中国全科医学 ›› 2022, Vol. 25 ›› Issue (24): 3043-3048.DOI: 10.12114/j.issn.1007-9572.2022.0087
张鹏, 黄艳平*( ), 林铭佳, 经文娟, 蒋忠胜
), 林铭佳, 经文娟, 蒋忠胜
Peng ZHANG, Yanping HUANG*(), Mingjia LIN, Wenjuan JING, Zhongsheng JIANG
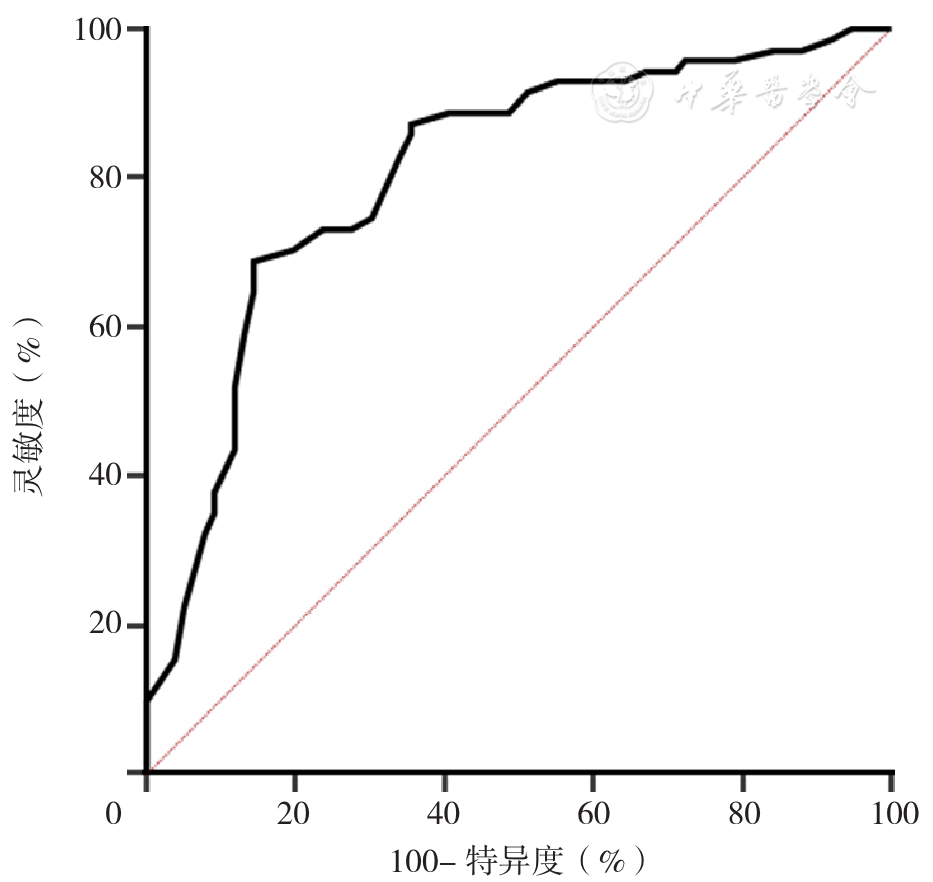
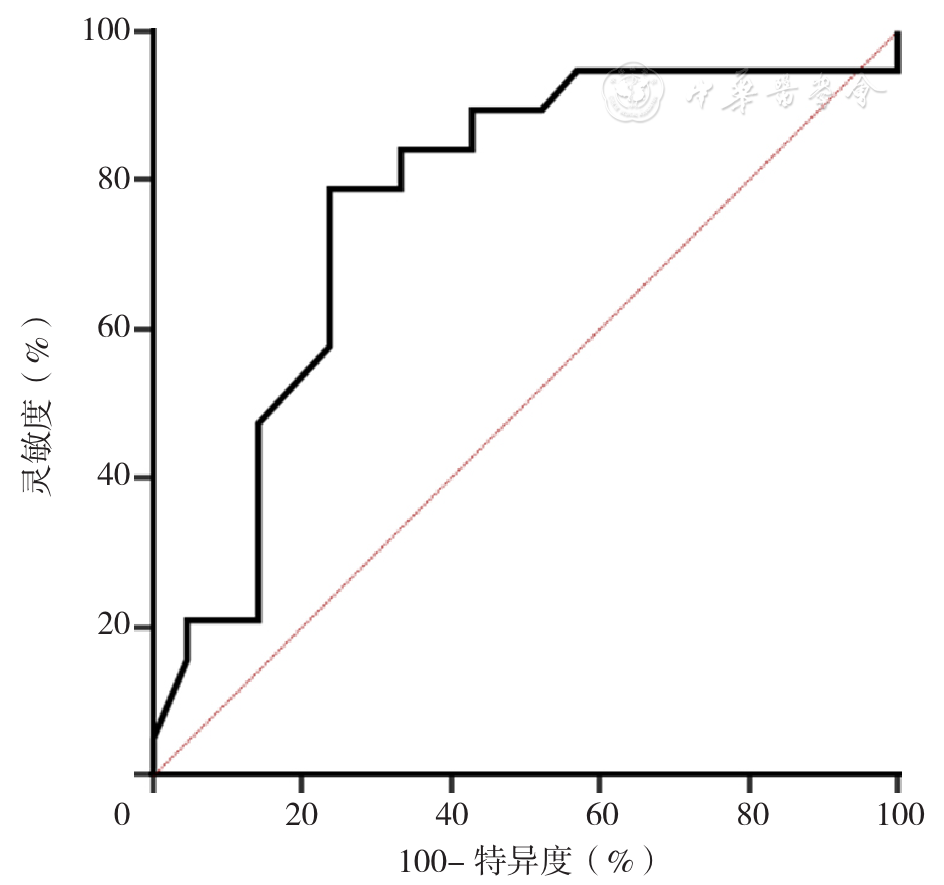
摘要: 背景 结核性脑膜炎(TM)是临床常见的中枢性感染的一种,其起病较慢,症状不典型,病原学诊断困难,误诊率高。目前有效的TM诊断工具较少。利用常见的临床症状、检查指标等建立诊断评分系体可提高诊断准确率,减少误诊。 目的 建立TM临床诊断评分体系(TMCDS),并对其应用价值进行初步评价。 方法 选取2011年11月至2021年9月在柳州市人民医院感染病科住院并诊断为脑膜炎的患者187例为研究对象,采用SPSS 21.0统计软件将患者随机分成建模组(147例)和验模组(40例)。根据是否为TM将建模组分为非TM亚组(76例)和TM亚组(71例)。收集患者的一般资料,主要包括性别、年龄、临床症状(发热、头痛、意识障碍、颈抵抗),实验室及影像学检查结果,包括人类免疫缺陷病毒(HIV)感染情况、CD4+ T淋巴细胞计数、C反应蛋白、颅内压、脑脊液常规生化检查(糖、氯、蛋白、细胞数)。建模组采用多因素Logistic回归分析探讨TM的影响因素;根据每个因素的β值所占比重设立相应分值,建立TMCDS;采用受试者工作特征曲线(ROC曲线)分析TMCDS诊断TM的价值。 结果 两亚组头痛、HIV感染、CD4+ T淋巴细胞计数<200/μl、C反应蛋白升高、颅内压>200 mm H2O(1 mm H2O=0.009 8 kPa)、脑脊液糖降低、脑脊液氯降低、脑脊液蛋白升高、脑脊液单核细胞升高情况比较,差异有统计学意义(P<0.05)。多因素Logistic回归分析结果显示,头痛、CD4+ T淋巴细胞<200/μl、C反应蛋白升高、脑脊液糖降低、脑脊液蛋白升高均是TM的影响因素(P<0.05)。将以上5个影响因素同时结合临床经验纳入脑脊液氯、脑脊液细胞数再次进行多因素Logistic回归分析,结果显示,头痛、CD4+ T淋巴细胞<200/μl、C反应蛋白升高、脑脊液糖降低、脑脊液蛋白升高均是TM的影响因素(P<0.05)。根据上述7个因素β值建立评分系统,将脑脊液氯降低β值设定为1分,其他因素β值与其的倍数即为该因素所对应的分值,因2个影响因素评分为负值,为方便临床,每个因素对应分值增加2.5分,最终建立TMCDS。TMCDS诊断建模组TM的ROC曲线下面积(AUC)为0.807〔95%CI(0.735,0.879),标准误=0.037,P<0.001〕,最佳诊断界值为21.50分。TMCDS诊断验模组TM的AUC为0.766〔95%CI(0.610,0.921),标准误=0.079,P=0.004〕,灵敏度为0.789,特异度为0.667。 结论 通过7个变量建立的TMCDS简单易行,对于早期TM具有较高的临床诊断价值。