中国全科医学 ›› 2026, Vol. 29 ›› Issue (06): 718-725.DOI: 10.12114/j.issn.1007-9572.2025.0254
雷淳心1, 张曦亚1, 张燕1, 陈嘉琪1, 刘子菡1, 罗静2,*( ), 陶庆文2,*()
), 陶庆文2,*()
LEI Chunxin1, ZHANG Xiya1, ZHANG Yan1, CHEN Jiaqi1, LIU Zihan1, LUO Jing2,*(), TAO Qingwen2,*()
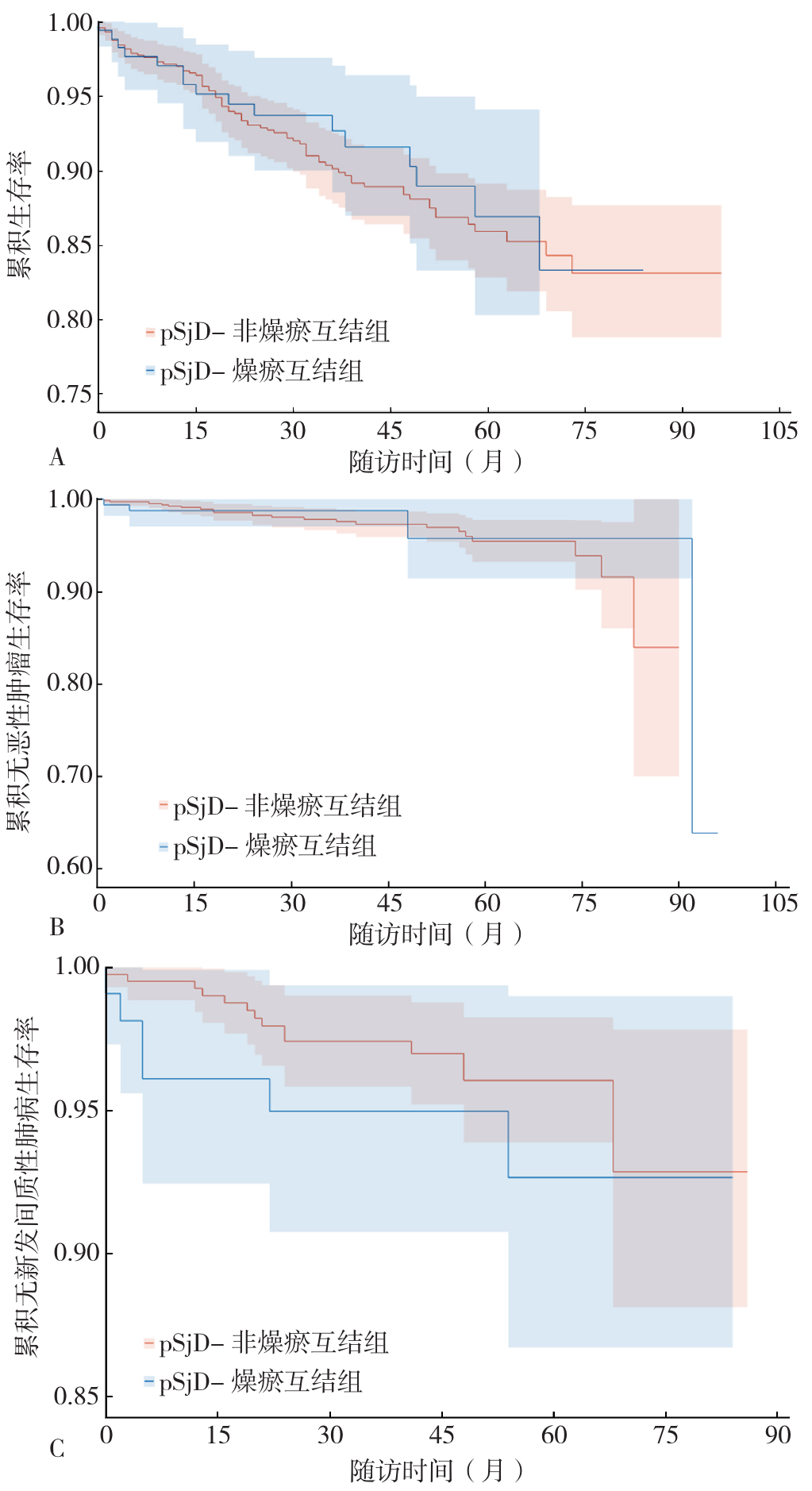
摘要: 背景 原发性干燥综合征(pSjD)是一种以淋巴细胞浸润外分泌腺体为特征的慢性自身免疫病,主要表现为口干、眼干,并可累及多系统。流行病学调查显示其患病率为0.06%~0.08%,且逐年上升。近年来中医专家共识提出燥瘀互结证为常见证型之一,但其临床特征、影响因素及预后情况尚缺乏系统研究。 目的 探索pSjD-燥瘀互结证患者的中西医临床特点、影响因素及预后情况。 方法 纳入2017—2022年就诊于中日友好医院的970例pSjD患者,分为pSjD-燥瘀互结组(185例)和pSjD-非燥瘀互结组(785例)。比较2组患者一般资料、临床症状、实验室指标及疾病活动度(ESSDAI)评分差异,采用多因素Logistic回归分析pSjD-燥瘀互结证的影响因素。生存结局(包括全因死亡、恶性肿瘤及间质性肺疾病)采用Kaplan-Meier生存曲线分析,组间差异使用Log-rank检验评估。 结果 与pSjD-非燥瘀互结组相比,pSjD-燥瘀互结组女性比例更高、病程更长、就诊年龄和发病年龄更小(P<0.05)。pSjD-燥瘀互结组患者中,前五位高频主诉症状依次为口干(75.1%)、眼干(75.1%)、关节痛(54.6%)、乏力(43.2%)、猖獗齿(33.5%)。pSjD-燥瘀互结组患者口干、关节痛、雷诺现象、淋巴结肿大、咳嗽、呼吸困难、腮腺肿大、紫癜样皮疹、关节炎、合并出血发生比例高于pSjD-非燥瘀互结组,咳嗽和呼吸困难发生比例低于pSjD-非燥瘀互结组(P<0.05)。多因素Logistic回归分析结果显示,就诊年龄增大(OR=0.979,95%CI=0.965~0.993,P=0.004)、血小板计数水平升高(OR=0.997,95%CI=0.994~0.999,P=0.007)为pSjD患者发生燥瘀互结证的独立保护因素,抗核糖核蛋白(RNP)抗体阳性(OR=2.352,95%CI=1.305~4.238,P=0.004)、抗着丝点蛋白B(CENP-B)抗体阳性(OR=2.490,95%CI=1.404~4.415,P=0.002)、抗β2-糖蛋白1(β2GP1)抗体阳性(OR=2.269,95%CI=1.057~4.872,P=0.036)以及ESSDAI评分升高(OR=1.037,95%CI=1.011~1.064,P=0.006)为pSjD患者发生燥瘀互结证的独立危险因素。Kaplan-Meier生存曲线分析结果显示,pSjD-燥瘀互结组与pSjD-非燥瘀互结组的总体死亡率、肿瘤及新发间质性肺疾病发生率比较,差异均无统计学意义(P>0.05)。 结论 pSjD-燥瘀互结证患者病情发展缠绵、ESSDAI评分更高、血液系统受累更显著,但合并ILD比例小。就诊年龄增大、血小板计数水平升高可能是pSjD患者发生燥瘀互结证的独立保护因素,抗RNP抗体阳性、抗CENP-B抗体阳性、抗β2GP1抗体阳性以及ESSDAI评分升高可能是pSjD患者发生燥瘀互结证的独立危险因素。pSjD-燥瘀互结组与pSjD-非燥瘀互结组的总体死亡率、肿瘤及新发ILD发生率无明显差异。
中图分类号: