
Chinese General Practice ›› 2023, Vol. 26 ›› Issue (08): 917-926.DOI: 10.12114/j.issn.1007-9572.2022.0592
Special Issue: 心血管最新文章合集
• Original Research • Previous Articles Next Articles
Received:2022-04-12
Revised:2022-10-10
Published:2023-03-15
Online:2022-11-24
Contact:
HE Sen
通讯作者:
何森
作者简介:基金资助:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2022.0592
| 变量 | 定义 | 赋值原则 |
|---|---|---|
| 年龄 | 首次评估时的年龄[ | 连续性变量:岁 |
| 既往TE事件 | 根据CHA2DS2-VASc评分模型中的相关定义,为:缺血性脑卒中、短暂性脑缺血发作或外周动脉栓塞[ | 二分类变量:是/否 |
| 血管疾病 | 根据CHA2DS2-VASc评分模型中的相关定义,为:陈旧心肌梗死、外周动脉疾病或主动脉斑块[ | 二分类变量:是/否 |
| 高血压 | 血压值持续或非同日3次以上超过标准血压,即3次非同日收缩压≥140 mm Hg和/或舒张压≥90 mm Hg者,则诊断高血压;如既往诊断高血压,目前服用药物情况下血压处于参考范围,也诊断为高血压[ | 二分类变量:是/否 |
| 糖尿病 | 空腹血糖水平≥7 mmol/L,或有医生诊断的糖尿病史,或服用降糖药物[ | 二分类变量:是/否 |
| 心房颤动 | 诊断依据:存在心房颤动病史,或常规心电图提示心房颤动,或动态心电图提示心房颤动[ | 二分类变量:是/否 |
| MWT | 超声心动图测定的MWT | 连续性变量:mm |
| LA内径 | 超声心动图测定的LA前后径 | 连续性变量:mm |
| LVOTO | 左心室流出道静息压力阶差≥30 mm Hg[ | 二分类变量:是/否 |
| NYHA心功能分级 | Ⅰ级:有心脏病但体力活动不受限制;日常体力活动不引起明显的疲乏、心悸、呼吸困难、心绞痛等症状 | 二分类变量:Ⅲ/Ⅳ级为是,Ⅰ/Ⅱ级为否 |
| Ⅱ级:体力活动轻度受限;休息时无自觉症状,日常活动可出现较明显的上述症状,休息后很快缓解 | ||
| Ⅲ级:体力活动明显受限;休息时可无症状,轻于日常活动即引起上述症状,休息较长时间后方可缓解 | ||
| Ⅳ级:不能从事任何体力活动;休息时亦有心衰的症状,体力活动后明显加重 | ||
| LVEF | 超声心动图测定的左心室射血分数 | 连续性变量:% |
Table 1 Definitions and weight assignment principles of candidate variables
| 变量 | 定义 | 赋值原则 |
|---|---|---|
| 年龄 | 首次评估时的年龄[ | 连续性变量:岁 |
| 既往TE事件 | 根据CHA2DS2-VASc评分模型中的相关定义,为:缺血性脑卒中、短暂性脑缺血发作或外周动脉栓塞[ | 二分类变量:是/否 |
| 血管疾病 | 根据CHA2DS2-VASc评分模型中的相关定义,为:陈旧心肌梗死、外周动脉疾病或主动脉斑块[ | 二分类变量:是/否 |
| 高血压 | 血压值持续或非同日3次以上超过标准血压,即3次非同日收缩压≥140 mm Hg和/或舒张压≥90 mm Hg者,则诊断高血压;如既往诊断高血压,目前服用药物情况下血压处于参考范围,也诊断为高血压[ | 二分类变量:是/否 |
| 糖尿病 | 空腹血糖水平≥7 mmol/L,或有医生诊断的糖尿病史,或服用降糖药物[ | 二分类变量:是/否 |
| 心房颤动 | 诊断依据:存在心房颤动病史,或常规心电图提示心房颤动,或动态心电图提示心房颤动[ | 二分类变量:是/否 |
| MWT | 超声心动图测定的MWT | 连续性变量:mm |
| LA内径 | 超声心动图测定的LA前后径 | 连续性变量:mm |
| LVOTO | 左心室流出道静息压力阶差≥30 mm Hg[ | 二分类变量:是/否 |
| NYHA心功能分级 | Ⅰ级:有心脏病但体力活动不受限制;日常体力活动不引起明显的疲乏、心悸、呼吸困难、心绞痛等症状 | 二分类变量:Ⅲ/Ⅳ级为是,Ⅰ/Ⅱ级为否 |
| Ⅱ级:体力活动轻度受限;休息时无自觉症状,日常活动可出现较明显的上述症状,休息后很快缓解 | ||
| Ⅲ级:体力活动明显受限;休息时可无症状,轻于日常活动即引起上述症状,休息较长时间后方可缓解 | ||
| Ⅳ级:不能从事任何体力活动;休息时亦有心衰的症状,体力活动后明显加重 | ||
| LVEF | 超声心动图测定的左心室射血分数 | 连续性变量:% |
| 变量 | 未发生TE事件(n=471) | 发生TE事件(n=42) | χ2(Z)值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 267/204 | 16/26 | 4.664 | 0.031 |
| 年龄〔M(P25,P75),岁〕 | 57.0(44.0,66.0) | 66.0(51.3,73.0) | 12.027a | 0.001 |
| 既往TE事件〔n(%)〕 | 20(4.25) | 7(16.67) | — | 0.004 |
| 血管疾病〔n(%)〕 | 35(7.43) | 5(11.90) | — | 0.360 |
| 高血压〔n(%)〕 | 147(31.21) | 15(35.71) | 0.184 | 0.668 |
| 糖尿病〔n(%)〕 | 33(7.01) | 7(16.67) | — | 0.035 |
| 心房颤动〔n(%)〕 | 65(13.80) | 22(52.38) | 38.063 | <0.001 |
| MWT〔M(P25,P75),mm〕 | 19.0(17.0,22.0) | 18.0(16.0,21.0) | 2.466a | 0.116 |
| LA内径〔M(P25,P75),mm〕 | 40.0(35.0,45.0) | 43.0(38.2,46.0) | 6.955a | 0.008 |
| LVOTO〔n(%)〕 | 208(44.16) | 14(33.33) | 1.427 | 0.232 |
| NYHA心功能Ⅲ/Ⅳ级〔n(%)〕 | 163(34.61) | 13(30.95) | 0.095 | 0.758 |
| LVEF〔M(P25,P75),%〕 | 69.0(63.0,73.0) | 67.5(62.2,70.0) | 3.712a | 0.054 |
| 阿司匹林〔n(%)〕 | 84(17.83) | 10(23.81) | 0.564 | 0.453 |
| 氯吡格雷〔n(%)〕 | 28(5.94) | 3(7.14) | — | 0.733 |
| 华法林〔n(%)〕 | 35(7.43) | 10(23.81) | — | 0.002 |
Table 2 Baseline characteristics in hypertrophic cardiomyopathy patients with and without thrombotic events
| 变量 | 未发生TE事件(n=471) | 发生TE事件(n=42) | χ2(Z)值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 267/204 | 16/26 | 4.664 | 0.031 |
| 年龄〔M(P25,P75),岁〕 | 57.0(44.0,66.0) | 66.0(51.3,73.0) | 12.027a | 0.001 |
| 既往TE事件〔n(%)〕 | 20(4.25) | 7(16.67) | — | 0.004 |
| 血管疾病〔n(%)〕 | 35(7.43) | 5(11.90) | — | 0.360 |
| 高血压〔n(%)〕 | 147(31.21) | 15(35.71) | 0.184 | 0.668 |
| 糖尿病〔n(%)〕 | 33(7.01) | 7(16.67) | — | 0.035 |
| 心房颤动〔n(%)〕 | 65(13.80) | 22(52.38) | 38.063 | <0.001 |
| MWT〔M(P25,P75),mm〕 | 19.0(17.0,22.0) | 18.0(16.0,21.0) | 2.466a | 0.116 |
| LA内径〔M(P25,P75),mm〕 | 40.0(35.0,45.0) | 43.0(38.2,46.0) | 6.955a | 0.008 |
| LVOTO〔n(%)〕 | 208(44.16) | 14(33.33) | 1.427 | 0.232 |
| NYHA心功能Ⅲ/Ⅳ级〔n(%)〕 | 163(34.61) | 13(30.95) | 0.095 | 0.758 |
| LVEF〔M(P25,P75),%〕 | 69.0(63.0,73.0) | 67.5(62.2,70.0) | 3.712a | 0.054 |
| 阿司匹林〔n(%)〕 | 84(17.83) | 10(23.81) | 0.564 | 0.453 |
| 氯吡格雷〔n(%)〕 | 28(5.94) | 3(7.14) | — | 0.733 |
| 华法林〔n(%)〕 | 35(7.43) | 10(23.81) | — | 0.002 |
| 变量 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||||
|---|---|---|---|---|---|---|
| HR(95%CI) | P值 | β | HR(95%CI) | P值 | ||
| 性别(以男性为参照) | ||||||
| 女 | 1.85(0.99,3.45) | 0.053 | — | — | — | |
| 年龄(岁,以<50岁为参照) | ||||||
| 50~<70 | 1.69(0.73,3.92) | 0.221 | 0.329 | 1.39(0.59,3.28) | 0.452 | |
| ≥70 | 4.46(1.92,10.4) | <0.001 | 1.107 | 3.02(1.25,7.34) | 0.014 | |
| 既往TE事件 | 5.62(2.49,12.7) | <0.001 | 1.174 | 3.24(1.38,7.61) | 0.007 | |
| 血管疾病1 | .92(0.75,4.90) | 0.174 | — | — | — | |
| 高血压 | 1.30(0.69,2.44) | 0.420 | — | — | — | |
| 糖尿病 | 2.20(0.97,4.94) | 0.058 | — | — | — | |
| 心房颤动 | 5.95(3.24,10.90) | <0.001 | 1.472 | 4.36(2.31,8.23) | <0.001 | |
| MWT(mm,以<20.0 mm为参照) | ||||||
| 20.0~<25.0 | 0.98(0.51,1.88) | 0.949 | — | — | — | |
| 25.0~<30.0 | 0.49(0.12,2.09) | 0.338 | — | — | — | |
| ≥30.0 | 0(0,Inf) | 0.996 | — | — | — | |
| LA内径(mm,以<35.0 mm为参照) | ||||||
| 35.0~<40.0 | 1.52(0.47,4.95) | 0.484 | — | — | — | |
| 40.0~<45.0 | 3.14(1.03,9.55) | 0.044 | — | — | — | |
| ≥45.0 | 2.80(0.93,8.44) | 0.067 | — | — | — | |
| LVOTO | 0.72(0.38,1.37) | 0.314 | — | — | — | |
| NYHA心功能分级(以Ⅰ/Ⅱ级为参照) | ||||||
| Ⅲ/Ⅳ级 | 1.05(0.54,2.02) | 0.887 | — | — | — | |
| LVEF(%,以<50.0%为参照) | ||||||
| 50.0~<70.0 | 0.56(0.17,1.86) | 0.344 | -0.981 | 0.37(0.11,1.29) | 0.120 | |
| ≥70.0 | 0.31(0.09,1.08) | 0.067 | -1.407 | 0.24(0.07,0.91) | 0.035 | |
| 阿司匹林 | 1.35(0.67,2.76) | 0.402 | — | — | — | |
| 氯吡格雷 | 1.26(0.39,4.07) | 0.702 | — | — | — | |
| 华法林 | 4.33(2.11,8.89) | <0.001 | — | — | — | |
Table 3 Univariate and multvariate Cox regression analyses for factors predicting the risk of thrombotic events in hypertrophic cardiomyopathy patients
| 变量 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||||
|---|---|---|---|---|---|---|
| HR(95%CI) | P值 | β | HR(95%CI) | P值 | ||
| 性别(以男性为参照) | ||||||
| 女 | 1.85(0.99,3.45) | 0.053 | — | — | — | |
| 年龄(岁,以<50岁为参照) | ||||||
| 50~<70 | 1.69(0.73,3.92) | 0.221 | 0.329 | 1.39(0.59,3.28) | 0.452 | |
| ≥70 | 4.46(1.92,10.4) | <0.001 | 1.107 | 3.02(1.25,7.34) | 0.014 | |
| 既往TE事件 | 5.62(2.49,12.7) | <0.001 | 1.174 | 3.24(1.38,7.61) | 0.007 | |
| 血管疾病1 | .92(0.75,4.90) | 0.174 | — | — | — | |
| 高血压 | 1.30(0.69,2.44) | 0.420 | — | — | — | |
| 糖尿病 | 2.20(0.97,4.94) | 0.058 | — | — | — | |
| 心房颤动 | 5.95(3.24,10.90) | <0.001 | 1.472 | 4.36(2.31,8.23) | <0.001 | |
| MWT(mm,以<20.0 mm为参照) | ||||||
| 20.0~<25.0 | 0.98(0.51,1.88) | 0.949 | — | — | — | |
| 25.0~<30.0 | 0.49(0.12,2.09) | 0.338 | — | — | — | |
| ≥30.0 | 0(0,Inf) | 0.996 | — | — | — | |
| LA内径(mm,以<35.0 mm为参照) | ||||||
| 35.0~<40.0 | 1.52(0.47,4.95) | 0.484 | — | — | — | |
| 40.0~<45.0 | 3.14(1.03,9.55) | 0.044 | — | — | — | |
| ≥45.0 | 2.80(0.93,8.44) | 0.067 | — | — | — | |
| LVOTO | 0.72(0.38,1.37) | 0.314 | — | — | — | |
| NYHA心功能分级(以Ⅰ/Ⅱ级为参照) | ||||||
| Ⅲ/Ⅳ级 | 1.05(0.54,2.02) | 0.887 | — | — | — | |
| LVEF(%,以<50.0%为参照) | ||||||
| 50.0~<70.0 | 0.56(0.17,1.86) | 0.344 | -0.981 | 0.37(0.11,1.29) | 0.120 | |
| ≥70.0 | 0.31(0.09,1.08) | 0.067 | -1.407 | 0.24(0.07,0.91) | 0.035 | |
| 阿司匹林 | 1.35(0.67,2.76) | 0.402 | — | — | — | |
| 氯吡格雷 | 1.26(0.39,4.07) | 0.702 | — | — | — | |
| 华法林 | 4.33(2.11,8.89) | <0.001 | — | — | — | |
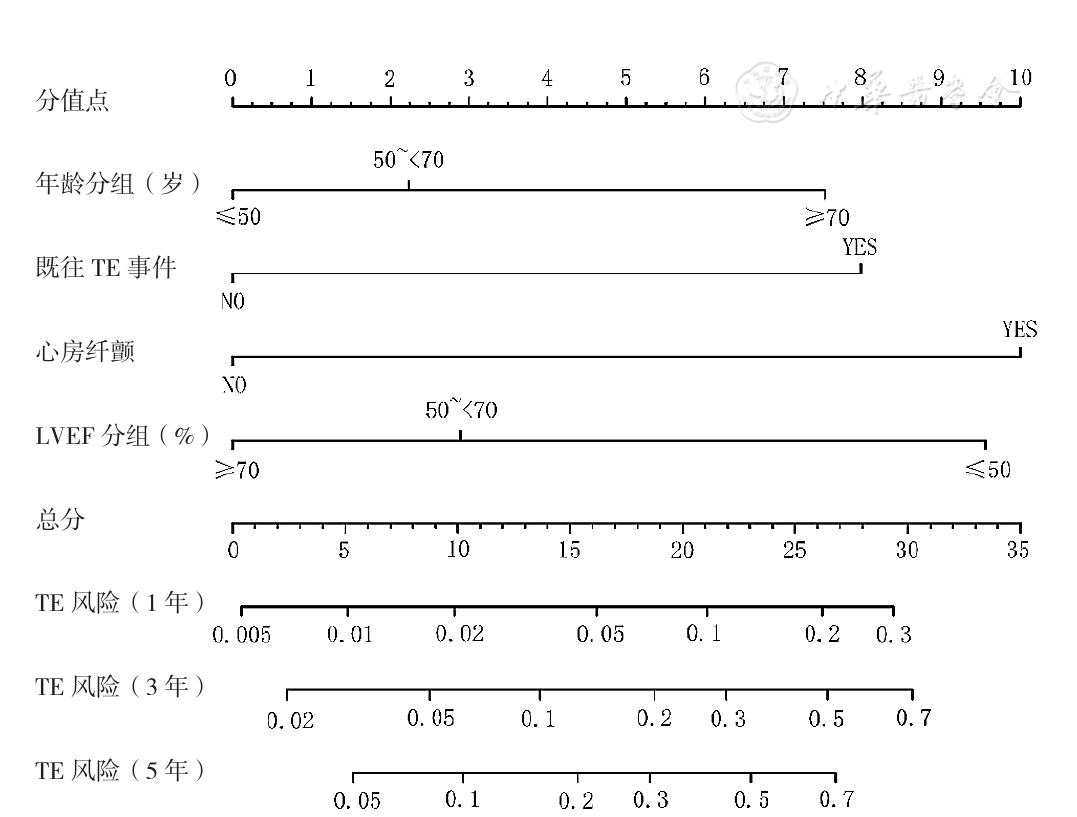
Figure 1 Nomangram for risk prediction of thrombotic events in hypertrophic cardiomyopathy patients
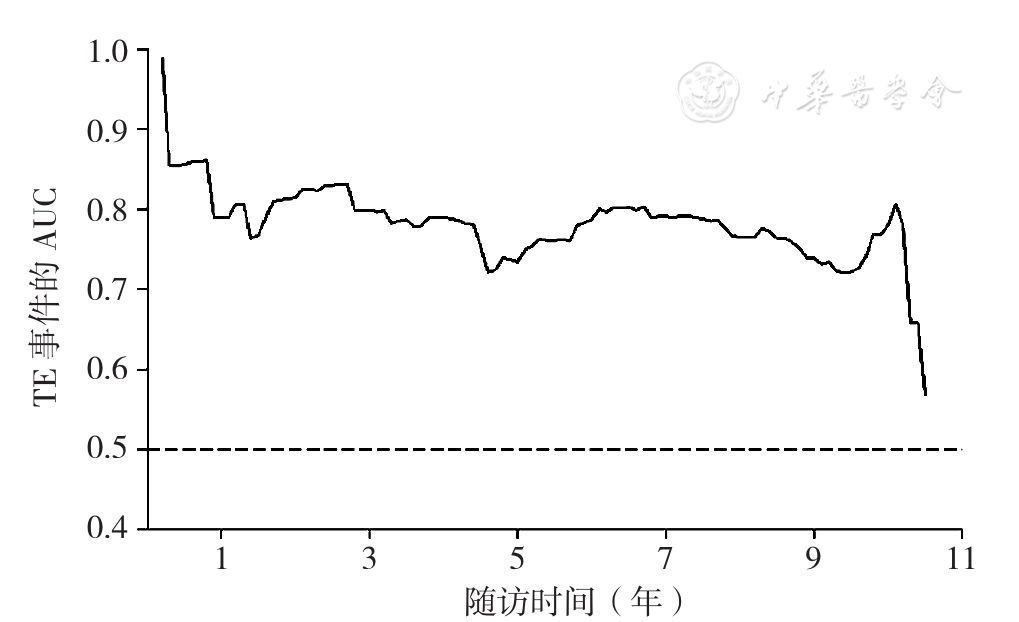
Figure 2 Predictive power of SAAE score for 1-,3- and 5-year risk of thrombotic events in the whole study population
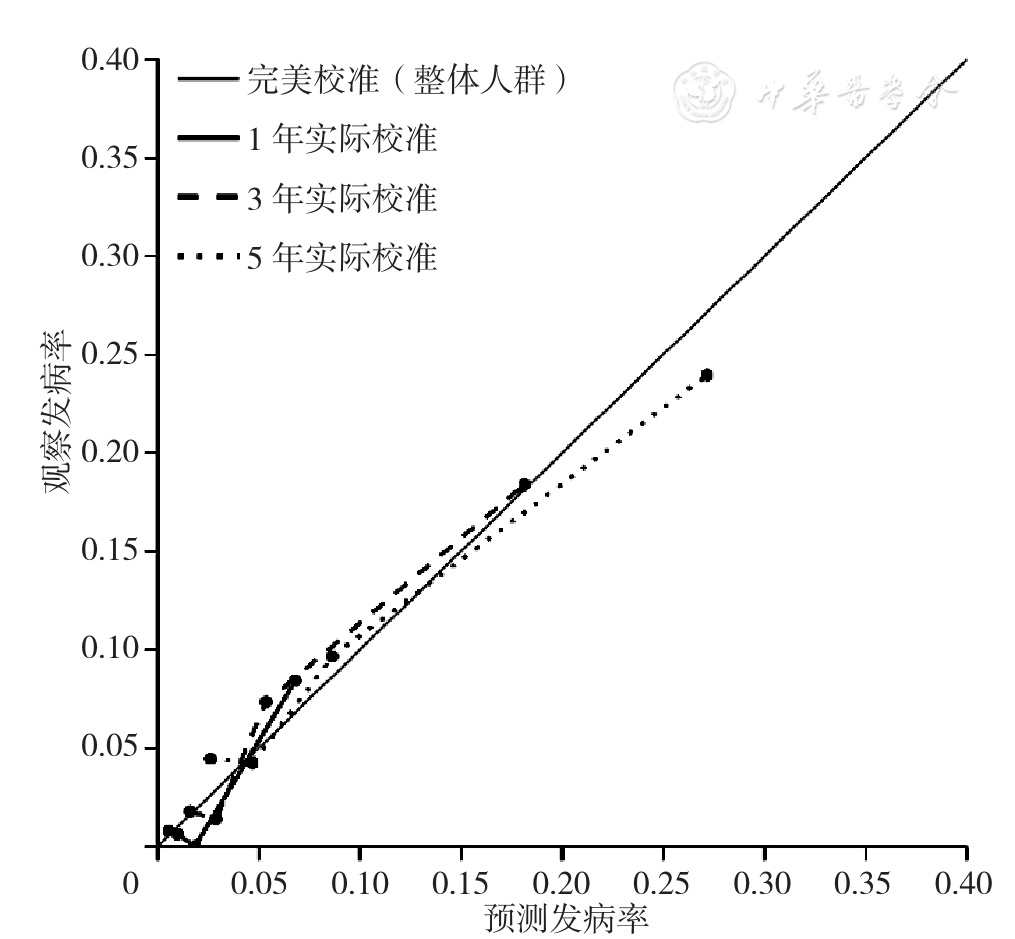
Figure 3 Calibration plots for predicted versus observed 1-,3-,5-year risk of thrombotic events for whole study population
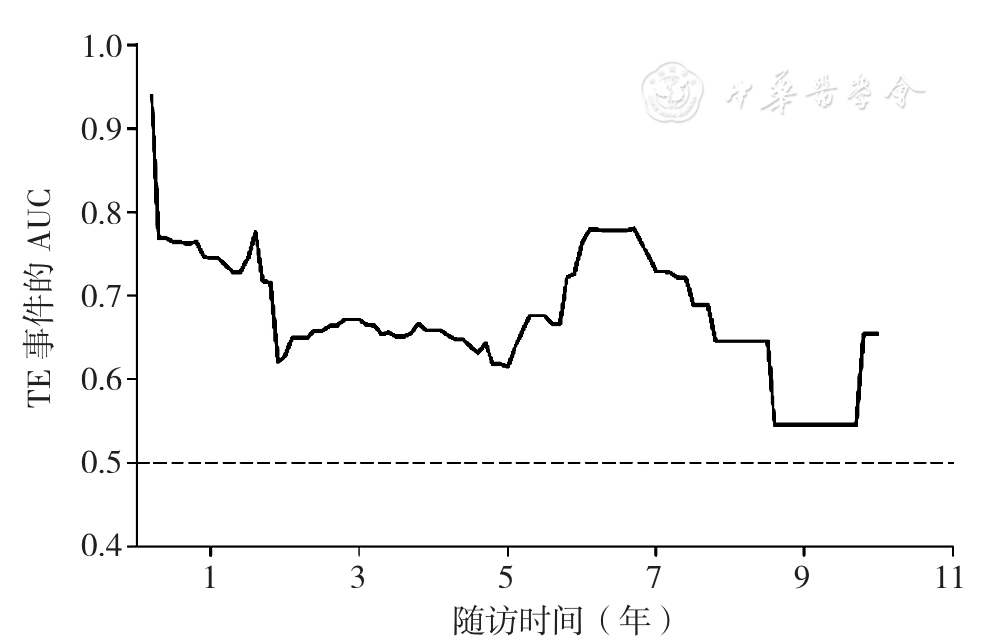
Figure 4 Predictive power of SAAE score for 1-,3-,5-year risk of thrombotic events for hypertrophic cardiomyopathy patients with atrial fibrillation
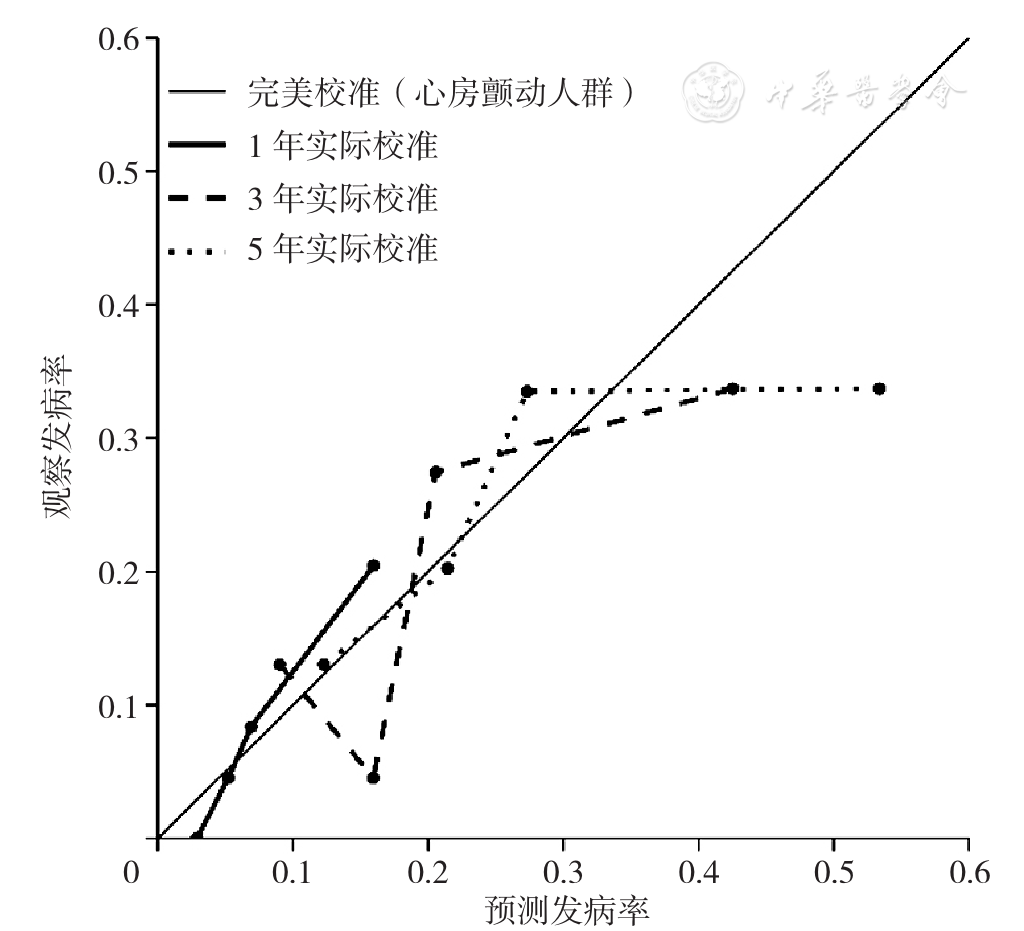
Figure 5 Calibration plots for predicted versus observed 1-,3-,5-year risk of thrombotic events for hypertrophic cardiomyopathy patients with atrial fibrillation
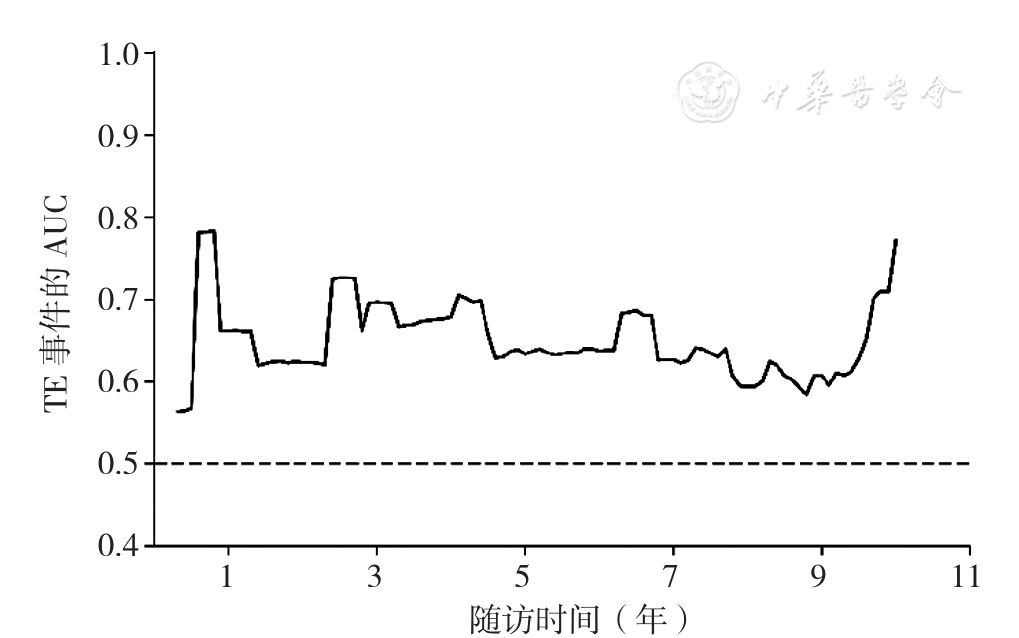
Figure 6 Predictive power of SAAE score for 1-,3- and 5-year risk of thrombotic events for hypertrophic cardiomyopathy patients without atrial fibrillation
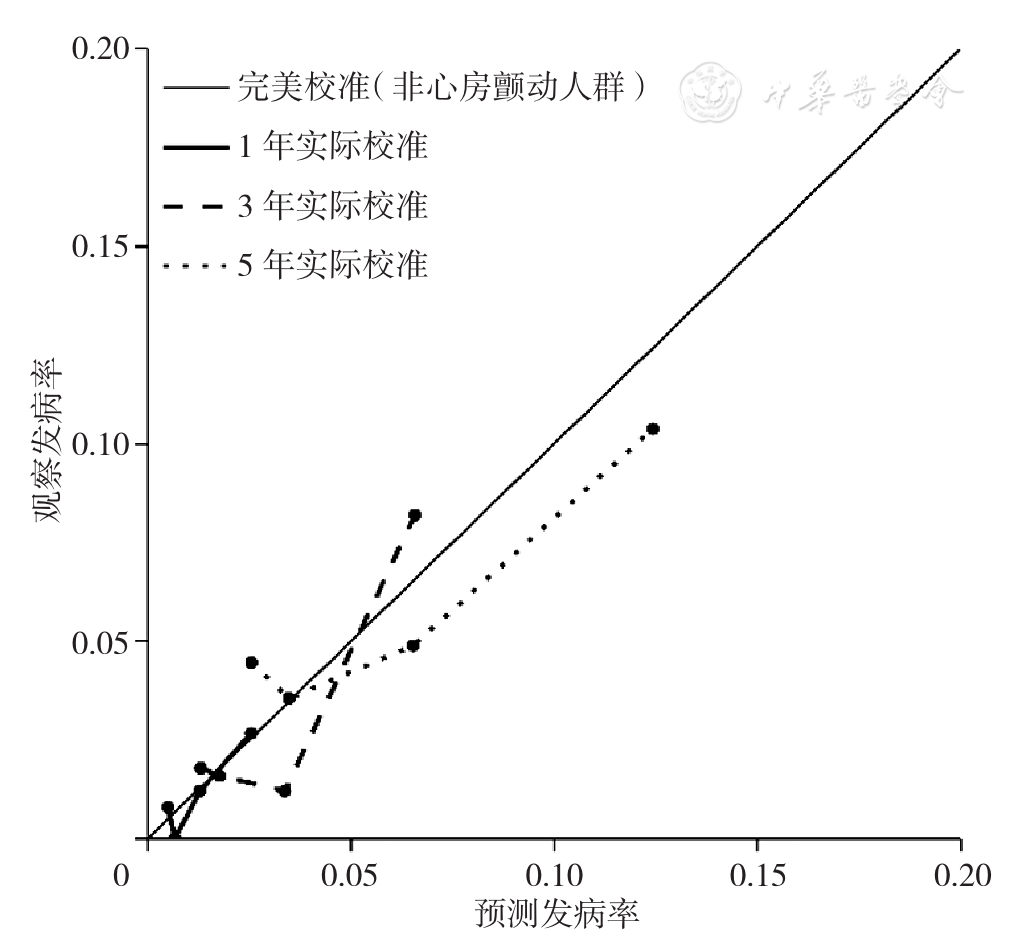
Figure 7 Calibration plots for predicted versus observed 1-,3-,5-year risk of thrombotic events for hypertrophic cardiomyopathy patients without atrial fibrillation
| 分类 | 低风险 | 中风险 | 高风险 |
|---|---|---|---|
| 整体人群 | <7.56 | 7.56~<17.38 | ≥17.38 |
| 心房颤动人群 | <17.56 | 17.56~<21.42 | ≥21.42 |
| 非心房颤动人群 | <3.87 | 3.87~<11.25 | ≥11.25 |
Table 4 Cutoff points of SAAE score for low,moderate and high risk of thrombotic events in different populations
| 分类 | 低风险 | 中风险 | 高风险 |
|---|---|---|---|
| 整体人群 | <7.56 | 7.56~<17.38 | ≥17.38 |
| 心房颤动人群 | <17.56 | 17.56~<21.42 | ≥21.42 |
| 非心房颤动人群 | <3.87 | 3.87~<11.25 | ≥11.25 |
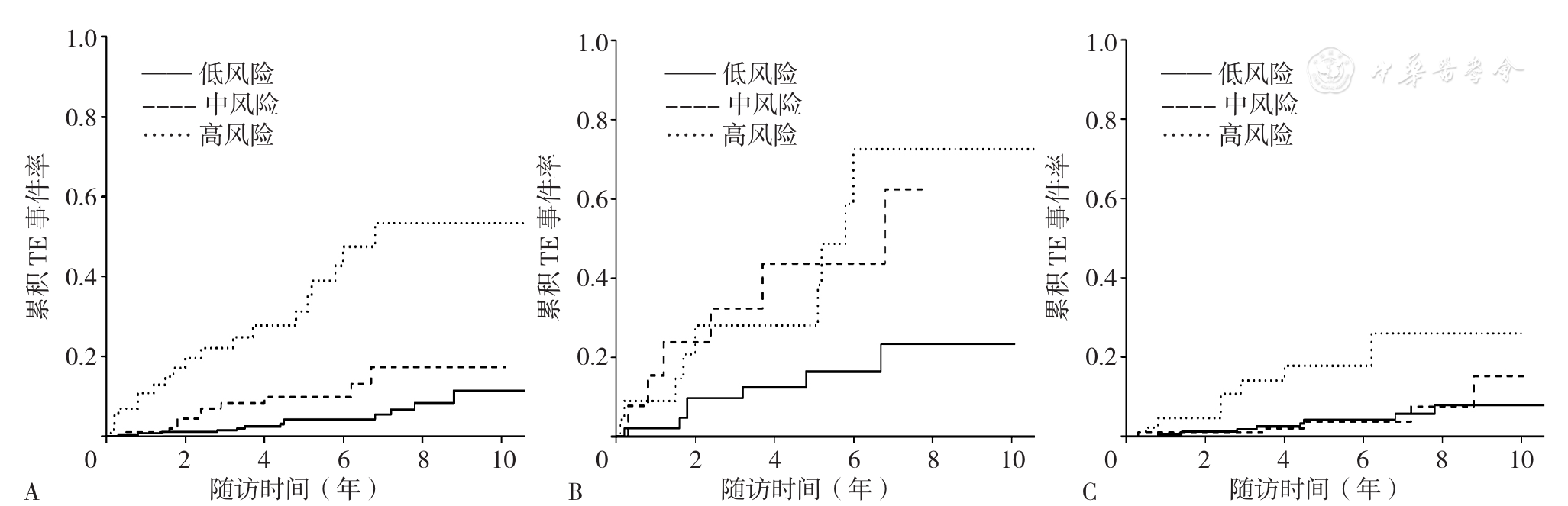
Figure 8 Kaplan-Meier analysis showing cumulative thrombotic events in hypertrophic cardiomyopathy patients with low,moderate or high thrombotic risk predicted by SAAE score
| 人群 | 评分模型 | 整体 | 1年 | 3年 | 5年 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | ||
| 整体人群 | SAAE score | 0.757 | 0.013 | 0.790 | 0.413 | 0.799 | 0.137 | 0.735 | 0.117 |
| HCM Risk-CVA | 0.671 | 0.710 | 0.715 | 0.670 | |||||
| 心房颤动人群 | SAAE score | 0.670 | 0.110 | 0.745 | 0.112 | 0.671 | 0.162 | 0.616 | 0.738 |
| HCM Risk-CVA | 0.560 | 0.557 | 0.538 | 0.587 | |||||
| 非心房颤动人群 | SAAE score | 0.624 | 0.549 | 0.661 | 0.828 | 0.697 | 0.899 | 0.634 | 0.644 |
| HCM Risk-CVA | 0.592 | 0.696 | 0.710 | 0.603 | |||||
Table 5 Comparisons between SAAE score and HCM Risk-CVA score for predicting the risk of thrombotic events in hypertrophic cardiomyopathy
| 人群 | 评分模型 | 整体 | 1年 | 3年 | 5年 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | ||
| 整体人群 | SAAE score | 0.757 | 0.013 | 0.790 | 0.413 | 0.799 | 0.137 | 0.735 | 0.117 |
| HCM Risk-CVA | 0.671 | 0.710 | 0.715 | 0.670 | |||||
| 心房颤动人群 | SAAE score | 0.670 | 0.110 | 0.745 | 0.112 | 0.671 | 0.162 | 0.616 | 0.738 |
| HCM Risk-CVA | 0.560 | 0.557 | 0.538 | 0.587 | |||||
| 非心房颤动人群 | SAAE score | 0.624 | 0.549 | 0.661 | 0.828 | 0.697 | 0.899 | 0.634 | 0.644 |
| HCM Risk-CVA | 0.592 | 0.696 | 0.710 | 0.603 | |||||
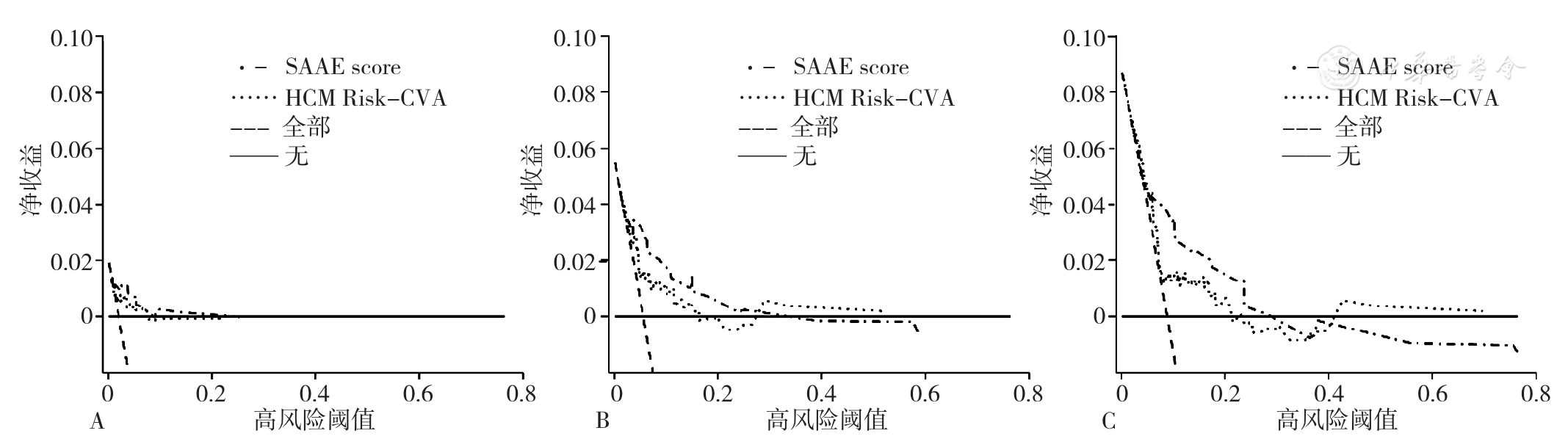
Figure 9 Decision curve analysis of SAAE score and HCM Risk-CVA score for predicting the risk of thrombotic events in hypertrophic cardiomyopathy at different time points
| [1] |
|
| [2] |
|
| [3] |
吴兆苏,姚崇华,赵冬. 我国人群脑卒中发病率、死亡率的流行病学研究[J]. 中华流行病学杂志,2003,24(3):236-239.
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
《中国高血压防治指南》修订委员会. 中国高血压防治指南2018年修订版[J]. 心脑血管病防治,2019,19(1):1-44. DOI:10.3969/j.issn.1009-816X.2019.01.001.
|
| [21] |
American Diabetes Association. Standards of medical care in diabetes—2010[J]. Diabetes Care,2010,33(Suppl 1):S11-61. DOI:10.2337/dc10-S011.
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
顾俊,贾锋鹏,封盼攀. CHADS2与CHA2DS2-VASc评分对非瓣膜病房颤患者左房血栓的风险评估[J]. 南方医科大学学报,2014,34(11):1601-1605.
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [1] | ZHANG Aili, HOU Qiqi, HAN Quanle, ZHANG Boheng, ZHANG Jiawei, CAO Hongxia, ZHANG Chao, CHEN Shuohua, WU Shouling, LI Kangbo. Correlation between Atrial Fibrillation and the Risk of New-onset Chronic Kidney Disease in Northern Chinese Population [J]. Chinese General Practice, 2023, 26(36): 4521-4526. |
| [2] | BAI Haiwei, MI Xiaokun, LIU Qingrui, ZHU Lin, WANG Yingnan, LIU Junyan, HAN Ying. Predictive Value of Serum Uric Acid in Perioperative Acute Ischemic Stroke in Patients with Non-small Cell Lung Cancer [J]. Chinese General Practice, 2023, 26(36): 4545-4551. |
| [3] | WEI Zongbo, LONG Bingcai, WANG Xiongjiang, LIANG Yingye, TANG Hongliang, XIA Tian, LU Dongming. Effect and Mechanism of Pivot Meridian Massage on TLR8/ERK Signaling Pathway and LncRNA-GAS5 in Rats with Neuropathic Pain [J]. Chinese General Practice, 2023, 26(36): 4565-4574. |
| [4] | LIU Ailing, ZHOU Jingjing, LI Chengcheng, HE Kaiyue, LIANG Shanshan, ZHOU Shangcheng. Analysis of the Disease Burden Trends and Death Projections for Esophageal Cancer Attributable to Tobacco in China from 1990 to 2019 [J]. Chinese General Practice, 2023, 26(36): 4587-4594. |
| [5] | LU Lixia, WANG Rongqi. Advances in Liver Cancer Screening and Health Surveillance Management in Primary Care Institutions [J]. Chinese General Practice, 2023, 26(36): 4505-4509. |
| [6] | Expert Consensus Writing Group of Integrated Traditional Chinese and Western Medicine Management for Chronic Obstructive Pulmonary Disease. Expert Consensus on Integrated Traditional Chinese and Western Medicine Management for Chronic Obstructive Pulmonary Disease (2023 Edition) [J]. Chinese General Practice, 2023, 26(35): 4359-4371. |
| [7] | LU Yihan, WANG Jiwen, SUN Yue, FENG Runrun, HAN Yufei, SONG Zhenzhen, SUN Ying, DAI Huihua, CHEN Xing. Risk Factors and Maternal and Neonatal Outcomes of Pregnant Women with Total Labor over 24 Hours [J]. Chinese General Practice, 2023, 26(35): 4459-4463. |
| [8] | XIE Xuemei, GAO Jing, BAI Dingxi, LU Xianying, HE Jiali, LI Yue. Current Status of Polypharmacy in the Elderly and Its Influencing Factors: a Meta-analysis [J]. Chinese General Practice, 2023, 26(35): 4394-4403. |
| [9] | XU Man, AN Zhuoling, ZHANG Yuhui, MA Zhuo. Current Situation of Potentially Inappropriate Medication in Older Cancer Patients and Strategies to Address It [J]. Chinese General Practice, 2023, 26(35): 4382-4387. |
| [10] | LIU Linbo, LIAO Zhijie, YANG Wenfan, BAI Dandan, WANG Dongmei, SHI Sen. Analysis of Gender Differences in Peripheral Arterial Disease Prevalence from 1990 to 2019 in China [J]. Chinese General Practice, 2023, 26(35): 4425-4432. |
| [11] | LIU Puqing, CHEN Jingwen, SHOU Zhangxuan. Evaluation of Potentially Inappropriate Medication of Direct Oral Anticoagulant in Hospitalized Elderly Patients with Non-valvular Atrial Fibrillation Based on Beers Criteria [J]. Chinese General Practice, 2023, 26(35): 4388-4393. |
| [12] | ZHONG Pingping, NAN Yayun, PENG Linlin, ZHOU Yuting, CHEN Qiong. A Bibliometrics Analysis of Polypharmacy in the Elderly from 2003 to 2022 [J]. Chinese General Practice, 2023, 26(35): 4404-4411. |
| [13] | LUO Weigang, YIN Yuanyuan, LIU Wanhu, XU Yuzhu, CAO Xiaoyun, BU Wei, ZHANG Lingyan, REN Huiling. Correlation of Triglyceride Glucose Index with Early Neurological Deterioration in Patients with Single Subcortical Infarction [J]. Chinese General Practice, 2023, 26(35): 4419-4424. |
| [14] | CHENG Hao, ZHOU Jinchi, LIU Xi, KANG Lin, FAN Ahui, DOU Weijia, LIU Zhenxiong. Risk Factors Analysis and Risk Prediction Model Establishment for Rebleeding Events within 3 Years after Endoscopic Treatment of Gastroesophageal Varices in Liver Cirrhosis Patients [J]. Chinese General Practice, 2023, 26(35): 4446-4452. |
| [15] | ZHANG Qian, LI Shu, LI Pengmei. Interpretation of the 2023 AGS Beers Criteria: Potentially Inappropriate Medication Use in Older Adults [J]. Chinese General Practice, 2023, 26(35): 4372-4381. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||