月上海市中医医院、上海中医药大学附属上海市中西医结合医院、上海中医药大学附属曙光医院收治的201例原发性高血压住院患者,根据超声心动图结果将其分为原发性高血压伴左心室肥厚组(EH-LVH组)和原发性高血压无左心室肥厚组(EH-NLVH组)。收集两组患者一般资料、理化指标及中医问诊信息,通过SMART-Ⅰ型中医脉象分析仪检测脉图参数。采用多因素Logistic回归分析探讨与EH-LVH发生风险存在独立关联的因素。应用R软件4.1.1rms程序包,分别以脉图参数、中医证候、脉图参数+中医证候+一般资料为变量,建立3个列线图模型(依次为模型A、B、C),以受试者工作特征(ROC)曲线分析区分度,校正曲线评估准确度,Hosmer-Lemeshow检验验证校准度,临床决策曲线(DCA曲线)评价临床实用性,并进行模型比较。 结果 多因素Logistic回归分析结果显示,低密度脂蛋白胆固醇(OR=1.511,95%CI=1.709~2.115)、阴虚阳亢证(OR=2.493,95%CI=1.272~4.885)、气滞血瘀证(OR=7.866,95%CI=2.201~28.110)、T(OR=1.906,95%CI=1.278~2.842)、H3/H1(OR=1.549,95%CI=1.021~2.351)、W1/T(OR=2.129,95%CI=1.369~3.310)是与EH-LVH风险独立相关的影响因素(P<0.01)。列线图模型的ROC曲线下面积(AUC)分别为:模型A的AUC为0.642(95%CI=0.571~0.713),模型B的AUC为0.717(95%CI=0.646~0.788),模型C的AUC为0.784(95%CI=0.719~0.849)。校准度结果显示,模型A:χ2=0.133(P>0.05),模型B:χ2=4.316(P>0.05),模型C:χ2=3.754(P>0.05),提示3个模型校准曲线的预测概率与实际概率一致性良好。DCA曲线分析显示,当预测EH-LVH发生的阈值处于0.05~0.80(估算值)时,模型C的适用性达到最优,表明该模型的临床实用价值更为显著。 结论 本研究以中医证候及脉图参数为核心预测变量,成功构建EH-LVH风险预测列线图。该列线图的区分效能与预测精准度经验证表现良好,具备临床推广应用价值,可作为临床开展该疾病风险评估的参考依据。
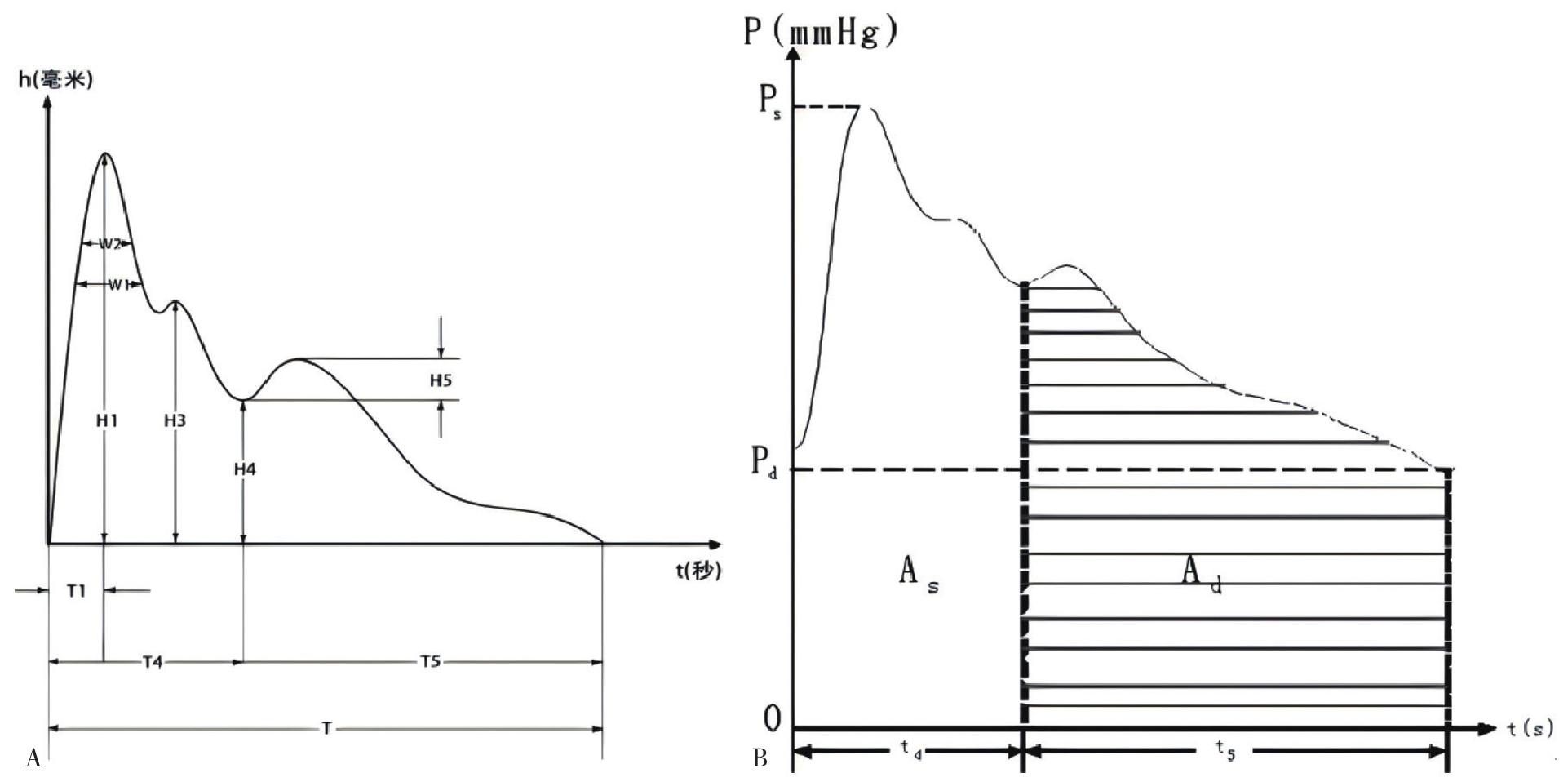
图1 脉图时域参数注:A为幅值与时值参数,B为面积参数;1 mmHg=0.133 kPa。
Figure 1 Time-domain parameters of pulse graph
| 组别 | 例数 | 性别[例(%)] | 年龄[M(P25,P75),岁] | BMI[M(P25,P75),kg/m2] | TC[M(P25,P75),mmol/L] | TG[M(P25,P75),mmol/L] | HDL-C[M(P25,P75),mmol/L] | LDL-C[M(P25,P75),mmol/L] | UA[M(P25,P75),μmol/L] | |
|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | |||||||||
| EH-NLVH组 | 119 | 71(59.7) | 48(40.3) | 67(62,72) | 26.2(23.4,28.5) | 4.23(3.56,4.98) | 1.40(1.10,1.98) | 1.02(0.91,1.22) | 2.54(1.89,3.13) | 307.50(257.70,369.45) |
| EH-LVH组 | 82 | 14(17.1) | 68(82.9) | 71(66,76) | 24.4(22.1,26.9) | 4.49(3.87,5.44) | 1.37(1.07,1.88) | 1.19(0.93,1.44) | 2.78(1.96,3.58) | 361.50(302.00,439.95) |
| Z(χ2)值 | 36.084a | -2.944 | -2.942 | -1.739 | -0.044 | -2.539 | -1.785 | -3.333 | ||
| P值 | <0.001 | 0.003 | 0.003 | 0.077 | 0.979 | 0.011 | 0.071 | 0.001 | ||
| 组别 | BUN[M(P25,P75),mmol/L] | Cys-C[M(P25,P75),mg/L] | FBG[M(P25,P75),mmol/L] | Hcy[M(P25,P75),μmol/L] | MALB[M(P25,P75),g/L] | 最高SBP[M(P25,P75),mmHg] | 最高DBP[M(P25,P75),mmHg] | 目前SBP[M(P25,P75),mmHg] | 目前DBP[M(P25,P75),mmHg] | Scr[M(P25,P75),μmol/L] |
| EH-NLVH组 | 5.60(4.54,6.88) | 1.05(0.92,1.30) | 5.90(5.20,7.53) | 13.80(11.80,18.70) | 1.21(0.74,10.10) | 170(160,180) | 100(90,100) | 135(125,149) | 80(75.0,90) | 73.30(64.10,86.10) |
| EH-LVH组 | 5.60(4.60,6.50) | 1.02(0.90,1.28) | 5.70(5.10,7.00) | 11.40(9.17,13.80) | 0.65(0.48,0.81) | 178(160,191) | 99(90,102) | 132(122,146) | 80(75,84) | 57.60(51.90,69.10) |
| Z(χ2)值 | -0.341 | -0.151 | -0.265 | -3.531 | -1.370 | -1.024 | -0.379 | -0.753 | -1.155 | -5.300 |
| P值 | 0.706 | 0.880 | 0.789 | 0.001 | 0.171 | 0.275 | 0.634 | 0.451 | 0.248 | <0.001 |
表1 EH-LVH组与EH-NLVH组一般资料比较
Table 1 Comparison of general data between EH-LVH group and EH-NLVH group
| 组别 | 例数 | 性别[例(%)] | 年龄[M(P25,P75),岁] | BMI[M(P25,P75),kg/m2] | TC[M(P25,P75),mmol/L] | TG[M(P25,P75),mmol/L] | HDL-C[M(P25,P75),mmol/L] | LDL-C[M(P25,P75),mmol/L] | UA[M(P25,P75),μmol/L] | |
|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | |||||||||
| EH-NLVH组 | 119 | 71(59.7) | 48(40.3) | 67(62,72) | 26.2(23.4,28.5) | 4.23(3.56,4.98) | 1.40(1.10,1.98) | 1.02(0.91,1.22) | 2.54(1.89,3.13) | 307.50(257.70,369.45) |
| EH-LVH组 | 82 | 14(17.1) | 68(82.9) | 71(66,76) | 24.4(22.1,26.9) | 4.49(3.87,5.44) | 1.37(1.07,1.88) | 1.19(0.93,1.44) | 2.78(1.96,3.58) | 361.50(302.00,439.95) |
| Z(χ2)值 | 36.084a | -2.944 | -2.942 | -1.739 | -0.044 | -2.539 | -1.785 | -3.333 | ||
| P值 | <0.001 | 0.003 | 0.003 | 0.077 | 0.979 | 0.011 | 0.071 | 0.001 | ||
| 组别 | BUN[M(P25,P75),mmol/L] | Cys-C[M(P25,P75),mg/L] | FBG[M(P25,P75),mmol/L] | Hcy[M(P25,P75),μmol/L] | MALB[M(P25,P75),g/L] | 最高SBP[M(P25,P75),mmHg] | 最高DBP[M(P25,P75),mmHg] | 目前SBP[M(P25,P75),mmHg] | 目前DBP[M(P25,P75),mmHg] | Scr[M(P25,P75),μmol/L] |
| EH-NLVH组 | 5.60(4.54,6.88) | 1.05(0.92,1.30) | 5.90(5.20,7.53) | 13.80(11.80,18.70) | 1.21(0.74,10.10) | 170(160,180) | 100(90,100) | 135(125,149) | 80(75.0,90) | 73.30(64.10,86.10) |
| EH-LVH组 | 5.60(4.60,6.50) | 1.02(0.90,1.28) | 5.70(5.10,7.00) | 11.40(9.17,13.80) | 0.65(0.48,0.81) | 178(160,191) | 99(90,102) | 132(122,146) | 80(75,84) | 57.60(51.90,69.10) |
| Z(χ2)值 | -0.341 | -0.151 | -0.265 | -3.531 | -1.370 | -1.024 | -0.379 | -0.753 | -1.155 | -5.300 |
| P值 | 0.706 | 0.880 | 0.789 | 0.001 | 0.171 | 0.275 | 0.634 | 0.451 | 0.248 | <0.001 |
| 组别 | 例数 | 阴虚证 | 血瘀证 | 阴虚阳亢证 | 气阴两虚证 | 气滞血瘀证 | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 无 | 有 | 无 | 有 | 无 | 有 | 无 | 有 | 无 | 有 | ||
| EH-NLVH组 | 119 | 71(59.7) | 48(40.3) | 97(81.5) | 22(18.5) | 72(60.5) | 47(39.5) | 92(77.3) | 27(22.7) | 115(96.6) | 4(3.4) |
| EH-LVH组 | 82 | 34(41.5) | 48(58.5) | 56(68.3) | 26(31.7) | 33(40.2) | 49(59.8) | 48(58.5) | 34(41.5) | 68(82.9) | 14(17.1) |
| χ2值 | 6.446 | 4.667 | 7.987 | 8.095 | 11.195 | ||||||
| P值 | 0.017 | 0.031 | 0.005 | 0.004 | 0.001 | ||||||
表2 EH-LVH组和EH-NLVH组中医证候分布比较[例(%)]
Table 2 Comparison of TCM syndrome distribution in EH-LVH group and EH-NLVH group
| 组别 | 例数 | 阴虚证 | 血瘀证 | 阴虚阳亢证 | 气阴两虚证 | 气滞血瘀证 | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 无 | 有 | 无 | 有 | 无 | 有 | 无 | 有 | 无 | 有 | ||
| EH-NLVH组 | 119 | 71(59.7) | 48(40.3) | 97(81.5) | 22(18.5) | 72(60.5) | 47(39.5) | 92(77.3) | 27(22.7) | 115(96.6) | 4(3.4) |
| EH-LVH组 | 82 | 34(41.5) | 48(58.5) | 56(68.3) | 26(31.7) | 33(40.2) | 49(59.8) | 48(58.5) | 34(41.5) | 68(82.9) | 14(17.1) |
| χ2值 | 6.446 | 4.667 | 7.987 | 8.095 | 11.195 | ||||||
| P值 | 0.017 | 0.031 | 0.005 | 0.004 | 0.001 | ||||||
| 组别 | 例数 | H3/H1 | T5 | T | W1 | W2 | W1/T | W2/T |
|---|---|---|---|---|---|---|---|---|
| EH-NLVH组 | 119 | 0.79(0.61,0.85) | 0.42(0.39,0.45) | 0.82(0.75,0.91) | 0.19(0.17,0.22) | 0.15(0.11,0.17) | 0.22(0.20,0.25) | 0.18(0.14,0.20) |
| EH-LVH组 | 82 | 0.85(0.76,0.89) | 0.43(0.41,0.47) | 0.88(0.80,0.95) | 0.21(0.18,0.23) | 0.17(0.13,0.19) | 0.25(0.22,0.27) | 0.18(0.16,0.21) |
| Z值 | -3.357 | -2.690 | -3.010 | -2.144 | -2.666 | -3.312 | -2.239 | |
| P值 | 0.001 | 0.007 | 0.003 | 0.032 | 0.008 | 0.001 | 0.025 |
表3 EH-LVH组与EH-NLVH组脉图参数比较[M(P25,P75)]
Table 3 Comparison of pulse diagram parameters in EH-LVH group and EH-NLVH group
| 组别 | 例数 | H3/H1 | T5 | T | W1 | W2 | W1/T | W2/T |
|---|---|---|---|---|---|---|---|---|
| EH-NLVH组 | 119 | 0.79(0.61,0.85) | 0.42(0.39,0.45) | 0.82(0.75,0.91) | 0.19(0.17,0.22) | 0.15(0.11,0.17) | 0.22(0.20,0.25) | 0.18(0.14,0.20) |
| EH-LVH组 | 82 | 0.85(0.76,0.89) | 0.43(0.41,0.47) | 0.88(0.80,0.95) | 0.21(0.18,0.23) | 0.17(0.13,0.19) | 0.25(0.22,0.27) | 0.18(0.16,0.21) |
| Z值 | -3.357 | -2.690 | -3.010 | -2.144 | -2.666 | -3.312 | -2.239 | |
| P值 | 0.001 | 0.007 | 0.003 | 0.032 | 0.008 | 0.001 | 0.025 |
| 影响因素 | 回归系数 | 标准误 | OR值 | 95%CI | Z值 | P值 |
|---|---|---|---|---|---|---|
| 气滞血瘀证 | 1.875 | 0.599 | 6.520 | 2.017~21.079 | 3.132 | 0.002 |
| 阴虚阳亢证 | 0.840 | 0.303 | 2.315 | 1.278~4.193 | 2.770 | 0.006 |
表4 中医证候与EH患者发生LVH风险关系的多因素Logistic回归分析
Table 4 Multivariate Logistic regression analysis of the relationship between traditional Chinese medicine syndromes and the risk of LVH in EH patients
| 影响因素 | 回归系数 | 标准误 | OR值 | 95%CI | Z值 | P值 |
|---|---|---|---|---|---|---|
| 气滞血瘀证 | 1.875 | 0.599 | 6.520 | 2.017~21.079 | 3.132 | 0.002 |
| 阴虚阳亢证 | 0.840 | 0.303 | 2.315 | 1.278~4.193 | 2.770 | 0.006 |
| 影响因素 | 回归系数 | 标准误 | OR值 | 95%CI | Z值 | P值 |
|---|---|---|---|---|---|---|
| T | 0.645 | 0.204 | 1.906 | 1.278~2.842 | 3.166 | 0.002 |
| H3/H1 | 0.454 | 0.195 | 1.575 | 1.075~2.307 | 2.333 | 0.020 |
| W1/T | 0.756 | 0.208 | 2.129 | 1.416~3.201 | 3.633 | <0.001 |
表5 脉图参数与EH患者发生LVH风险关系的多因素Logistic回归分析
Table 5 Multivariate Logistic regression analysis of the relationship between pulse diagram parameters and the risk of LVH in EH patients
| 影响因素 | 回归系数 | 标准误 | OR值 | 95%CI | Z值 | P值 |
|---|---|---|---|---|---|---|
| T | 0.645 | 0.204 | 1.906 | 1.278~2.842 | 3.166 | 0.002 |
| H3/H1 | 0.454 | 0.195 | 1.575 | 1.075~2.307 | 2.333 | 0.020 |
| W1/T | 0.756 | 0.208 | 2.129 | 1.416~3.201 | 3.633 | <0.001 |
| 影响因素 | 回归系数 | 标准误 | OR值 | 95%CI | Z值 | P值 |
|---|---|---|---|---|---|---|
| LDL-C | 0.413 | 0.172 | 1.511 | 1.079~2.115 | 2.405 | 0.016 |
| 阴虚阳亢证 | 0.913 | 0.343 | 2.493 | 1.272~4.885 | 2.661 | 0.008 |
| 气滞血瘀证 | 2.063 | 0.650 | 7.866 | 2.201~28.110 | 3.174 | 0.002 |
| T | 0.646 | 0.223 | 1.907 | 1.233~2.951 | 2.900 | 0.004 |
| H3/H1 | 0.438 | 0.213 | 1.549 | 1.021~2.351 | 2.057 | 0.040 |
| W1/T | 0.756 | 0.225 | 2.129 | 1.369~3.310 | 3.354 | 0.001 |
表6 EH患者发生LVH影响因素的多因素Logistic回归分析
Table 6 Multivariate Logistic regression analysis of influencing factors for LVH in EH patients
| 影响因素 | 回归系数 | 标准误 | OR值 | 95%CI | Z值 | P值 |
|---|---|---|---|---|---|---|
| LDL-C | 0.413 | 0.172 | 1.511 | 1.079~2.115 | 2.405 | 0.016 |
| 阴虚阳亢证 | 0.913 | 0.343 | 2.493 | 1.272~4.885 | 2.661 | 0.008 |
| 气滞血瘀证 | 2.063 | 0.650 | 7.866 | 2.201~28.110 | 3.174 | 0.002 |
| T | 0.646 | 0.223 | 1.907 | 1.233~2.951 | 2.900 | 0.004 |
| H3/H1 | 0.438 | 0.213 | 1.549 | 1.021~2.351 | 2.057 | 0.040 |
| W1/T | 0.756 | 0.225 | 2.129 | 1.369~3.310 | 3.354 | 0.001 |
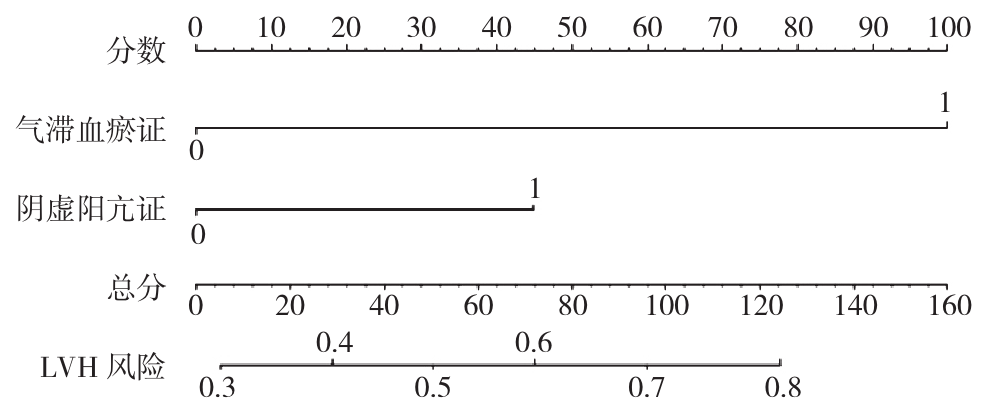
图2 基于中医证候构建的列线图注:LVH=左心室肥厚。
Figure 2 Nomogram based on TCM syndromes
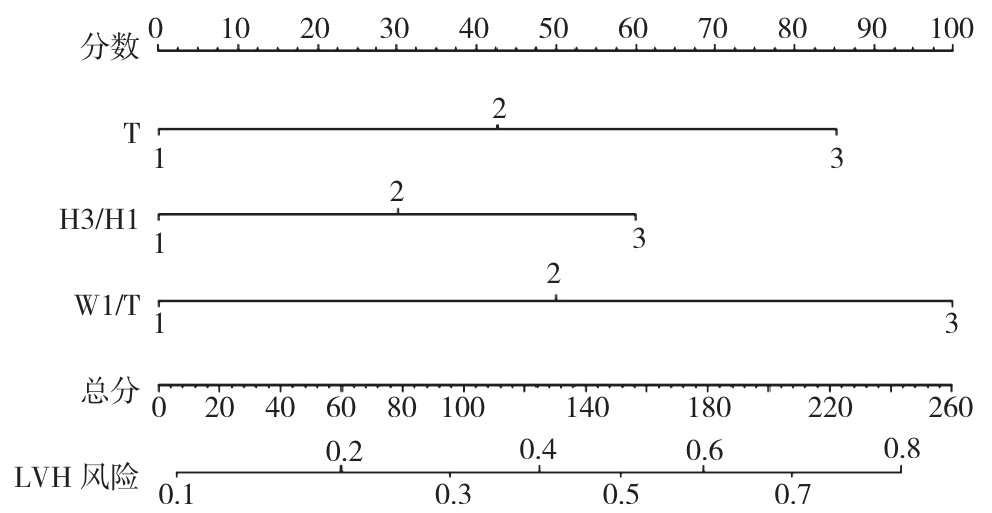
图3 基于脉图参数构建的列线图
Figure 3 Nomogram based on pulse graph parameters
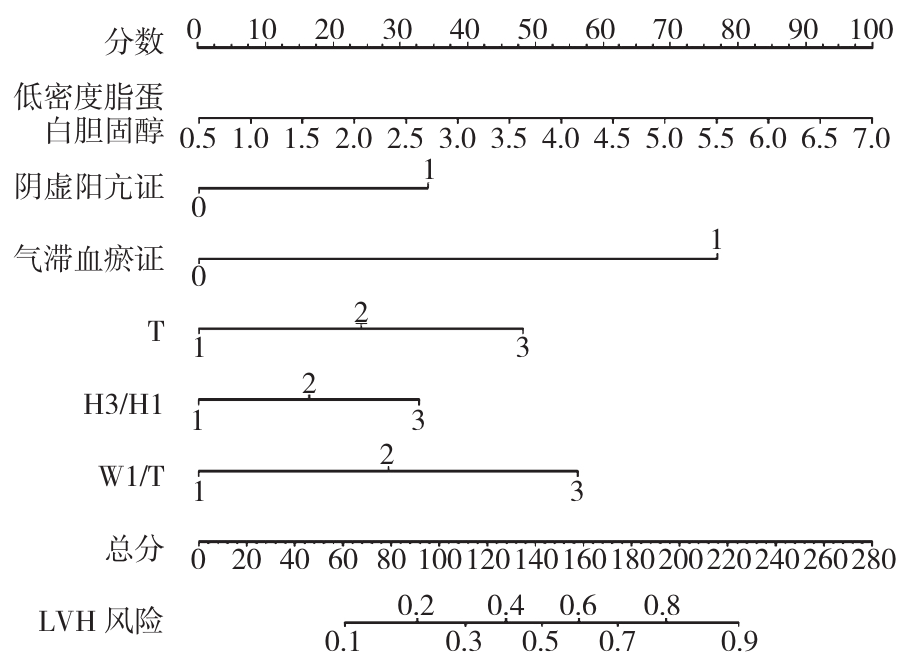
图4 基于中医证候+脉图参数+一般资料构建的列线图
Figure 4 Nomogram based on TCM syndrome+pulse graph parameters+general data
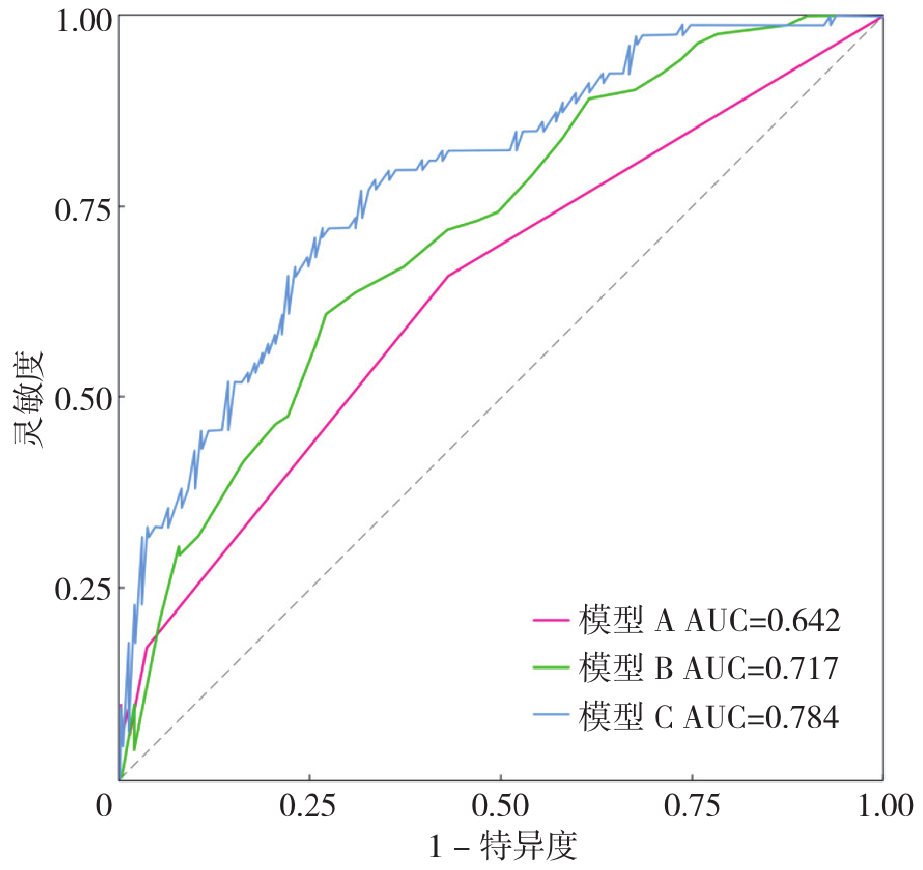
图5 3个列线图模型预测EH-LVH的ROC曲线注:AUC=受试者工作特征曲线下面积。
Figure 5 ROC curves of the three nomogram models for predicting EH-LVH
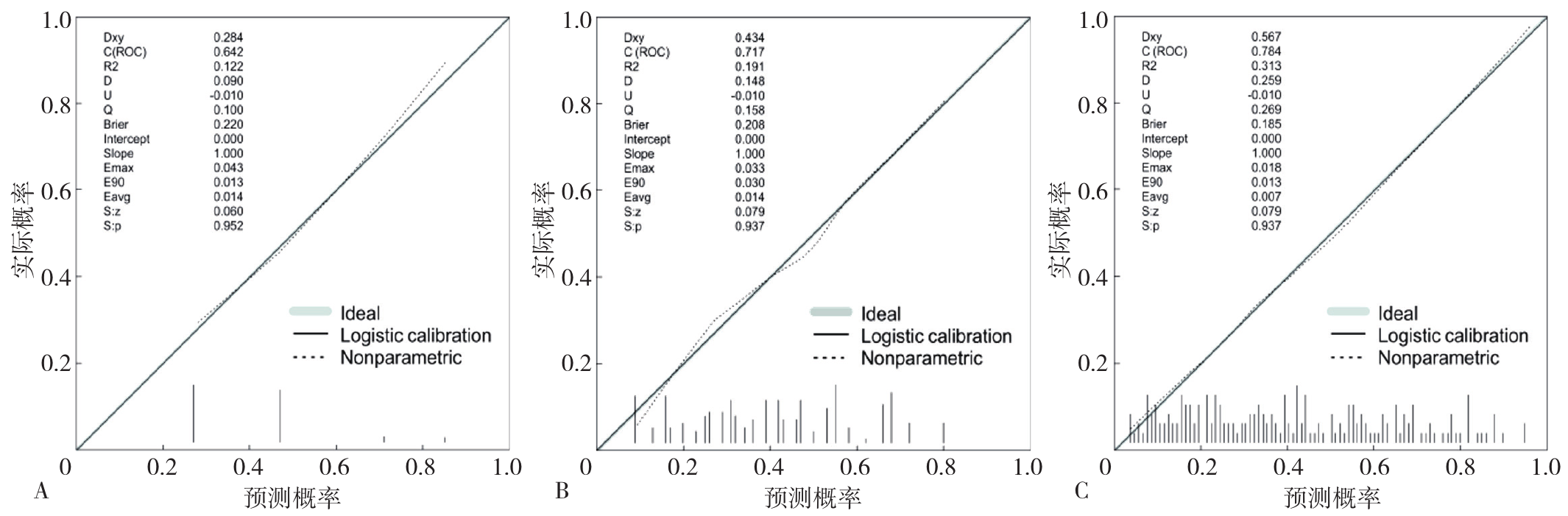
图6 3个列线图模型的校准曲线注:A为模型A,B为模型B,C为模型C。
Figure 6 Calibration curves of the three nomogram models
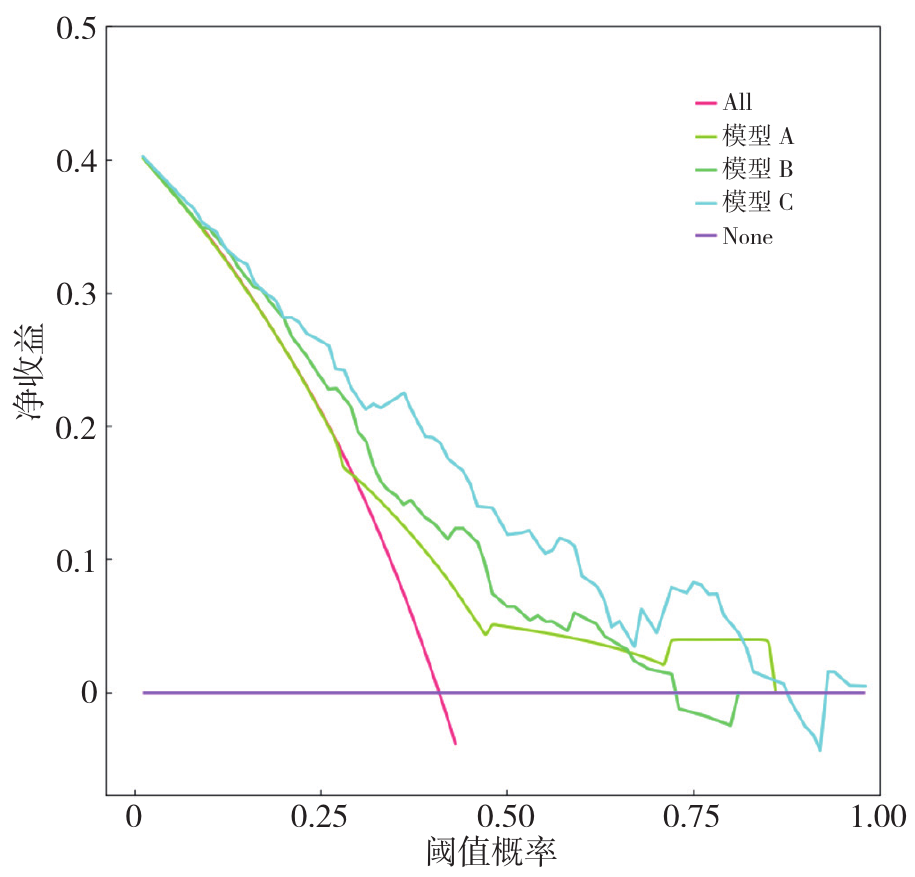
图7 3个列线图模型的DCA曲线
Figure 7 DCA curves of the three nomogram models
| [1] |
|
| [2] |
傅桑娅, 李正昕, 温清, 等.心血管疾病风险预测的危险因素和模型构建的研究进展[J].中华高血压杂志, 2024, 32(11): 1020-1028. DOI: 10.16439/j.issn.1673-7245.2024.11.006.
|
| [3] |
费兆馥.现代中医脉诊学[M].北京: 人民卫生出版社, 2006: 14-18.
|
| [4] |
牛欣. 脉诊位,数,形,势变化的心血管生理学探讨[J]. 北京中医学院学报, 1992(1): 30-33.
|
| [5] |
张梦楚, 赵倩倩, 解天骁, 等. 基于脉图参数构建原发性高血压患者伴左心室肥厚的风险预测列线图模型[J]. 中国中医药信息杂志, 2022, 29(8): 116-122. DOI: 10.19879/j.cnki.1005-5304.202112351.
|
| [6] |
|
| [7] |
中国高血压防治指南修订委员会, 高血压联盟(中国), 中国医疗保健国际交流促进会高血压分会, 等. 中国高血压防治指南(2024年修订版)[J]. 中华高血压杂志, 2024, 32(7): 603-700.
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
黄元伟, 戚文航. 临床心血管病学[M]. 天津: 天津科学技术出版社, 1998: 26-34.
|
| [12] |
胡亮亮. 基于中医四诊信息的冠心病发病风险预测模型研究[D]. 上海: 上海中医药大学, 2019.
|
| [13] |
朱文锋. 证素辨证学[M].北京: 人民卫生出版社, 2008: 36-53.
|
| [14] |
国家技术监督局. 中医临床诊疗术语 证候部分: GB/T 16751.2—1997[S]. 北京: 中国标准出版社, 2004.
|
| [15] |
张伯臾. 中医内科学[M]. 上海: 上海科学技术出版社, 1985.
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
王永炎, 严世芸. 实用中医内科学[M]. 2版. 上海: 上海科学技术出版社, 2009: 108.
|
| [23] |
|
| [24] |
|
| [25] |
程斌, 宋婷婷, 董昌武. 近5年中医药防治高血压左心室肥厚研究[J]. 中医药临床杂志, 2018, 30(6): 995-998.
|
| [26] |
方媛, 倪永骋. 基于心脏稳态失衡探析高血压心脏病从虚和瘀论治内涵[J]. 中国中医药信息杂志, 2024, 31(12): 15-19.
|
| [27] |
成思燃. 老年高血压患者血脂异常与左室收缩功能及左室质量指数的相关性研究[D]. 银川: 宁夏医科大学, 2020.
|
| [28] |
岳军. 血清HDL-C、LDL-C对老年2型糖尿病患者动脉粥样硬化的评估分析[J]. 心血管病防治知识, 2021, 11(30): 3-5.
|
| [29] |
杨继, 张垚, 张秋月, 等. 高血压病并发脑卒中的影响因素分析及风险预测模型的初步建立——3859例回顾性研究[J]. 中医杂志, 2021, 62(10): 868-873.
|
| [30] |
|
| [31] |
郑筱萸. 中药新药临床研究指导原则——试行[M]. 北京: 中国医药科技出版社, 2002: 73-77.
|
| [32] |
靳利利, 王清海, 李典鸿. 高血压左心室肥厚患者的中医辨证分型研究[J]. 辽宁中医杂志, 2008, 35(10): 1542. DOI: 10.3969/j.issn.1000-1719.2008.10.053.
|
| [33] |
叶天士. 临证指南医案[M]. 苏礼, 整理. 北京: 人民卫生出版社, 2018: 10.
|
| [34] |
关山月. 高血压左心室肥厚中医证型与左心室结构指标的关系及中药干预研究[D]. 北京: 北京中医药大学, 2015.
|
| [35] |
邢长城. 原发性高血压的中医辨证分型与左心室肥厚的相关性研究[D]. 济南: 山东中医药大学, 2021.
|
| [36] |
田代华. 黄帝内经素问[M]. 北京: 人民卫生出版社, 2017.
|
| [37] |
范金茹, 王行宽, 熊国强. 高血压左室肥厚中医病名、病位、病因病机探讨[J]. 中医药通报, 2005, 4(2): 19-21.
|
| [38] |
刘璐, 马泽慧, 陈聪, 等. 上海中医药大学在校大学生不同情感状态脉图特征参数分析与识别[J]. 中国中医药信息杂志, 2019, 26(4): 19-23.
|
| [39] |
陈新胜, 柯植泉. 原发性高血压合并左心室肥厚与心率变异性及室性心律失常的相关性研究[J]. 临床医学工程, 2016, 23(7): 863-864.
|
| [40] |
刘璐, 陈瑞, 张春柯, 等. 冠状动脉不同病变程度患者中医脉图特征参数分析[J]. 中国中医药信息杂志, 2020, 27(4): 13-17.
|
| [41] |
姚天文, 王清亮, 潘诗蕾, 等. 健康成人不同年龄、不同性格对中医脉图的影响[J]. 中华中医药学刊, 2015, 33(11): 2775-2777.
|
| [42] |
陈一峰, 方寒蕊, 王浩, 等. 高血压200例脉象及病机分析[J]. 中国社区医师, 2021, 37(27): 91-92.
|
| [43] |
王蕾, 尚倩倩, 钱鹏, 等. 高血压病患者动态动脉硬化指数的研究现状及对中医脉诊研究的启示[J]. 中华中医药杂志, 2017, 32(11): 4793-4797.
|
| [44] |
武玉琳, 齐新, 魏丽萍, 等. 老年高血压患者的无创血流动力学参数与心脏结构变化的关系[J]. 中华老年心脑血管病杂志, 2020, 22(1): 10-14.
|
| [1] | 胡嘉琦, 李端, 方昊, 樊兴颖, 杜薇, 周涵妮. 基于体检人群队列的高尿酸血症非遗传因素风险预测模型构建研究[J]. 中国全科医学, 2026, 29(10): 1324-1333. |
| [2] | 余新艳, 马忠, 曹凡, 苏鹏, 林颖, 张海澄. 基于单导联可穿戴心电设备预测基层老年心血管代谢疾病患者抑郁发生风险的研究[J]. 中国全科医学, 2026, 29(10): 1300-1310. |
| [3] | 曹磊, 刘学春, 江伟, 陈炎, 严孙宏, 杜静. 颞肌横截面积和颞肌厚度预测急性缺血性脑卒中患者肌肉衰减状态的研究[J]. 中国全科医学, 2026, 29(08): 997-1007. |
| [4] | 李丽清, 刘文慧, 杨嘉逸, 王芳. 我国中部六省优质医疗资源与经济社会耦合协调发展的时空演化与趋势预测[J]. 中国全科医学, 2026, 29(07): 844-850. |
| [5] | 李纪新, 邱林杰, 任燕, 王文茹, 李美洁, 栗文婕, 邹姹姹, 吴梓敬, 张晋. 肌肉与脂肪比值对非超重/肥胖2型糖尿病的预测价值研究[J]. 中国全科医学, 2026, 29(06): 726-732. |
| [6] | 刘璠, 李嘉丽, 柯立鑫, 张强, 陈嘉慧, 卢存存, 赵信科. 1990—2021年全球与中国60岁及以上人群高胆固醇血症的疾病负担:趋势分析与模型预测[J]. 中国全科医学, 2026, 29(05): 631-640. |
| [7] | 江晓蕊, 闫玉瑶, 卫靖靖, 乔利杰, 彭广操, 朱明军. 冠心病患者并发心力衰竭风险预测模型的系统评价[J]. 中国全科医学, 2026, 29(03): 393-402. |
| [8] | 代天顾, 何清, 高雪菲, 张高钰, 樊佳溶, 王子涵, 肖响, 李琳. 肱踝脉搏波传导速度和血清总胆固醇及N末端B型脑钠肽前体联合检测对原发性高血压患者发生冠心病的预测价值研究[J]. 中国全科医学, 2025, 28(32): 4061-4066. |
| [9] | 秦邦国, 孙瑾, 李曼, 邱娇娇, 程柏凯, 朱平, 王曙霞. 农村高血压人群非高密度脂蛋白胆固醇与高密度脂蛋白胆固醇比值与左心室肥厚的关系研究[J]. 中国全科医学, 2025, 28(30): 3753-3760. |
| [10] | 贾高鹏, 陈秋雨. 老年急性ST段抬高型心肌梗死经皮冠状动脉介入治疗术后心绞痛复发风险预测模型构建和验证:基于CYP2C19相关基因检测[J]. 中国全科医学, 2025, 28(30): 3779-3786. |
| [11] | 徐百川, 王艳, 张彭, 李艺婷, 刘飞来, 谢洋. 慢性阻塞性肺疾病共病肺癌筛查工具分析[J]. 中国全科医学, 2025, 28(30): 3847-3852. |
| [12] | 李玲, 李雅萍, 钱时兴, 聂婧, 陆春华, 李霞. 社区中老年人认知功能影响因素及风险预测研究[J]. 中国全科医学, 2025, 28(30): 3773-3778. |
| [13] | 刘银银, 隋鸿平, 李婷婷, 姜桐桐, 史铁英, 夏云龙. 乳腺癌治疗相关心脏毒性风险预测模型的研究进展[J]. 中国全科医学, 2025, 28(24): 3072-3078. |
| [14] | 吴莎, 张代义, 李晋, 宣勤考, 钱晓东, 朱传武, 浦剑虹, 朱莉. 基于体检队列的代谢相关脂肪性肝病与高血糖关联及联合预测模型构建研究[J]. 中国全科医学, 2025, 28(23): 2861-2869. |
| [15] | 周倩, 吴晓敏, 王宝华, 严若菡, 蔚苗, 吴静. 胃癌发生风险的列线图预测模型研究[J]. 中国全科医学, 2025, 28(23): 2870-2877. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










