中国全科医学 ›› 2023, Vol. 26 ›› Issue (13): 1641-1647.DOI: 10.12114/j.issn.1007-9572.2022.0421
所属专题: 社区卫生服务最新研究合辑; 家庭医生团队最新文章合集
徐佳玙1, 颜骅1,*( ), 方军波1, 王海琴1, 郭佩1, 沈福来2, 王形松2
), 方军波1, 王海琴1, 郭佩1, 沈福来2, 王形松2
XU Jiayu1, YAN Hua1,*(), FANG Junbo1, WANG Haiqin1, GUO Pei1, SHEN Fulai2, WANG Xingsong2
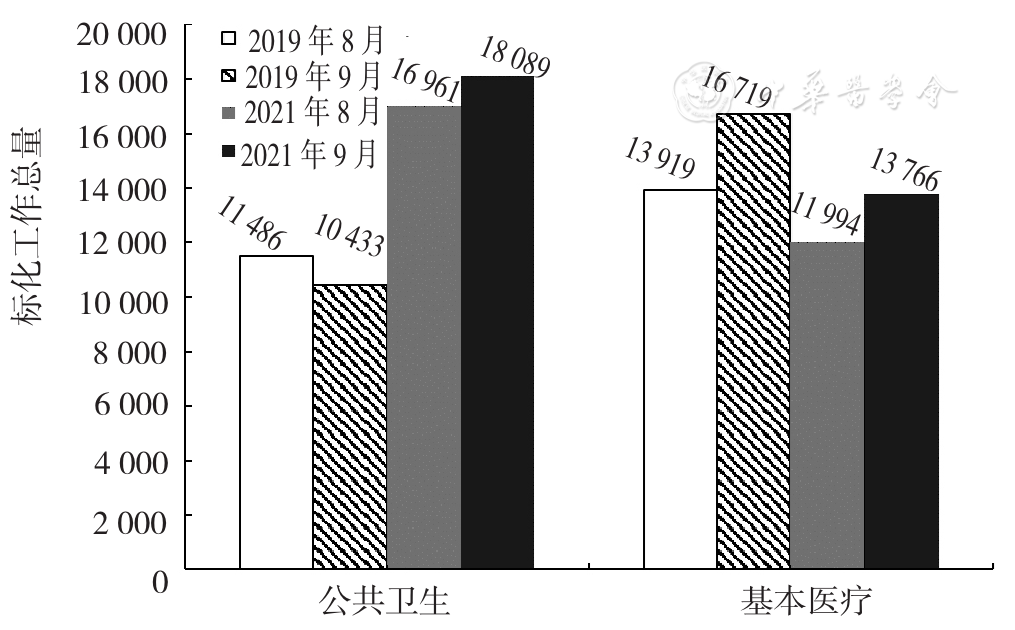
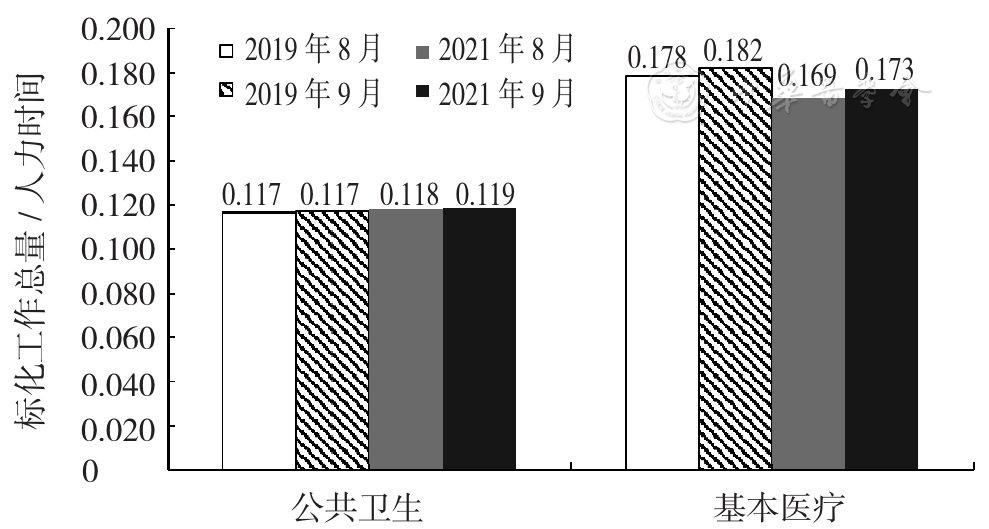
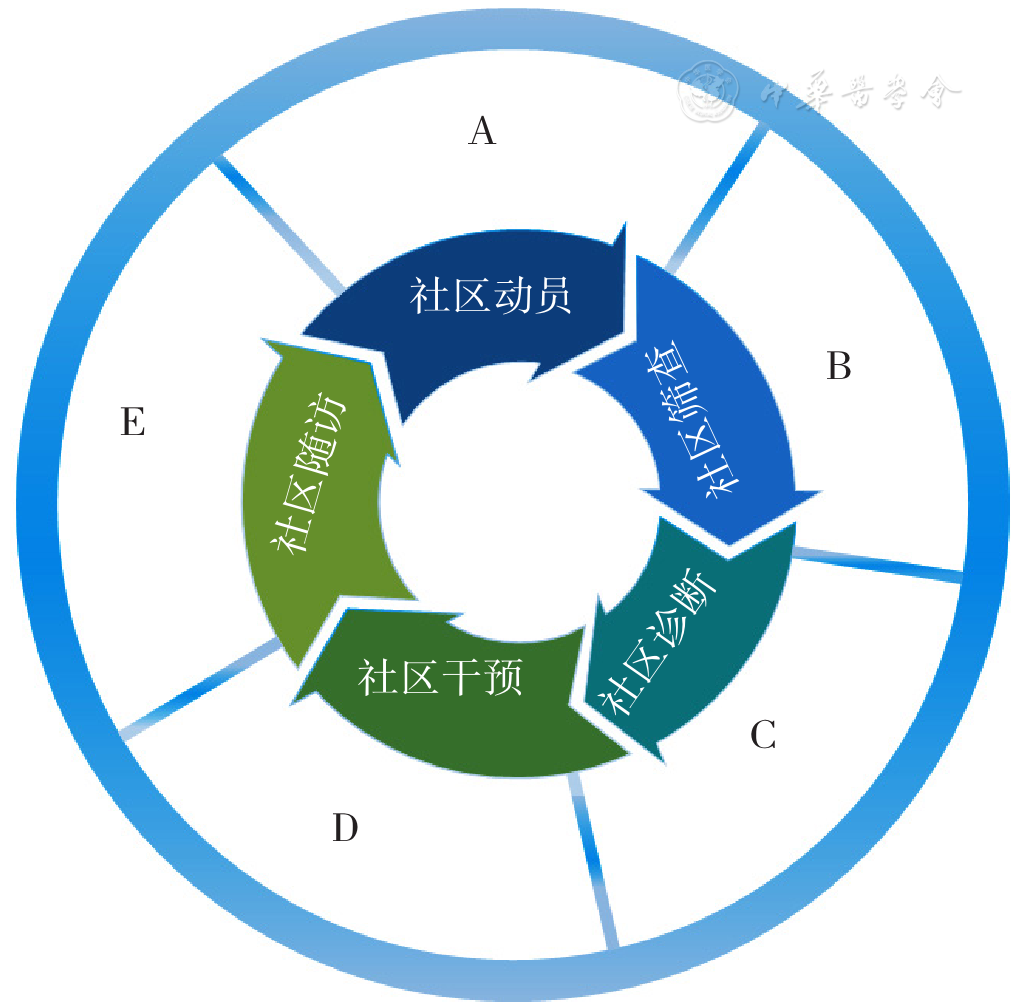
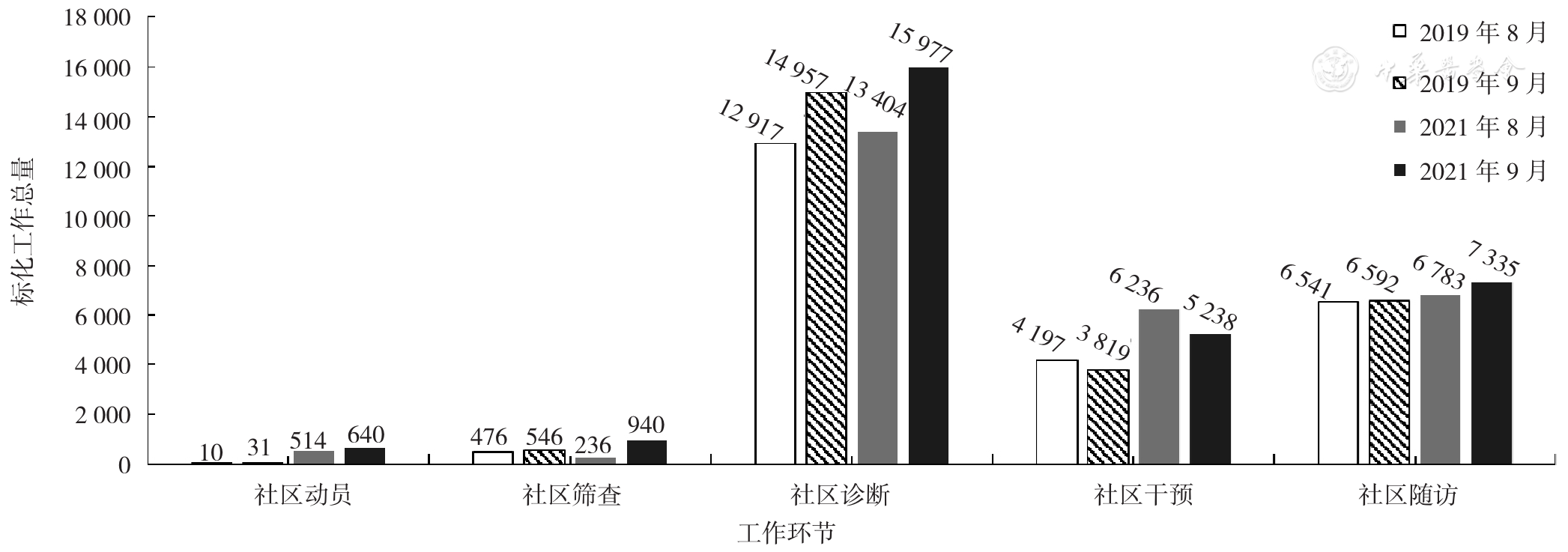
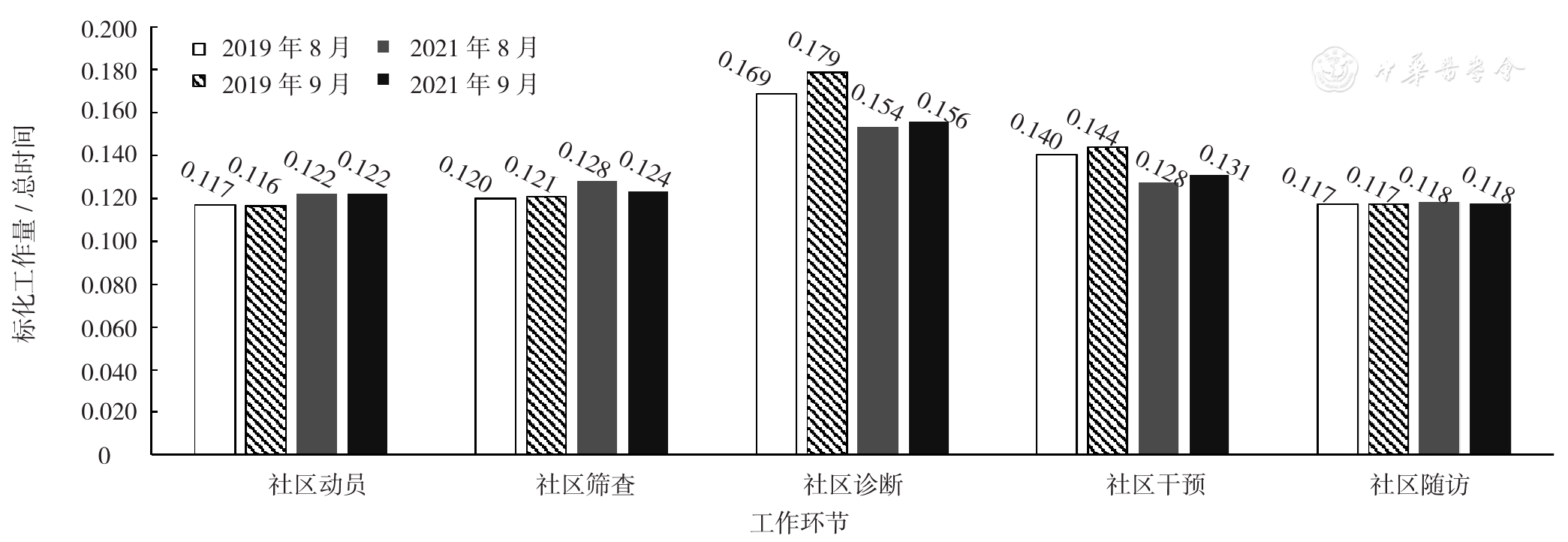
摘要: 背景 家庭医生团队在运行过程中存在着工作内容条理不清、分工不合理和"高能低用"等问题,制约了家庭医生团队的整体发展。 目的 基于标化工作量对上海市中心城区社区卫生服务机构家庭医生团队工作开展现状进行分析,了解阻碍家庭医生团队发展的主要因素,为家庭医生团队工作模式改进提供指导。 方法 于2021年7—11月,以上海市徐汇区斜土街道社区卫生服务中心的家庭医生团队为研究对象,收集该机构家庭医生团队于2019年8—9月和2021年8—9月所开展的服务项目、各项目标化工作量相关参数、各项目发生数量。一是根据服务项目的性质,将家庭医生团队服务分为基本医疗服务和公共卫生服务,计算其基本医疗和公共卫生工作的标化工作总量和总时间;二是根据医防融合的思路,将家庭医生团队工作拆分为社区动员、社区筛查、社区诊断、社区干预、社区随访5个环节,计算各工作环节的标化工作总量和总时间;三是运用优劣解距离法(TOPSIS)对家庭医生社区动员、社区筛查、社区随访环节的所有服务项目的价值水平进行综合评价。 结果 2021年8月和9月家庭医生团队公共卫生服务的标化工作总量分别为16 961和18 089,2019年的同期数据分别为11 486和10 433,平均涨幅为59.9%。Pearson相关分析结果显示,家庭医生团队的基本医疗服务标化工作总量与公共卫生服务标化工作总量无相关关系(r=-0.72,P=0.27)。家庭医生团队在各环节的标化工作总量从大到小依次为:社区诊断、社区随访、社区干预、社区筛查、社区动员。社区动员、社区筛查、社区随访环节的标化工作量/总时间相对较低。根据TOPSIS评价结果,更新慢性病患者健康档案、高血压和糖尿病患者随访管理、签约居民信息维护等13个项目可考虑外包或降低执行人力成本。 结论 家庭医生团队尚未形成有效的工作方式来实现医防融合,导致公共卫生服务中非必须家庭医生执行环节浪费过多人力资源,并进而影响了家庭医生的基本医疗工作开展。下一步,应加强家庭医生团队社区干预相关专业技能的培训,增加相关设施设备;优化家庭医生团队各工作环节的人力资源配置,主要降低社区动员、社区筛查和社区随访的执行人力成本。