中国全科医学 ›› 2023, Vol. 26 ›› Issue (18): 2227-2231.DOI: 10.12114/j.issn.1007-9572.2022.0873
所属专题: 内分泌代谢性疾病最新文章合集; 泌尿系统疾病最新文章合集; 老年问题最新文章合集
赵丽珍*( ), 李卫民, 姜瑞霞
), 李卫民, 姜瑞霞
ZHAO Lizhen*(), LI Weimin, JIANG Ruixia
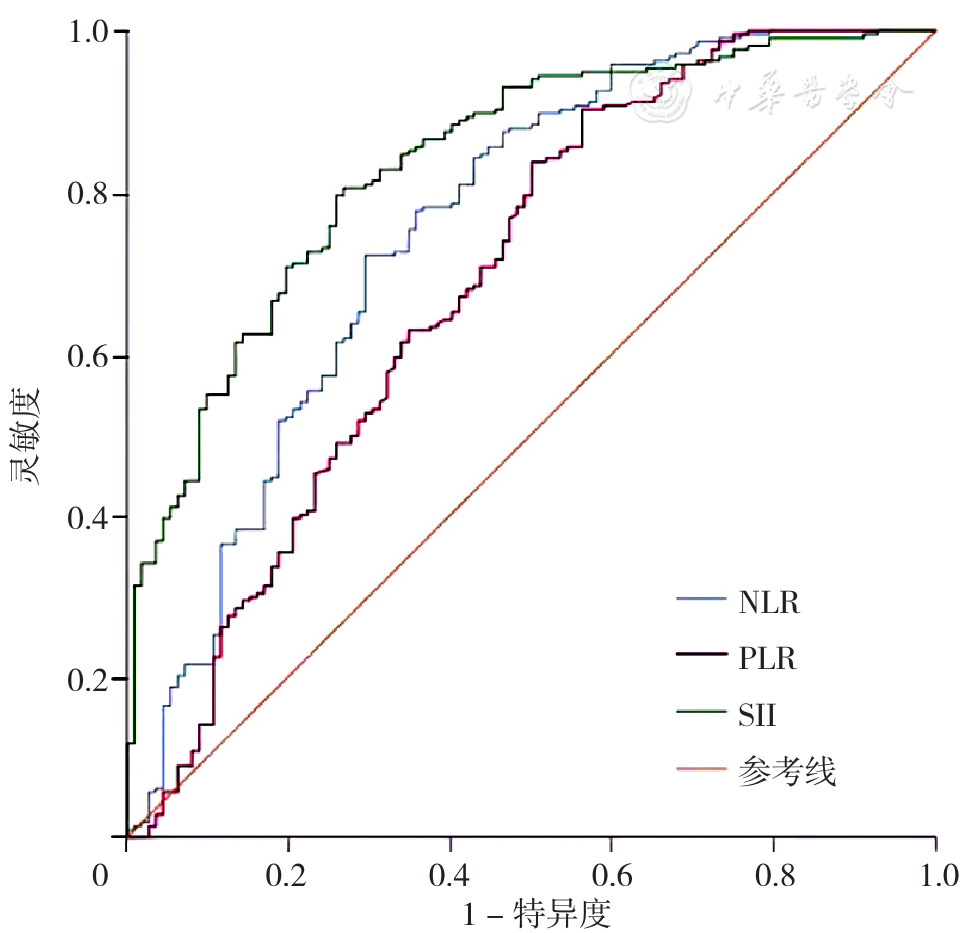
摘要: 背景 糖尿病肾病(DKD)是糖尿病常见并发症,以损伤肾脏微血管为主要特征,其早期诊断、积极防治是改善预后的关键。血液炎性指标可能与DKD存在相关性。 目的 探究系统免疫炎症指数(SII)对社区老年2型糖尿病(T2DM)患者并发DKD的诊断价值。 方法 回顾性分析2021年1—12月于首都医科大学附属北京朝阳医院西区社区医疗部常规体检的老年T2DM患者327例为研究对象。根据是否并发DKD将327例T2DM患者分为非DKD组(n=112)和DKD组(n=215)。收集两组患者的一般资料及实验室检查资料并进行比较。采用Pearson相关分析及Spearman秩相关分析探讨老年T2DM患者尿白蛋白/肌酐比值(UACR)与各指标的相关性;采用多因素Logistic回归分析探讨老年T2DM患者并发DKD的影响因素;采用受试者工作特征曲线(ROC曲线)评估中性粒细胞/淋巴细胞比值(NLR)、血小板/淋巴细胞比值(PLR)、SII对社区老年T2DM患者并发DKD的诊断价值,并计算ROC曲线下面积(AUC)及其95%CI。 结果 DKD组患者的T2DM病程长于非DKD组,高血压病史比例、空腹葡萄糖(FPG)、低密度脂蛋白(LDL)、尿素氮(BUN)、血肌酐(Scr)、UACR、中性粒细胞计数、血小板计数、NLR、PLR、SII水平高于非DKD组(P<0.05)。相关性分析结果显示,老年T2DM患者UACR与T2DM病程、FPG、三酰甘油(TG)、LDL、中性粒细胞、血小板、NLR、PLR、SII呈正相关(r=0.716、0.114、0.113、0.144、0.533、0.226、0.538、0.430、0.494,P<0.05)。多因素Logistic回归分析结果显示,T2DM病程〔OR=1.300,95%CI(1.173,1.441),P<0.001〕、LDL〔OR=2.565,95%CI(1.320,4.985),P=0.005〕、Scr〔OR=1.093,95%CI(1.046,1.143),P<0.001〕、NLR〔OR=2.565,95%CI(1.320,4.985),P=0.005〕和SII〔OR=1.011,95%CI(1.007,1.015),P<0.001〕均是老年T2DM患者并发DKD的影响因素。NLR诊断老年T2DM患者并发DKD的AUC为0.755〔95%CI(0.696,0.814)〕,最佳截断值为2.49,灵敏度和特异度分别为72.1%、70.5%;PLR诊断老年T2DM患者并发DKD的AUC为0.689〔95%CI(0.624,0.754)〕,最佳截断值为112.81,灵敏度和特异度分别为90.2%、43.8%;SII诊断老年T2DM患者并发DKD的AUC为0.836〔95%CI(0.791,0.881)〕,最佳截断值为492.08,灵敏度和特异度分别为80.5%、73.2%。 结论 T2DM病程、LDL、Scr、NLR、SII可能是老年T2DM患者并发DKD的影响因素;SII对社区老年T2DM患者并发DKD具有较高的临床诊断价值。