Background The prevalence of heart failure (HF) is growing in a rapidly increased number of older adults (≥60 years) , which, together with older age, produces an impact on nutritional status of the HF cases. But there are relatively few studies on the impact of nutritional status on the prognosis in elderly patients with chronic HF.
Methods A retrospective cohort study was conducted. Inpatients with HFpEF and coronary heart disease (≥60 years old, NYHA gradeⅡ-Ⅳ) treated in Department of Geriatrics, Beijing Tongren Hospital, Capital Medical University between 2017 and 2019 were enrolled. Clinical and laboratory data were collected. HF-related readmission and all-cause mortality within one year after discharge were followed up. Nutritional status was evaluated by controlling nutritional status (CONUT) score, geriatric nutritional risk index (GNRI) and prognostic nutritional index (PNI) . Patients were divided into non-malnutrition group (CONUT score 0-1, n=42) , low malnutrition risk group (CONUT score 2-4, n=181) and medium-high malnutrition risk group (CONUT score 5-12, n=156) . The differences in clinical data and prognosis among the three groups were compared. Univariate and multivariate logistic regression analyses were used to explore the influencing factors of readmission due to HF and all-cause mortality within one year after discharge. ROC analysis was used to analyze the prognostic value of CONUT score, GNRI and PNI for readmission due to HF and all-cause mortality within 1 year after discharge.
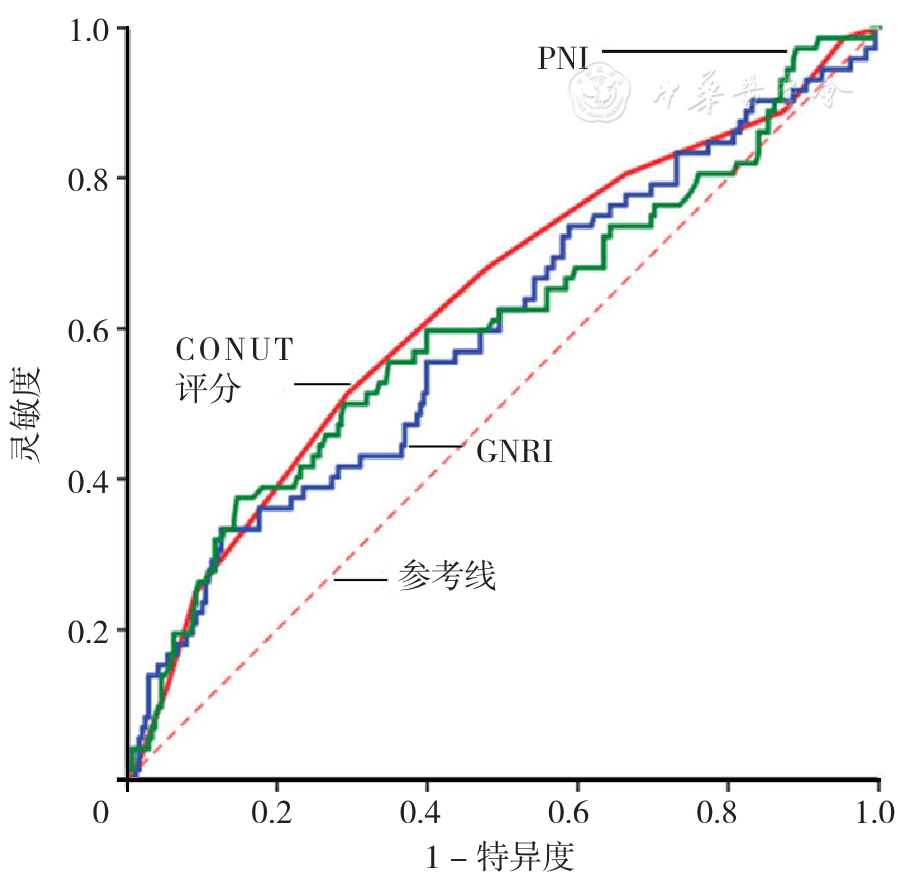
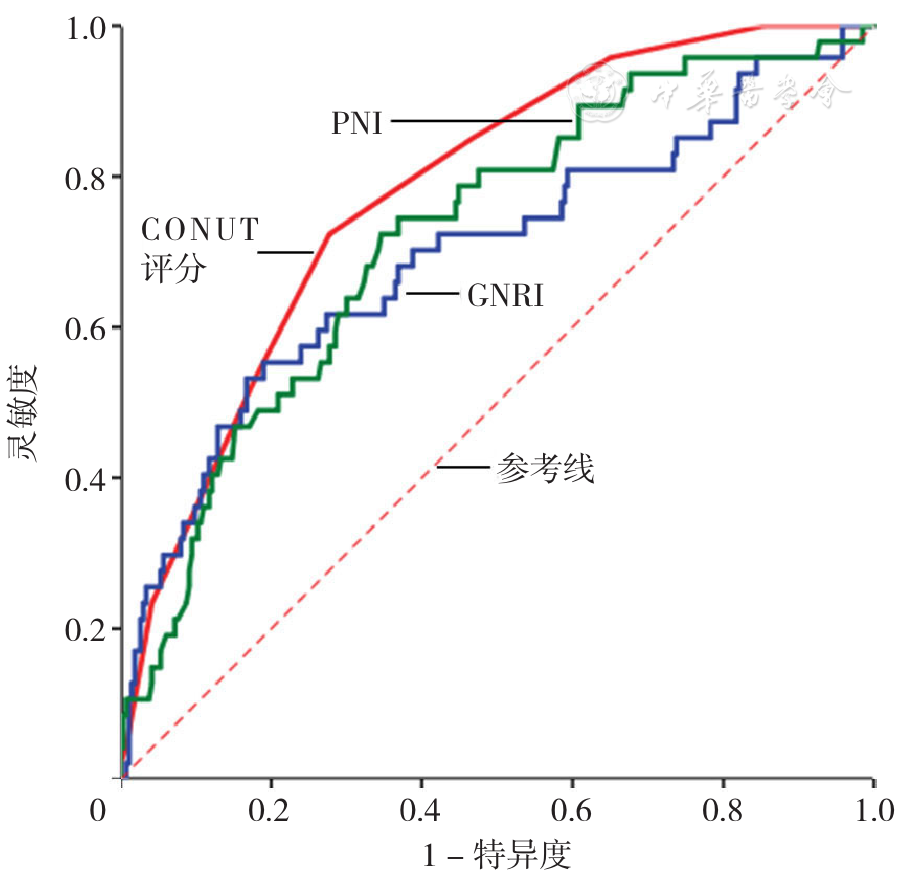
Results Age, proportion of elderly patients, sex, BMI, bed rest, length of hospital stay, NYHA grade, hemoglobin, lymphocytes, urea nitrogen, creatinine, total protein, albumin, triacylglycerol, total cholesterol, low density lipoprotein cholesterol, B-type brain natriuretic peptide (BNP) , all-cause death within 1 year were compared among the three groups, and there were statistically significant differences (P<0.05) ; among them, age, proportion of elderly patients, bed rest, length of hospital stay, NYHA grade, old myocardial infarction, urea nitrogen, creatinine, BNP, and all-cause death within 1 year in the no-malnutrition risk group and the low-malnutrition risk group were significantly lower than those in the medium-high malnutrition risk group (P<0.05) , and BMI, hemoglobin, lymphocytes, total protein, albumin, triacylglycerol, total cholesterol and low-density lipoprotein cholesterol were significantly higher than those in the medium-high malnutrition risk group (P<0.05) . Univariate logistic regression analysis showed that age, bed rest, length of stay, NYHA grade, hemoglobin, albumin, BNP, left ventricular ejection fraction, CONUT score, GNRI and PNI are the influencing factors of readmission due to HF and all-cause death within 1 year (P<0.05) . Multivariate logistic regression analysis showed that CONUT score〔OR=1.567, 95%CI (1.302, 1.885) , P<0.05〕 is an influence factor of all-cause death within 1 year (P<0.05) . ROC analysis estimating the performance in predicting all-cause mortality within one year after discharge showed that the AUC of CONUT score was 0.780〔95%CI (0.714, 0.845) 〕 with 0.723 sensitivity and 0.722 specificity when the optimal cut-off value was determined as 7.5, the AUC of GNRI was 0.695〔95%CI (0.604, 0.786) 〕with 0.532 sensitivity and 0.833 specificity when the optimal cut-off value was determined as 89, and the AUC of PNI was 0.722〔95%CI (0.643, 0.800) 〕 with 0.723 sensitivity and 0.654 specificity when the optimal cut-off value was determined as 41.

 ), 郑辉, 何玉
), 郑辉, 何玉