中国全科医学 ›› 2026, Vol. 29 ›› Issue (15): 1992-1997.DOI: 10.12114/j.issn.1007-9572.2025.0120
熊晓曼, 李爱军, 郑月红, 杨秋雁, 张艳丽*( )
)
XIONG Xiaoman, LI Aijun, ZHENG Yuehong, YANG Qiuyan, ZHANG Yanli*()
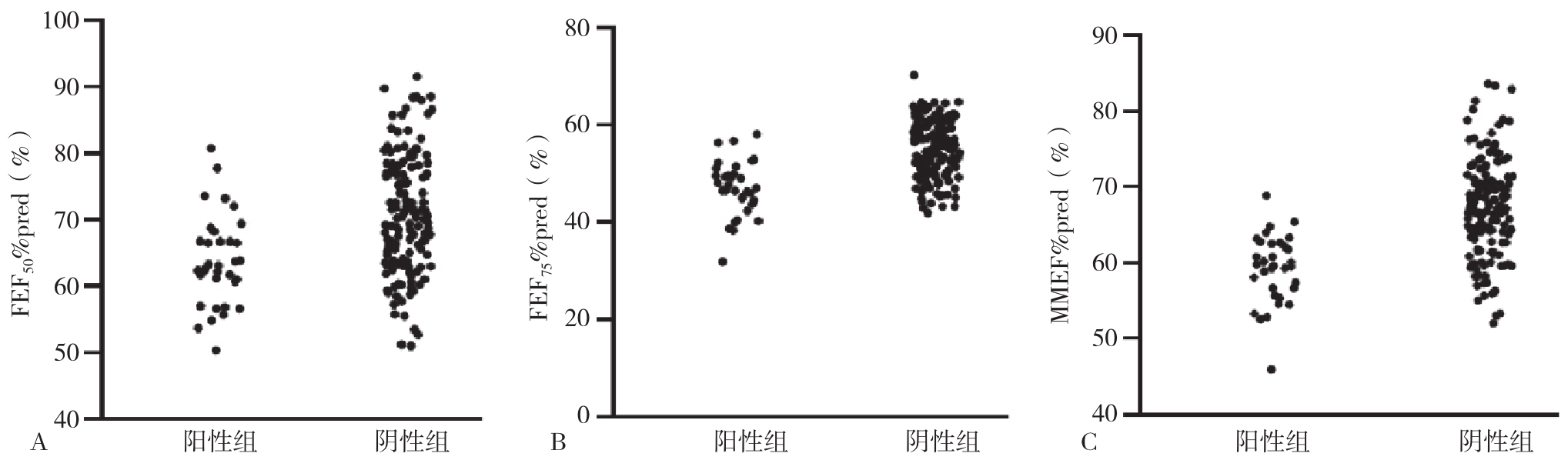
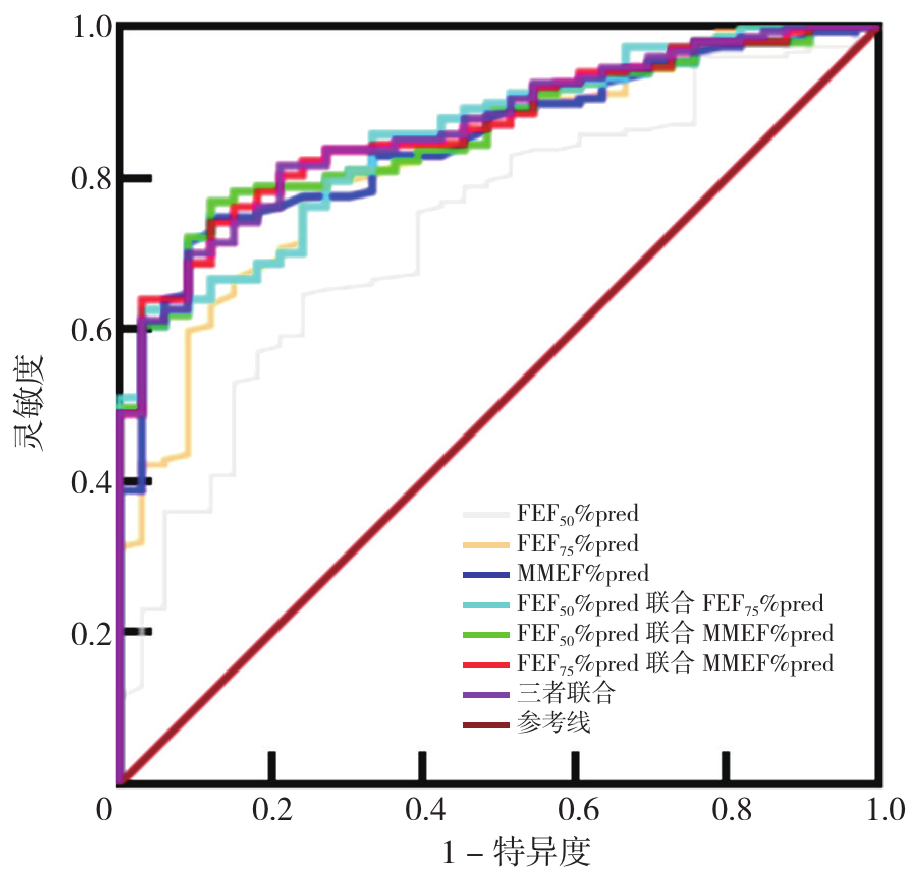
摘要: 背景 临床中对于有喘息、咳嗽、胸闷等哮喘相关症状患儿首先行肺通气功能检查,当第1秒用力呼气容积(FEV1)<70%提示存在明显的气流受限或呼吸道阻塞,应行支气管舒张试验,但部分患儿FEV1正常但小气道功能下降,提示可能存在轻度气流受限或呼吸道阻塞,且进行支气管激发试验较复杂、费用较高、具有一定的危险性、较多基层医院不具备开展的设备和人员条件,但这部分儿童进行支气管舒张试验也可以为阳性,对于哮喘诊断有一定意义。 目的 探讨FEV1、用力肺活量(FVC)及一秒率(FEV1/FVC)正常但小气道功能下降患儿行支气管舒张试验的必要性。 方法 选取2019-05-29—2024-09-20就诊于郑州大学第三附属医院门诊的180例5~14岁有喘息、咳嗽、胸闷等症状的哮喘患儿进行病例对照研究。研究对象已行常规肺通气功能检查及支气管舒张试验,且其常规肺通气功能检查结果显示FEV1、FVC及FEV1/FVC均正常、但小气道功能下降。以FEV1改善率≥12%作为支气管舒张试验阳性判断标准分为阳性组(n=33)及阴性组(n=147),比较两组基本资料及肺通气功能指标。采用Pearson相关性分析探讨小气道功能指标与支气管舒张试验结果的相关性。采用受试者工作特征(ROC)曲线分析小气道功能指标预测支气管舒张试验阳性结果的效能。 结果 支气管舒张试验阳性组患儿用力呼出50%肺活量时的瞬间流量占预测值百分比(FEF50%pred)、用力呼出75%肺活量时的瞬间流量占预测值百分比(FEF75%pred)及最大呼气中期流量占预测值百分比(MMEF%pred)均低于阴性组(P<0.05)。FEF50%pred、FEF75%pred、MMEF%pred与支气管舒张试验结果均具有相关性(P<0.001)。FEF50%pred、FEF75%pred、MMEF%pred预测支气管舒张试验阳性结果的曲线下面积(AUC)分别是0.733(95%CI=0.644~0.822)、0.827(95%CI=0.756~0.898)、0.849(95%CI=0.789~0.909),最佳截断值分别为66.85%、50.00%、63.35%;FEF50%pred联合FEF75%pred、FEF50%pred联合MMEF%pred、FEF75%pred联合MMEF%pred及三指标联合预测支气管舒张试验阳性结果的AUC分别为0.859、0.855、0.865、0.865;三指标联合预测支气管舒张试验阳性结果的AUC值大于FEF50%pred、FEF75%pred指标单独预测(Z=-2.801、-1.994,P=0.005、0.046)。 结论 对于存在喘息、胸闷、咳嗽等哮喘相关症状的患儿,即使FEV1、FVC及FEV1/FVC正常,仍需关注小气道功能指标,当FEF50%pred≤66.85%或FEF75%pred≤50.00%或MMEF%pred≤63.35%时可预测支气管舒张试验阳性结果,应积极行支气管舒张试验以辅助哮喘诊断。
中图分类号: