中国全科医学 ›› 2025, Vol. 28 ›› Issue (26): 3307-3313.DOI: 10.12114/j.issn.1007-9572.2024.0300
所属专题: 内分泌代谢性疾病最新文章合辑; 肾脏疾病最新文章合辑
张睿敏1,2, 董哲毅1, 李爽1, 王倩1, 陈香美1,2,*( )
)
ZHANG Ruimin1,2, DONG Zheyi1, LI Shuang1, WANG Qian1, CHEN Xiangmei1,2,*()
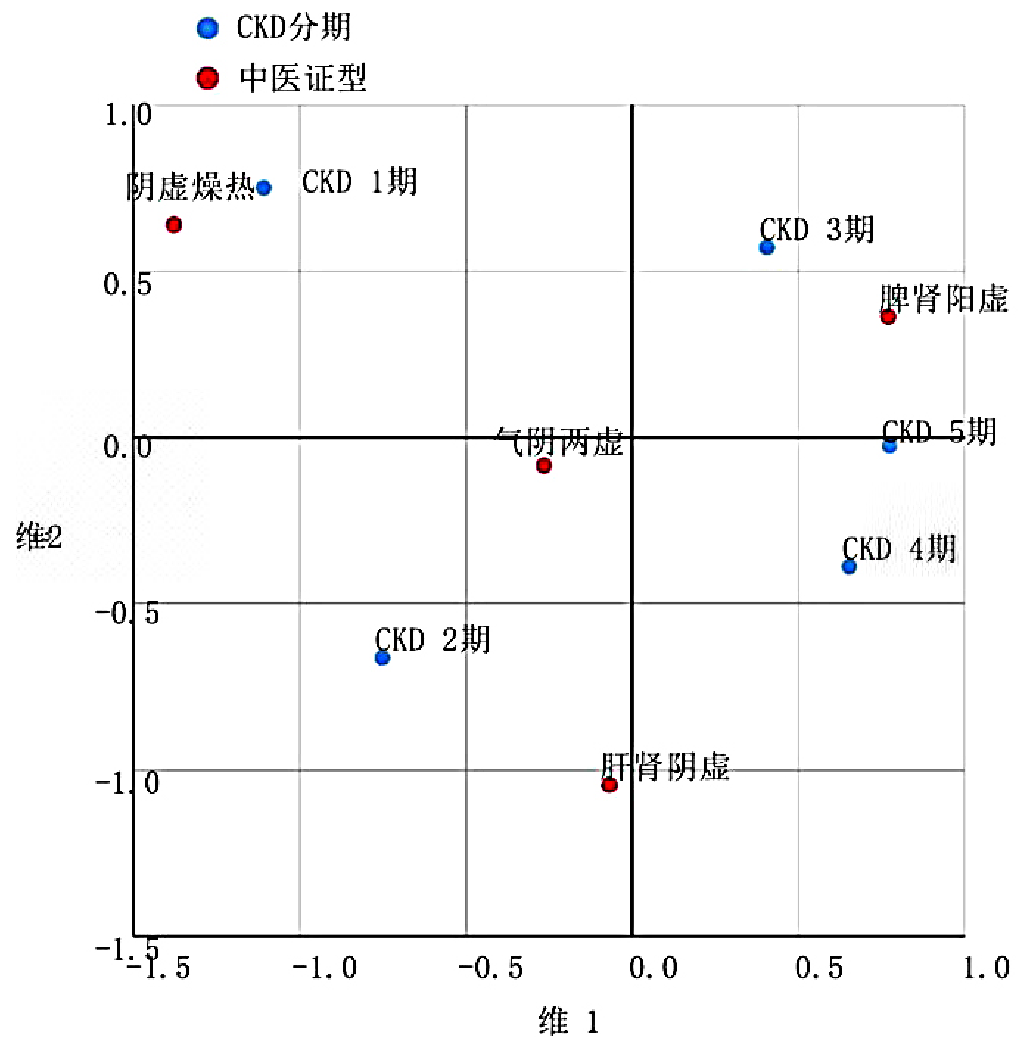
摘要: 背景 糖尿病肾病(DN)是糖尿病常见的微血管并发症,同时也是终末期肾脏病的主要原因之一。肾活检是DN病理诊断的金标准。既往关于DN的中医相关因素研究大多缺乏肾活检依据,可能导致纳入人群不够精准。 目的 探讨DN患者中医证型的分布规律及伴大量蛋白尿、肾功能不全的相关中医证素,为DN病机研究提供中医思路。 方法 纳入2022年1月—2024年1月在中国人民解放军总医院第一医学中心肾脏病医学部确诊为2型糖尿病且经肾活检诊断为单纯DN的78例患者的中医信息及临床资料。探索中医证型的临床特征及分布规律,采用二元Logistic回归探讨DN伴大量蛋白尿(24 h尿蛋白定量>3.5 g)、估算肾小球滤过率(eGFR)<60 mL·min-1·(1.73 m2)-1的相关中医证素。 结果 将DN患者按照慢性肾脏病(CKD)分期进行分组:CKD 1期组11例,CKD 2期组19例,CKD 3期组22例,CKD 4期组21例,CKD 5期组5例。不同CKD分期组间的血红蛋白、eGFR、血清白蛋白、血清肌酐、血清尿素氮、24 h尿蛋白定量比较,差异均有统计学意义(P<0.05)。按照中医证型分类DN患者可分为:阴虚燥热证11例,气阴两虚证23例,肝肾阴虚证15例,脾肾阳虚证29例。不同中医证型患者的血红蛋白、eGFR、血清总蛋白、血清白蛋白、血清肌酐、血清尿素氮比较,差异均有统计学意义(P<0.05)。CKD 1~5期组中医证型分布比较,差异有统计学意义(P<0.05),其中CKD 1期组阴虚燥热证、气阴两虚证所占比例较多,分别为45.5%(5/11)、27.3%(3/11);CKD 2期组气阴两虚证、肝肾阴虚证所占比例较多,分别为42.1%(8/19)、31.6%(6/19);CKD 3期组脾肾阳虚证、气阴两虚证所占比例较多,分别为54.5%(12/22)、31.8%(7/22);CKD 4期组脾肾阳虚证、肝肾阴虚证所占比例较多,分别为52.4%(11/21)、28.6%(6/21);CKD 5期组脾肾阳虚证所占比例最多(60.0%,3/5)。对应性分析显示,阴虚燥热证、气阴两虚证、脾肾阳虚证分别对应CKD分期的1、2、5期。阳虚证(OR=3.545,95%CI=1.270~9.895,P=0.016)、病位心(OR=3.208,95%CI=1.082~9.511,P=0.035)是DN伴大量蛋白尿的影响因素。阳虚证(OR=3.000,95%CI=1.141~7.890,P=0.026)是DN伴eGFR<60 mL·min-1·(1.73 m2)-1的影响因素。 结论 随着CKD分期的加重,DN中医证型大致呈阴虚、气虚、阳虚的转变规律。阳虚证、病位心是DN伴大量蛋白尿的影响因素,阳虚证是DN伴eGFR<60 mL·min-1·(1.73 m2)-1的影响因素。中医辨证结合现代医学,有利于把握DN病机,发挥中西医结合诊疗的优势。
中图分类号: