中国全科医学 ›› 2026, Vol. 29 ›› Issue (09): 1121-1128.DOI: 10.12114/j.issn.1007-9572.2024.0199
所属专题: 社区卫生服务最新研究合辑; 心血管最新文章合辑
杨玲*( ), 杜雪平
), 杜雪平
YANG Ling*(), DU Xueping
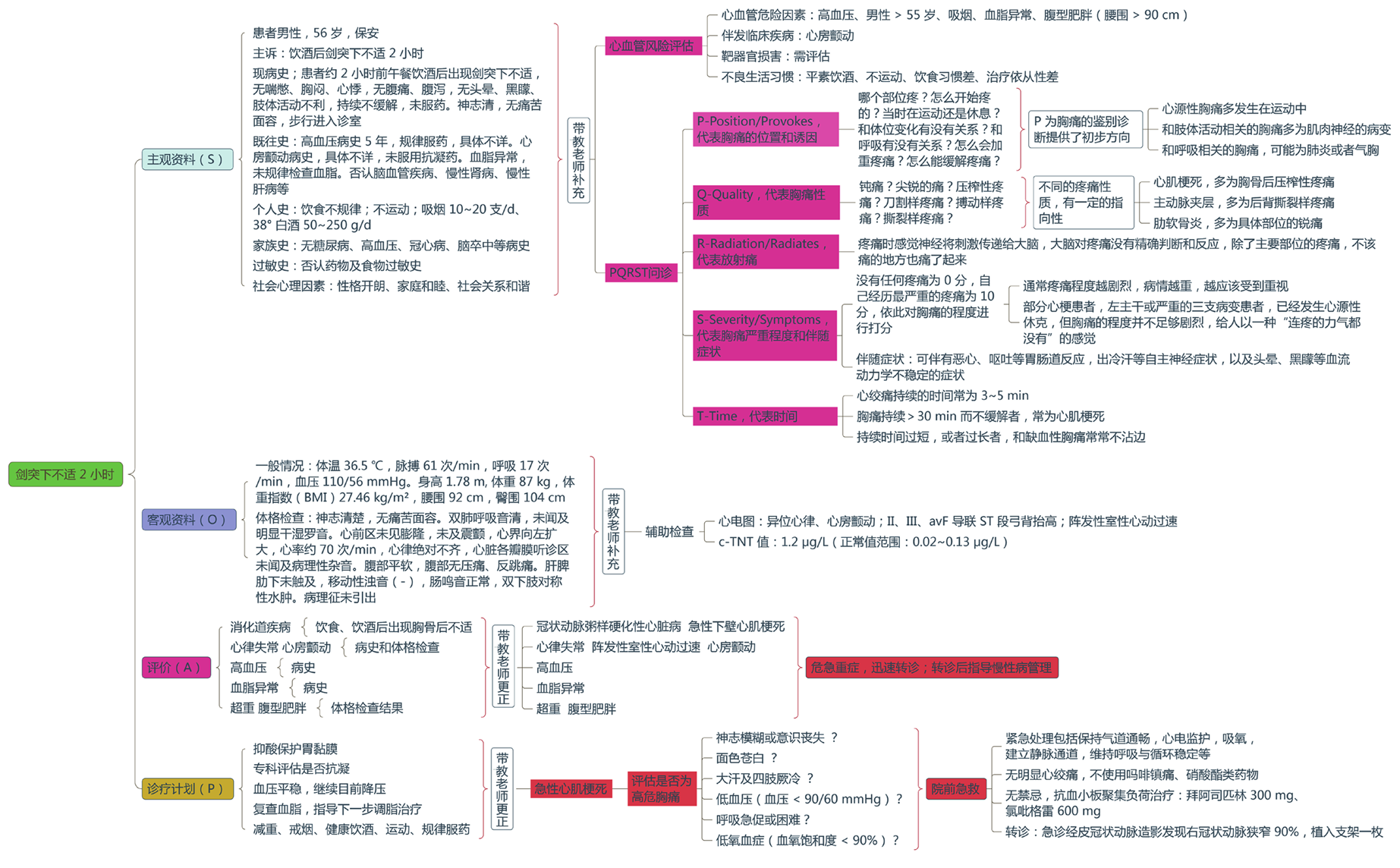
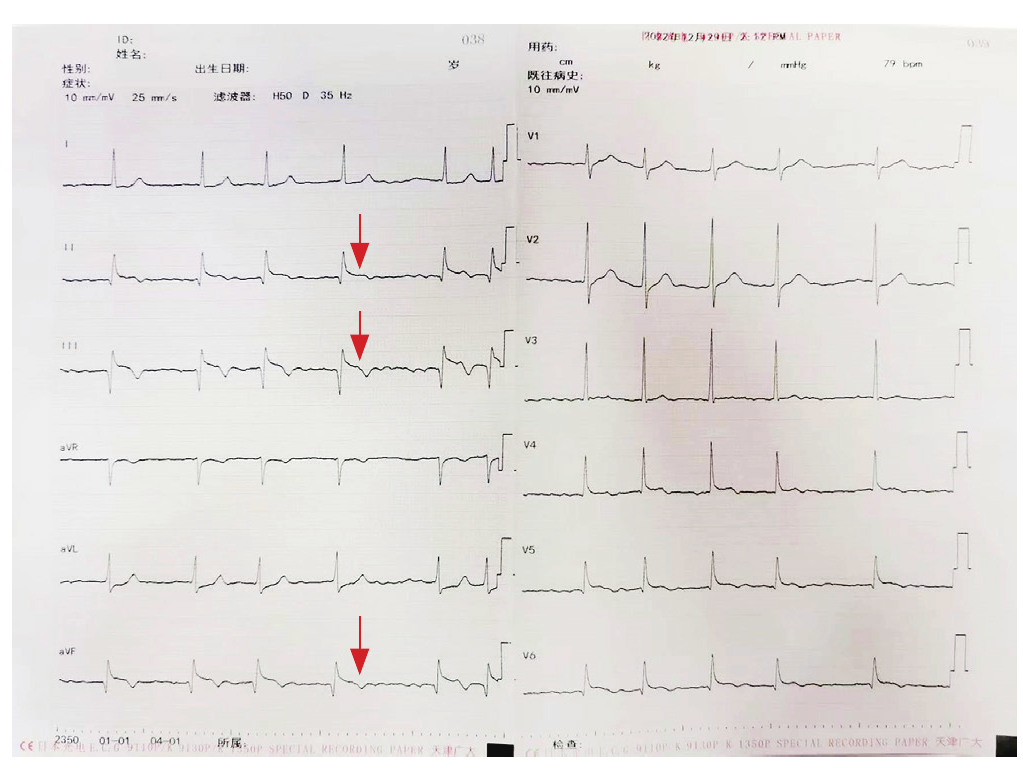
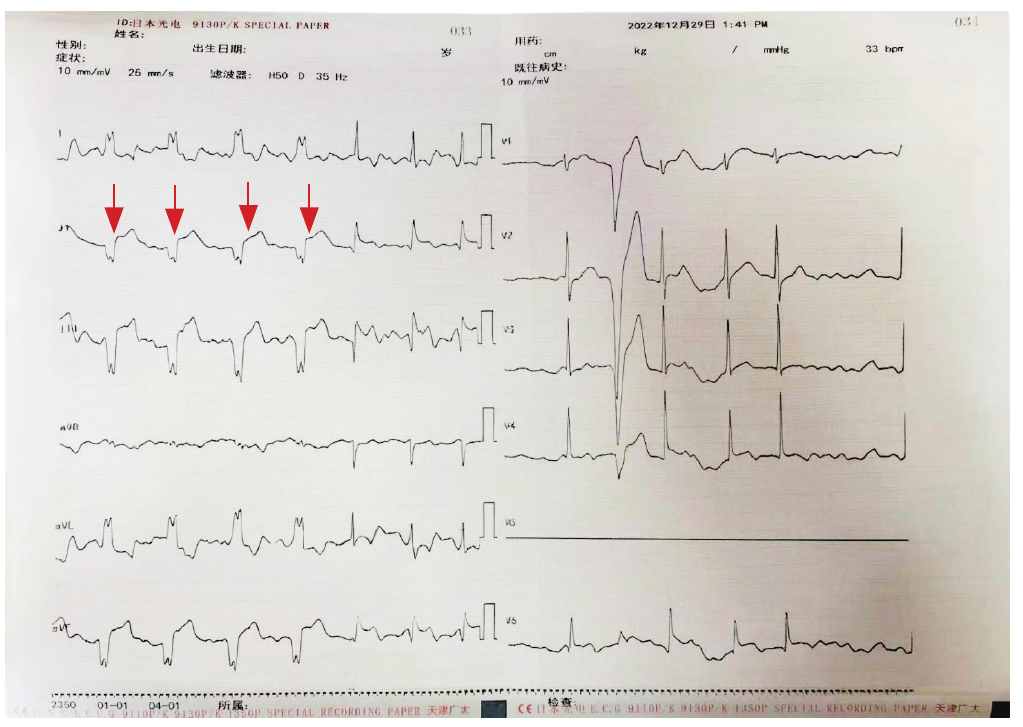
摘要: 背景 全科住院医师规范化培训(以下简称全科住培)分层递进式的培养目标要求全科住培第3年的住院医师(R3)具备独立接诊能力,带教老师就重点问题、疑难问题进行指导,从而提升其临床思维与全科诊疗能力。然而目前基层门诊教学内容、方法较单一,难以满足对危急重症如不典型急性冠脉综合征(ACS)的系统识别与处理能力的培养需求。 目的 探索在全科住培基层门诊教学中,采用PQRST疼痛评估法联合心血管风险评估,提升R3对不典型ACS的识别、诊断与处理能力,优化门诊教学质量。 方法 采用案例导向学习(CBL)法,以1名"饮酒后剑突下不适2小时"就诊患者为例,由R3独立接诊并书写病历,带教老师观察后补充并指出存在的问题,运用PQRST疼痛评估法系统采集症状信息,结合心血管风险评估工具进行风险分层,辅助心电图及心肌损伤标志物检查,明确ACS诊断,并实施院前急救与转诊。教学过程中采用思维导图记录与反馈,强化R3的临床推理与总结能力。 结果 通过PQRST疼痛评估法明确患者症状符合不典型胸痛特征,心血管风险评估属于"很高危"层次,心电图及心肌损伤标志物结果确诊为ST段抬高型心肌梗死(STEMI)。R3在带教老师指导下完成快速评估、院前处理及有序转诊。教学后R3对不典型ACS的识别能力、临床逻辑思维及急救转诊流程掌握程度显著提升。 结论 PQRST疼痛评估法联合心血管风险评估有助于提高R3对不典型ACS的早期识别与处理能力,结合思维导图进行反馈与总结,可有效构建系统鉴别诊断框架,适用于基层门诊教学中危急重症的案例教学,具有推广价值。
中图分类号: