
中国全科医学 ›› 2025, Vol. 28 ›› Issue (36): 4566-4577.DOI: 10.12114/j.issn.1007-9572.2024.0521
所属专题: 心血管最新文章合辑
刘瑞越1,2, 杨雪梅3, 赵乃慧4, 温薪冉1,2, 蔡汐1,2, 梁雅靖1,2, 马佳佳1,2, 吴寿岭5, 崔刘福2,*( )
)
收稿日期:2024-11-04
修回日期:2025-06-30
出版日期:2025-12-20
发布日期:2025-12-04
通讯作者:
崔刘福
作者贡献:
刘瑞越负责论文起草,研究的实施,数据收集、采集、清洗和统计学分析、绘制图表;杨雪梅负责提出研究思路,设计研究方案,研究命题的提出、设计;赵乃慧、温薪冉、蔡汐、梁雅靖、马佳佳负责数据收集、采集、清洗;吴寿岭、崔刘福负责文章的质量控制与审查,对文章整体负责,监督管理。
LIU Ruiyue1,2, YANG Xuemei3, ZHAO Naihui4, WEN Xinran1,2, CAI Xi1,2, LIANG Yajing1,2, MA Jiajia1,2, WU Shouling5, CUI Liufu2,*()
Received:2024-11-04
Revised:2025-06-30
Published:2025-12-20
Online:2025-12-04
Contact:
CUI Liufu
摘要: 背景 心血管疾病(CVD)是最常见的慢性非传染性疾病,其患病率在全球范围内呈上升趋势,也是世界上人口死亡的主要原因。超敏C反应蛋白(hs-CRP)与白蛋白(ALB)比值(CAR)是一种新型的炎症指标,既往本研究团队对其与CVD的关联进行了研究,发现高CAR与CVD发病风险增加密切相关。且目前已有研究报道了从中年人群(51~64岁)到老年人群(≥65岁),高水平的hs-CRP所致的CVD发病风险逐渐降低。然而,CAR作为评估CVD风险的新型指标,其对新发CVD的影响在不同年龄段人群中是否存在差异尚不明确。 目的 探讨不同年龄段CAR对新发CVD的影响。 方法 纳入参加开滦队列研究2010年度第3次体检的54 951例参与者为研究对象,收集参与者人口学与临床数据、体检资料与实验室检查指标。计算CAR并进行对数转化(lgCAR),依据lgCAR四分位数将研究对象分为Q1组(lgCAR<-4.34,n=13 744)、Q2组(-4.34≤lgCAR<-3.67,n=13 731)、Q3组(-3.67≤lgCAR<-2.83,n=13 736)、Q4组(lgCAR≥-2.83,n=13 740),并按年龄进行分层,即<40岁(n=9 617)、40~49岁(n=12 633)、50~59岁(n=17 740)和≥60岁(n=14 691)。以完成2010年度体检的时间为随访起点,以发生CVD、全因死亡和到达随访结束日期为随访终点对患者进行随访,随访截至2021-12-31。采用Kaplan-Meier方法计算总人群和各年龄段人群CVD累积发病率,并采用Log-rank检验进行组间比较。采用Cox比例风险回归分析不同CAR水平总人群发生CVD的风险。通过Cox比例风险回归模型探究年龄与CAR各分位数组间的乘法交互作用,并按年龄进行分层重复上述分析。为了消除服用药物对结果产生的影响,排除基线和随访时服用降压、降糖、降脂药物的研究对象后进行敏感性分析;为了消除反向因果关系和随访时间过短对结果造成的影响,排除随访时间<1年的研究对象后进行敏感性分析;由于CVD的死亡风险较高,CVD和患者死亡之间可能存在相互竞争,因此对60岁以上的参与者采用死亡竞争风险模型分析不同CAR水平对CVD的影响。 结果 最终纳入54 951例研究对象,其中男41 083例(74.8%),女13 868例(25.2%),研究对象平均年龄(51.7±12.8)岁,Q1~Q4组平均lgCAR分别为-5.6±1.5、-4.0±0.2、-3.3±0.2、-2.2±0.6。Q1~Q4组年龄、性别、接受高等教育、吸烟、饮酒、体育锻炼、BMI、hs-CRP、低密度脂蛋白胆固醇、高密度脂蛋白胆固醇、总胆固醇、收缩压、舒张压、糖尿病、高血压、服用降压药、服用降糖药、服用降脂药、估算肾小球滤过率、丙氨酸氨基转移酶、ALB、lgCAR比较,差异有统计学意义(P<0.05)。平均随访(10.38±1.99)年,随访期间共3 444例(6.27%)研究对象发生了CVD,Q1~Q4组新发CVD病例分别为659、809、901、1 075例;累积发病率分别为4.79%、5.89%、6.56%、7.82%,Log-rank结果表明,总人群与不同年龄段Q1~Q4组研究对象CVD的累积发病率差异有统计学意义(P<0.05)。Cox比例风险回归模型分析结果表明,在校正混杂因素后,Q4组人群新发CVD的风险是Q1组的1.20倍(HR=1.20,95%CI=1.07~1.35),年龄和CAR组与CVD存在交互作用(P交互=0.021)。在<40岁、40~49岁、50~59岁和≥60岁人群中Q4组新发CVD的风险分别为Q1组的1.13倍(HR=1.13,95%CI=0.55~2.33)、1.44倍(HR=1.44,95%CI=1.06~1.96)、1.24倍(HR=1.24,95%CI=1.02~1.50)和1.11倍(HR=1.11,95%CI=0.93~1.33)。敏感性分析结果显示,在排除基线和随访期间服用降脂药的人群中,年龄和CAR组与CVD存在交互作用(P交互=0.020),在排除基线和随访期间服用降糖药的人群中,年龄和CAR组与CVD存在交互作用(P交互=0.015),在排除随访时间<1年的人群中,年龄和CAR组与CVD存在交互作用(P交互=0.045);Cox比例风险回归模型分析结果与主结果保持一致,CAR分组与新发CVD的关联在中年人群(40~59岁)中依然存在,并且随着年龄的增长,CAR升高所导致的CVD发病风险降低。排除在基线和随访期间服用降压药的人群后,年龄和CAR组与CVD之间的交互作用不显著(P交互=0.114);Cox比例风险回归模型分析发现,与主结果相比,在50~59岁人群中,CAR分组与新发CVD的统计学关联无意义(P>0.05)。对≥60岁研究对象采用死亡竞争风险模型分析不同CAR水平对CVD的影响,结果与主结果保持一致,CAR与新发心血管事件无关联。 结论 高CAR水平是新发CVD的独立危险因素,CAR与CVD发病风险的关联在中年人群呈年龄依赖性,而随着年龄增加,高CAR所致的CVD发病风险呈下降趋势。
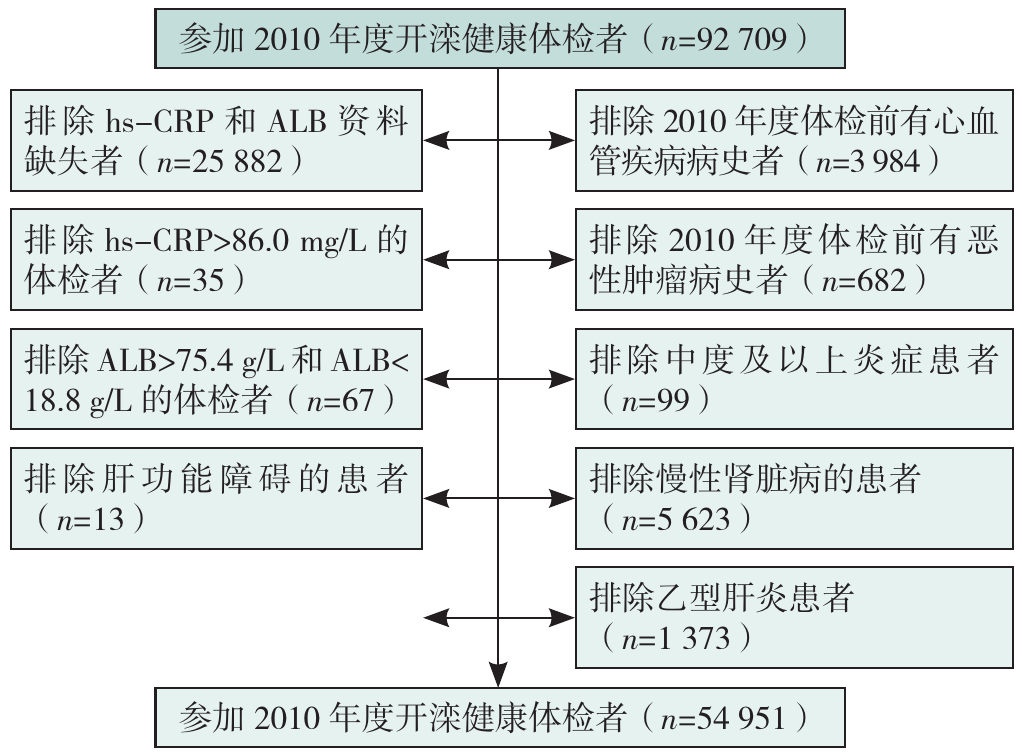
图1 研究对象纳入、排除流程图注:hs-CRP=超敏C反应,ALB=白蛋白。
Figure 1 The flow chart of the inclusion and exclusion
| 组别 | 例数 | 年龄(岁) | 性别(男/女) | 接受高等教育[例(%)] | 吸烟[例(%)] | 饮酒[例(%)] | 体育锻炼[例(%)] | BMI(kg/m2) | hs-CRP[M(P25,P75),mg/L] | LDL-C(mmol/L) | HDL-C(mmol/L) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1组 | 13 744 | 49.9±13.4 | 10 039/3 705 | 3 279(23.9) | 4 300(31.3) | 635(4.6) | 1 807(13.1) | 23.8±3.1 | 0.3(0.1,0.5) | 2.3±0.9 | 1.6±0.5 | ||
| Q2组 | 13 731 | 52.4±12.6 | 9 850/3 881 | 2 533(18.4) | 4 476(32.6) | 732(5.3) | 2 319(16.9) | 24.6±3.1 | 0.9(0.7,1.0) | 2.6±0.8 | 1.7±0.5 | ||
| Q3组 | 13 736 | 52.1±12.3 | 10 522/3 214 | 2 210(16.1) | 4 618(33.6) | 712(5.2) | 1 840(13.4) | 25.5±3.3 | 1.8(1.4,2.2) | 2.6±1.0 | 1.5±0.4 | ||
| Q4组 | 13 740 | 52.4±12.7 | 10 672/3 068 | 1 934(14.1) | 4 741(34.5) | 606(4.4) | 1 527(11.1) | 25.9±3.6 | 4.7(3.5,7.1) | 2.5±1.0 | 1.5±0.4 | ||
| 检验统计量值 | 125.58a | 174.45b | 495.66b | 35.72b | 17.24b | 201.06b | 1 155.63a | 51 340.37c | 237.46a | 630.80a | |||
| P值 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | |||
| 组别 | TC(mmol/L) | TG[M(P25,P75),mmol/L] | 收缩压(mmHg) | 舒张压(mmHg) | 糖尿病[例(%)] | 高血压[例(%)] | 服用降压药[例(%)] | 服用降糖药[例(%)] | 服用降脂药[例(%)] | eGFR[mL·min-1·(1.73 m2)-1] | ALT(U/L) | ALB(g/L) | lgCAR |
| Q1组 | 4.9±1.0 | 1.1(0.8,1.7) | 125±19 | 82±11 | 1 057(7.7) | 6 219(45.2) | 1 421(10.3) | 465(3.4) | 137(1.0) | 99.3±17.0 | 19.1±13.3 | 46.6±2.8 | -5.6±1.5 |
| Q2组 | 4.9±1.0 | 1.3(0.9,1.8) | 128±19 | 83±11 | 1 344(9.8) | 7 361(53.6) | 1 999(14.6) | 561(4.1) | 215(1.6) | 97.1±16.3 | 20.5±14.2 | 46.6±3.1 | -4.0±0.2 |
| Q3组 | 5.0±1.0 | 1.4(1.0,2.1) | 131±19 | 85±11 | 1 596(11.6) | 8 231(59.9) | 2 075(15.1) | 582(4.2) | 209(1.5) | 94.0±17.8 | 22.8±17.9 | 46.6±3.2 | -3.3±0.2 |
| Q4组 | 5.0±1.0 | 1.4(0.9,2.1) | 132±19 | 85±11 | 1 916(13.9) | 8 636(62.9) | 2 364(17.2) | 603(4.4) | 221(1.6) | 92.0±17.8 | 23.7±18.8 | 46.4±3.1 | -2.2±0.6 |
| 检验统计量值 | 66.70a | 1 266.77c | 331.12a | 295.96a | 304.03b | 1 013.67b | 278.58b | 21.09b | 24.11b | 487.64a | 237.17a | 12.50a | 44 981.90a |
| P值 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
表1 总人群中不同CAR分组的基线特征
Table 1 Baseline characteristics of different CAR groups in the total population
| 组别 | 例数 | 年龄(岁) | 性别(男/女) | 接受高等教育[例(%)] | 吸烟[例(%)] | 饮酒[例(%)] | 体育锻炼[例(%)] | BMI(kg/m2) | hs-CRP[M(P25,P75),mg/L] | LDL-C(mmol/L) | HDL-C(mmol/L) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1组 | 13 744 | 49.9±13.4 | 10 039/3 705 | 3 279(23.9) | 4 300(31.3) | 635(4.6) | 1 807(13.1) | 23.8±3.1 | 0.3(0.1,0.5) | 2.3±0.9 | 1.6±0.5 | ||
| Q2组 | 13 731 | 52.4±12.6 | 9 850/3 881 | 2 533(18.4) | 4 476(32.6) | 732(5.3) | 2 319(16.9) | 24.6±3.1 | 0.9(0.7,1.0) | 2.6±0.8 | 1.7±0.5 | ||
| Q3组 | 13 736 | 52.1±12.3 | 10 522/3 214 | 2 210(16.1) | 4 618(33.6) | 712(5.2) | 1 840(13.4) | 25.5±3.3 | 1.8(1.4,2.2) | 2.6±1.0 | 1.5±0.4 | ||
| Q4组 | 13 740 | 52.4±12.7 | 10 672/3 068 | 1 934(14.1) | 4 741(34.5) | 606(4.4) | 1 527(11.1) | 25.9±3.6 | 4.7(3.5,7.1) | 2.5±1.0 | 1.5±0.4 | ||
| 检验统计量值 | 125.58a | 174.45b | 495.66b | 35.72b | 17.24b | 201.06b | 1 155.63a | 51 340.37c | 237.46a | 630.80a | |||
| P值 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | |||
| 组别 | TC(mmol/L) | TG[M(P25,P75),mmol/L] | 收缩压(mmHg) | 舒张压(mmHg) | 糖尿病[例(%)] | 高血压[例(%)] | 服用降压药[例(%)] | 服用降糖药[例(%)] | 服用降脂药[例(%)] | eGFR[mL·min-1·(1.73 m2)-1] | ALT(U/L) | ALB(g/L) | lgCAR |
| Q1组 | 4.9±1.0 | 1.1(0.8,1.7) | 125±19 | 82±11 | 1 057(7.7) | 6 219(45.2) | 1 421(10.3) | 465(3.4) | 137(1.0) | 99.3±17.0 | 19.1±13.3 | 46.6±2.8 | -5.6±1.5 |
| Q2组 | 4.9±1.0 | 1.3(0.9,1.8) | 128±19 | 83±11 | 1 344(9.8) | 7 361(53.6) | 1 999(14.6) | 561(4.1) | 215(1.6) | 97.1±16.3 | 20.5±14.2 | 46.6±3.1 | -4.0±0.2 |
| Q3组 | 5.0±1.0 | 1.4(1.0,2.1) | 131±19 | 85±11 | 1 596(11.6) | 8 231(59.9) | 2 075(15.1) | 582(4.2) | 209(1.5) | 94.0±17.8 | 22.8±17.9 | 46.6±3.2 | -3.3±0.2 |
| Q4组 | 5.0±1.0 | 1.4(0.9,2.1) | 132±19 | 85±11 | 1 916(13.9) | 8 636(62.9) | 2 364(17.2) | 603(4.4) | 221(1.6) | 92.0±17.8 | 23.7±18.8 | 46.4±3.1 | -2.2±0.6 |
| 检验统计量值 | 66.70a | 1 266.77c | 331.12a | 295.96a | 304.03b | 1 013.67b | 278.58b | 21.09b | 24.11b | 487.64a | 237.17a | 12.50a | 44 981.90a |
| P值 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
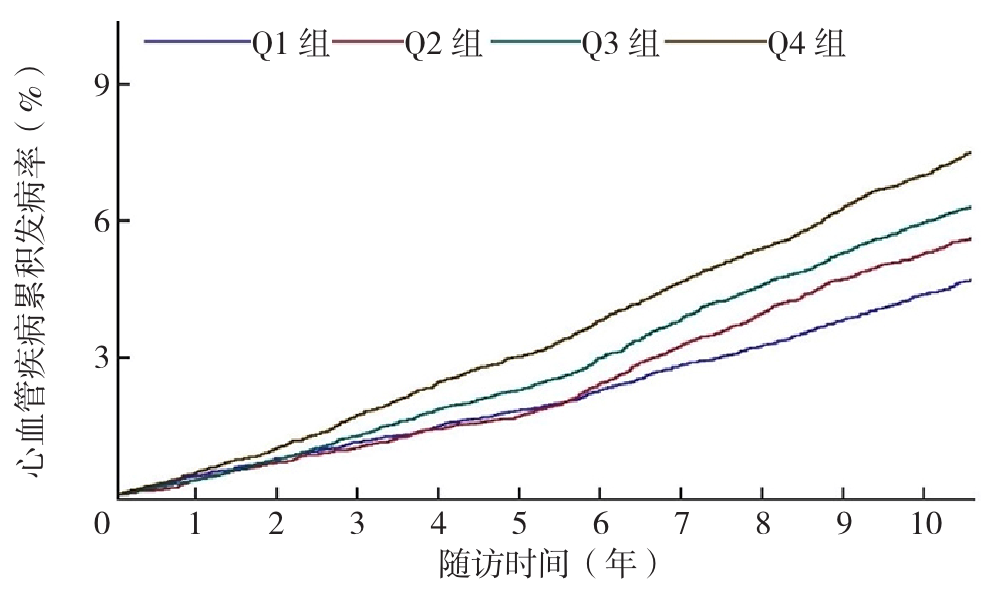
图2 不同CAR分组人群CVD累积发病率的Kaplan-Meier生存分析曲线
Figure 2 Kaplan-Meier survival analysis curves of cumulative incidence of CVD in different CAR groups
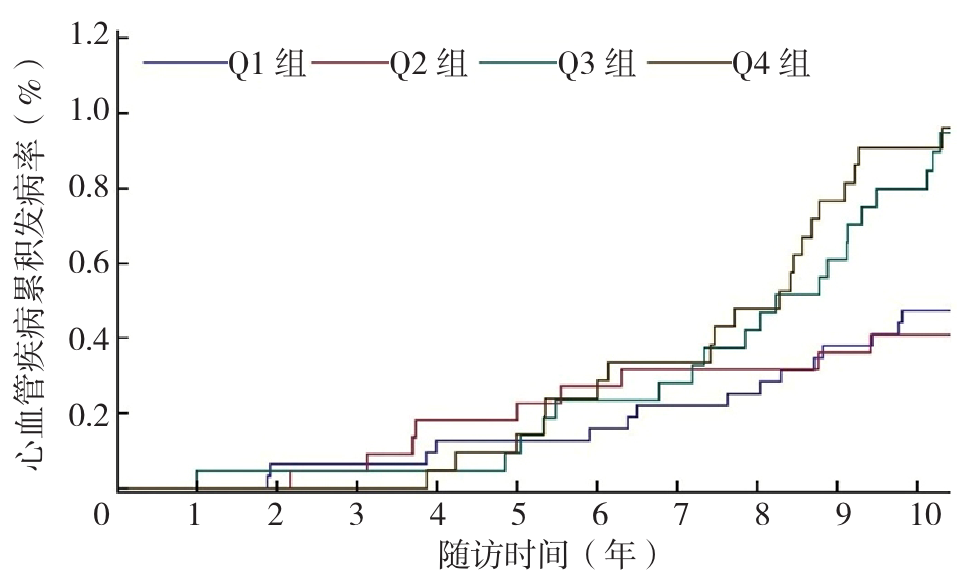
图3 <40岁人群不同CAR分组CVD累积发病率的Kaplan-Meier生存分析曲线
Figure 2 Kaplan-Meier survival analysis curves of cumulative incidence of CVD in different CAR groups in people under 40 years old
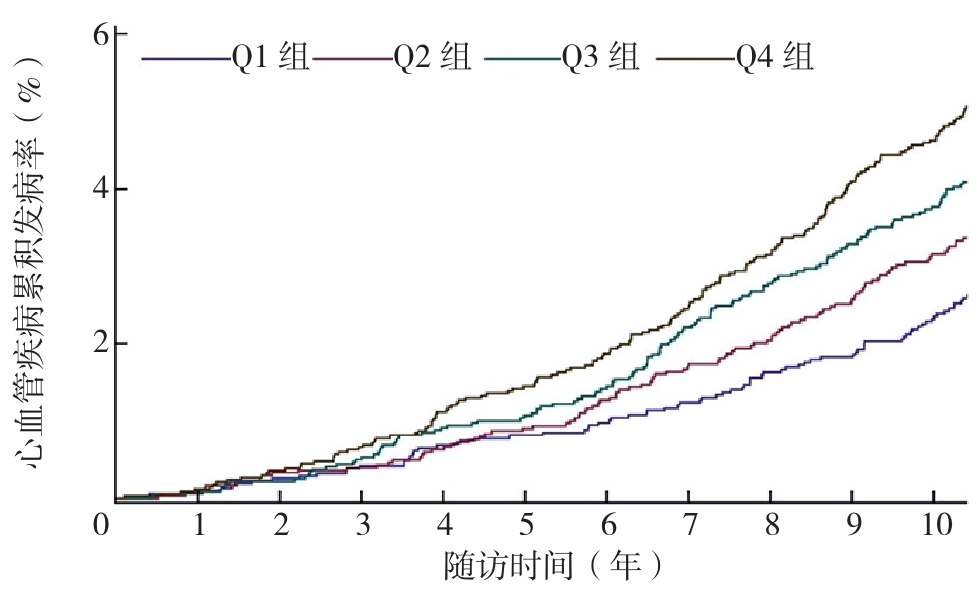
图4 40~49岁人群不同CAR分组CVD累积发病率的Kaplan-Meier生存分析曲线
Figure 4 Kaplan-Meier survival analysis curves of cumulative incidence of CVD in different CAR groups in people aged 40-49 years
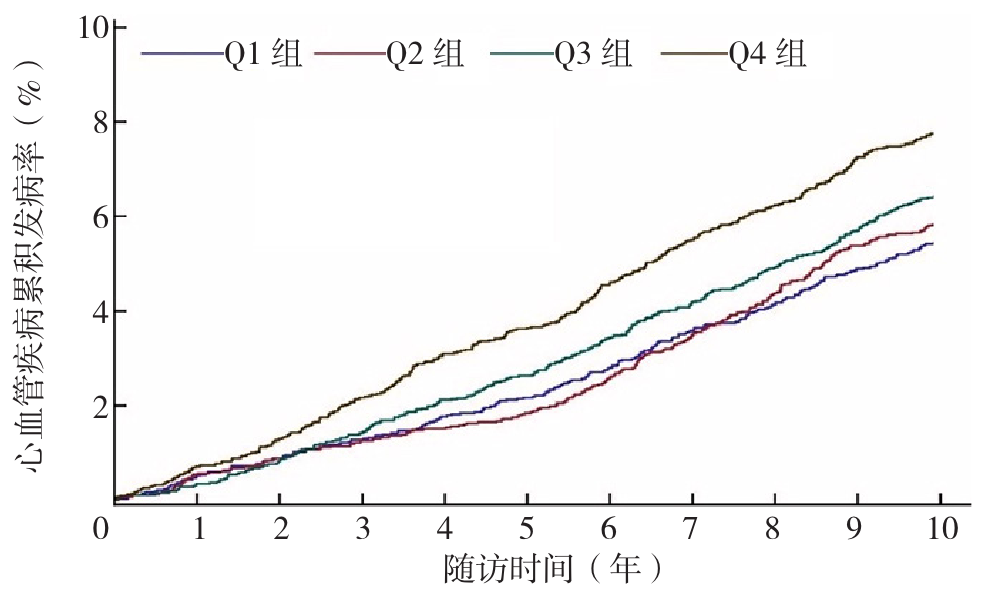
图5 50~59岁人群不同CAR分组CVD累积发病率的Kaplan-Meier生存分析曲线
Figure 5 Kaplan-Meier survival analysis curves of cumulative incidence of CVD in different CAR groups in people aged 50-59 years
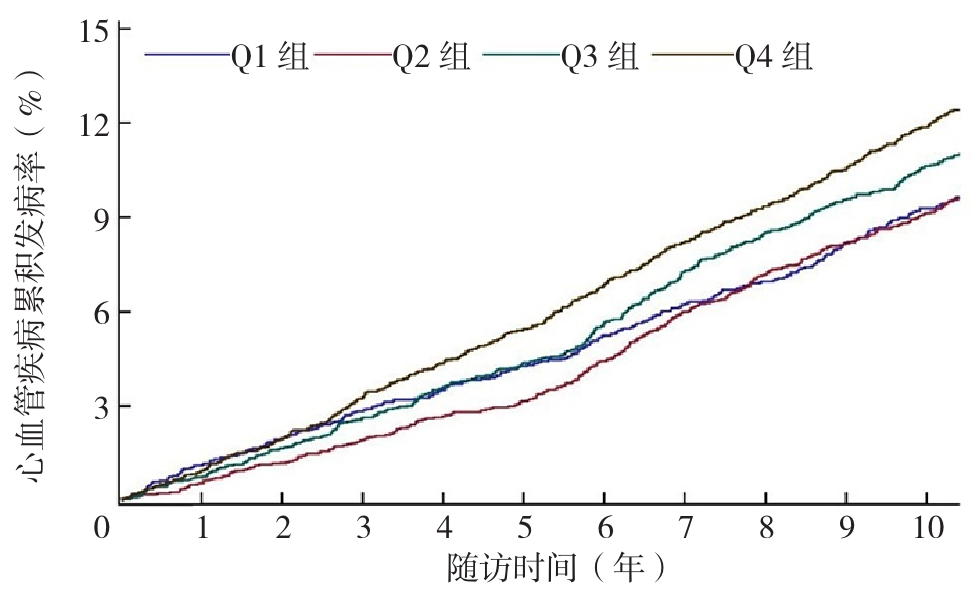
图6 ≥60岁人群不同CAR分组CVD累积发病率的Kaplan-Meier生存分析曲线
Figure 6 Kaplan-Meier survival analysis curves of cumulative incidence of CVD in people over 60 years old in different CAR groups
| 分组 | CVD发病人数(例) | 总人数(例) | 累积发病率(%) | 发病密度(例/千人年) |
|---|---|---|---|---|
| 总人群 | ||||
| Q1组 | 659 | 13 744 | 4.79 | 4.62 |
| Q2组 | 809 | 13 731 | 5.89 | 5.64 |
| Q3组 | 901 | 13 736 | 6.56 | 6.30 |
| Q4组 | 1 075 | 13 740 | 7.82 | 7.60 |
| <40岁 | ||||
| Q1组 | 17 | 3 168 | 0.54 | 0.50 |
| Q2组 | 10 | 2 212 | 0.45 | 0.41 |
| Q3组 | 25 | 2 143 | 1.17 | 1.06 |
| Q4组 | 29 | 2 094 | 1.38 | 1.25 |
| 40~49岁 | ||||
| Q1组 | 88 | 3 084 | 2.85 | 2.64 |
| Q2组 | 115 | 3 016 | 3.81 | 3.52 |
| Q3组 | 146 | 3 196 | 4.57 | 4.21 |
| Q4组 | 195 | 3 337 | 5.84 | 5.40 |
| 50~59岁 | ||||
| Q1组 | 261 | 4 326 | 6.03 | 5.81 |
| Q2组 | 280 | 4 324 | 6.48 | 6.15 |
| Q3组 | 329 | 4 666 | 7.05 | 6.72 |
| Q4组 | 392 | 4 424 | 8.86 | 8.55 |
| ≥60岁 | ||||
| Q1组 | 293 | 3 166 | 9.25 | 9.74 |
| Q2组 | 404 | 4 179 | 9.67 | 9.87 |
| Q3组 | 401 | 3 731 | 10.75 | 11.23 |
| Q4组 | 459 | 3 885 | 11.81 | 12.68 |
表2 Q1~Q4组各年龄分层CVD的发病情况
Table 2 Incidence of CVD in each age stratum of Q1-Q4 groups
| 分组 | CVD发病人数(例) | 总人数(例) | 累积发病率(%) | 发病密度(例/千人年) |
|---|---|---|---|---|
| 总人群 | ||||
| Q1组 | 659 | 13 744 | 4.79 | 4.62 |
| Q2组 | 809 | 13 731 | 5.89 | 5.64 |
| Q3组 | 901 | 13 736 | 6.56 | 6.30 |
| Q4组 | 1 075 | 13 740 | 7.82 | 7.60 |
| <40岁 | ||||
| Q1组 | 17 | 3 168 | 0.54 | 0.50 |
| Q2组 | 10 | 2 212 | 0.45 | 0.41 |
| Q3组 | 25 | 2 143 | 1.17 | 1.06 |
| Q4组 | 29 | 2 094 | 1.38 | 1.25 |
| 40~49岁 | ||||
| Q1组 | 88 | 3 084 | 2.85 | 2.64 |
| Q2组 | 115 | 3 016 | 3.81 | 3.52 |
| Q3组 | 146 | 3 196 | 4.57 | 4.21 |
| Q4组 | 195 | 3 337 | 5.84 | 5.40 |
| 50~59岁 | ||||
| Q1组 | 261 | 4 326 | 6.03 | 5.81 |
| Q2组 | 280 | 4 324 | 6.48 | 6.15 |
| Q3组 | 329 | 4 666 | 7.05 | 6.72 |
| Q4组 | 392 | 4 424 | 8.86 | 8.55 |
| ≥60岁 | ||||
| Q1组 | 293 | 3 166 | 9.25 | 9.74 |
| Q2组 | 404 | 4 179 | 9.67 | 9.87 |
| Q3组 | 401 | 3 731 | 10.75 | 11.23 |
| Q4组 | 459 | 3 885 | 11.81 | 12.68 |
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.11(1.00~1.23) | 0.04 | 1.05(0.94~1.16) | 0.38 | 1.04(0.94~1.15) | 0.45 | 1.04(0.93~1.15) | 0.51 |
| Q3组 | 1.26(1.14~1.39) | <0.01 | 1.11(1.00~1.23) | 0.03 | 1.11(1.00~1.23) | 0.04 | 1.10(0.99~1.22) | 0.07 |
| Q4组 | 1.49(1.35~1.64) | <0.01 | 1.27(1.15~1.40) | <0.01 | 1.26(1.15~1.40) | <0.01 | 1.20(1.07~1.35) | <0.01 |
| <40岁 | <0.01a | 0.08a | 0.06a | 0.35a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.64(0.28~1.43) | 0.27 | 0.57(0.25~1.28) | 0.17 | 0.56(0.25~1.26) | 0.16 | 0.55(0.24~1.23) | 0.14 |
| Q3组 | 1.65(0.89~3.07) | 0.11 | 1.31(0.70~2.46) | 0.39 | 1.36(0.72~2.55) | 0.33 | 1.28(0.68~2.42) | 0.44 |
| Q4组 | 1.92(1.05~3.51) | 0.03 | 1.44(0.77~2.69) | 0.25 | 1.47(0.79~2.75) | 0.22 | 1.13(0.55~2.33) | 0.74 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.03a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.29(0.98~1.70) | 0.07 | 1.21(0.92~1.60) | 0.17 | 1.21(0.92~1.60) | 0.17 | 1.21(0.91~1.60) | 0.18 |
| Q3组 | 1.42(1.09~1.85) | 0.01 | 1.22(0.93~1.59) | 0.14 | 1.23(0.94~1.61) | 0.12 | 1.22(0.93~1.60) | 0.14 |
| Q4组 | 1.76(1.36~2.26) | <0.01 | 1.45(1.12~1.87) | 0.01 | 1.47(1.14~1.91) | <0.01 | 1.44(1.06~1.96) | 0.02 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.13(0.95~1.33) | 0.16 | 1.06(0.90~1.26) | 0.48 | 1.06(0.90~1.26) | 0.49 | 1.06(0.90~1.26) | 0.49 |
| Q3组 | 1.17(0.99~1.38) | 0.05 | 1.04(0.88~1.22) | 0.67 | 1.03(0.88~1.22) | 0.68 | 1.03(0.87~1.22) | 0.72 |
| Q4组 | 1.48(1.27~1.73) | <0.01 | 1.27(1.08~1.49) | <0.01 | 1.26(1.08~1.48) | <0.01 | 1.24(1.02~1.50) | 0.03 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.13a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.03(0.89~1.20) | 0.70 | 0.99(0.85~1.15) | 0.91 | 0.98(0.85~1.14) | 0.82 | 0.98(0.84~1.13) | 0.73 |
| Q3组 | 1.19(1.02~1.38) | 0.02 | 1.11(0.95~1.29) | 0.18 | 1.10(0.95~1.28) | 0.20 | 1.08(0.93~1.26) | 0.33 |
| Q4组 | 1.33(1.15~1.54) | <0.01 | 1.21(1.05~1.41) | 0.01 | 1.20(1.03~1.39) | 0.01 | 1.11(0.93~1.33) | 0.24 |
表3 不同CAR分组总人群及不同年龄段人群CVD发生率的Cox比例风险回归模型分析结果
Table 3 Cox proportional hazards model analysis results of CVD incidence in the total population and different age groups in different CAR groups
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.11(1.00~1.23) | 0.04 | 1.05(0.94~1.16) | 0.38 | 1.04(0.94~1.15) | 0.45 | 1.04(0.93~1.15) | 0.51 |
| Q3组 | 1.26(1.14~1.39) | <0.01 | 1.11(1.00~1.23) | 0.03 | 1.11(1.00~1.23) | 0.04 | 1.10(0.99~1.22) | 0.07 |
| Q4组 | 1.49(1.35~1.64) | <0.01 | 1.27(1.15~1.40) | <0.01 | 1.26(1.15~1.40) | <0.01 | 1.20(1.07~1.35) | <0.01 |
| <40岁 | <0.01a | 0.08a | 0.06a | 0.35a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.64(0.28~1.43) | 0.27 | 0.57(0.25~1.28) | 0.17 | 0.56(0.25~1.26) | 0.16 | 0.55(0.24~1.23) | 0.14 |
| Q3组 | 1.65(0.89~3.07) | 0.11 | 1.31(0.70~2.46) | 0.39 | 1.36(0.72~2.55) | 0.33 | 1.28(0.68~2.42) | 0.44 |
| Q4组 | 1.92(1.05~3.51) | 0.03 | 1.44(0.77~2.69) | 0.25 | 1.47(0.79~2.75) | 0.22 | 1.13(0.55~2.33) | 0.74 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.03a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.29(0.98~1.70) | 0.07 | 1.21(0.92~1.60) | 0.17 | 1.21(0.92~1.60) | 0.17 | 1.21(0.91~1.60) | 0.18 |
| Q3组 | 1.42(1.09~1.85) | 0.01 | 1.22(0.93~1.59) | 0.14 | 1.23(0.94~1.61) | 0.12 | 1.22(0.93~1.60) | 0.14 |
| Q4组 | 1.76(1.36~2.26) | <0.01 | 1.45(1.12~1.87) | 0.01 | 1.47(1.14~1.91) | <0.01 | 1.44(1.06~1.96) | 0.02 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.13(0.95~1.33) | 0.16 | 1.06(0.90~1.26) | 0.48 | 1.06(0.90~1.26) | 0.49 | 1.06(0.90~1.26) | 0.49 |
| Q3组 | 1.17(0.99~1.38) | 0.05 | 1.04(0.88~1.22) | 0.67 | 1.03(0.88~1.22) | 0.68 | 1.03(0.87~1.22) | 0.72 |
| Q4组 | 1.48(1.27~1.73) | <0.01 | 1.27(1.08~1.49) | <0.01 | 1.26(1.08~1.48) | <0.01 | 1.24(1.02~1.50) | 0.03 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.13a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.03(0.89~1.20) | 0.70 | 0.99(0.85~1.15) | 0.91 | 0.98(0.85~1.14) | 0.82 | 0.98(0.84~1.13) | 0.73 |
| Q3组 | 1.19(1.02~1.38) | 0.02 | 1.11(0.95~1.29) | 0.18 | 1.10(0.95~1.28) | 0.20 | 1.08(0.93~1.26) | 0.33 |
| Q4组 | 1.33(1.15~1.54) | <0.01 | 1.21(1.05~1.41) | 0.01 | 1.20(1.03~1.39) | 0.01 | 1.11(0.93~1.33) | 0.24 |
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.07(0.95~1.22) | 0.26 | 1.02(0.90~1.16) | 0.70 | 1.02(0.90~1.16) | 0.74 | 1.02(0.90~1.15) | 0.80 |
| Q3组 | 1.26(1.12~1.42) | <0.01 | 1.12(0.99~1.27) | 0.06 | 1.12(0.99~1.26) | 0.07 | 1.10(0.97~1.25) | 0.12 |
| Q4组 | 1.47(1.30~1.65) | <0.01 | 1.28(1.13~1.44) | <0.01 | 1.27(1.13~1.43) | <0.01 | 1.21(1.04~1.39) | 0.01 |
| <40岁 | 0.26a | 0.80a | 0.79a | 0.96a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.58(0.24~1.42) | 0.23 | 0.52(0.21~1.28) | 0.15 | 0.52(0.21~1.27) | 0.15 | 0.50(0.20~1.24) | 0.13 |
| Q3组 | 1.57(0.80~3.08) | 0.18 | 1.22(0.61~2.43) | 0.57 | 1.24(0.62~2.46) | 0.54 | 1.15(0.58~2.31) | 0.68 |
| Q4组 | 1.17(0.57~2.40) | 0.66 | 0.88(0.42~1.87) | 0.74 | 0.88(0.42~1.86) | 0.73 | 0.65(0.27~2.57) | 0.33 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.35(0.96~1.90) | 0.08 | 1.29(0.91~1.81) | 0.15 | 1.27(0.90~1.79) | 0.16 | 1.26(0.89~1.78) | 0.18 |
| Q3组 | 1.49(1.07~2.07) | 0.01 | 1.33(0.95~1.85) | 0.09 | 1.32(0.95~1.84) | 0.10 | 1.30(0.93~1.81) | 0.12 |
| Q4组 | 2.01(1.47~2.73) | <0.01 | 1.73(1.26~2.37) | <0.01 | 1.73(1.26~2.37) | <0.01 | 1.62(1.12~2.34) | 0.01 |
| 50~59岁 | <0.01a | 0.05a | 0.07a | 0.22a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.00(0.82~1.23) | 0.96 | 0.96(0.78~1.18) | 0.71 | 0.96(0.78~1.18) | 0.69 | 0.97(0.79~1.19) | 0.75 |
| Q3组 | 1.05(0.86~1.27) | 0.65 | 0.94(0.77~1.14) | 0.51 | 0.93(0.76~1.14) | 0.48 | 0.94(0.77~1.15) | 0.53 |
| Q4组 | 1.39(1.15~1.68) | <0.01 | 1.22(1.00~1.47) | 0.04 | 1.21(0.99~1.46) | 0.05 | 1.23(0.97~1.57) | 0.08 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.13a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.05(0.87~1.25) | 0.63 | 1.01(0.84~1.21) | 0.92 | 1.00(0.84~1.20) | 0.97 | 0.99(0.83~1.19) | 0.95 |
| Q3组 | 1.29(1.08~1.54) | 0.01 | 1.19(0.99~1.43) | 0.06 | 1.18(0.99~1.42) | 0.06 | 1.16(0.96~1.39) | 0.11 |
| Q4组 | 1.34(1.12~1.60) | <0.01 | 1.22(0.02~1.47) | 0.02 | 1.21(1.01~1.46) | 0.03 | 1.12(0.90~1.39) | 0.31 |
表4 排除服用降压药研究对象后不同CAR分组总人群及不同年龄段人群CVD发生率的Cox比例风险回归模型分析结果
Table 4 Results of Cox proportional hazards model analysis on the incidence of cvd in different car groups and different age groups after excluding study subjects taking antihypertensive medications
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.07(0.95~1.22) | 0.26 | 1.02(0.90~1.16) | 0.70 | 1.02(0.90~1.16) | 0.74 | 1.02(0.90~1.15) | 0.80 |
| Q3组 | 1.26(1.12~1.42) | <0.01 | 1.12(0.99~1.27) | 0.06 | 1.12(0.99~1.26) | 0.07 | 1.10(0.97~1.25) | 0.12 |
| Q4组 | 1.47(1.30~1.65) | <0.01 | 1.28(1.13~1.44) | <0.01 | 1.27(1.13~1.43) | <0.01 | 1.21(1.04~1.39) | 0.01 |
| <40岁 | 0.26a | 0.80a | 0.79a | 0.96a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.58(0.24~1.42) | 0.23 | 0.52(0.21~1.28) | 0.15 | 0.52(0.21~1.27) | 0.15 | 0.50(0.20~1.24) | 0.13 |
| Q3组 | 1.57(0.80~3.08) | 0.18 | 1.22(0.61~2.43) | 0.57 | 1.24(0.62~2.46) | 0.54 | 1.15(0.58~2.31) | 0.68 |
| Q4组 | 1.17(0.57~2.40) | 0.66 | 0.88(0.42~1.87) | 0.74 | 0.88(0.42~1.86) | 0.73 | 0.65(0.27~2.57) | 0.33 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.35(0.96~1.90) | 0.08 | 1.29(0.91~1.81) | 0.15 | 1.27(0.90~1.79) | 0.16 | 1.26(0.89~1.78) | 0.18 |
| Q3组 | 1.49(1.07~2.07) | 0.01 | 1.33(0.95~1.85) | 0.09 | 1.32(0.95~1.84) | 0.10 | 1.30(0.93~1.81) | 0.12 |
| Q4组 | 2.01(1.47~2.73) | <0.01 | 1.73(1.26~2.37) | <0.01 | 1.73(1.26~2.37) | <0.01 | 1.62(1.12~2.34) | 0.01 |
| 50~59岁 | <0.01a | 0.05a | 0.07a | 0.22a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.00(0.82~1.23) | 0.96 | 0.96(0.78~1.18) | 0.71 | 0.96(0.78~1.18) | 0.69 | 0.97(0.79~1.19) | 0.75 |
| Q3组 | 1.05(0.86~1.27) | 0.65 | 0.94(0.77~1.14) | 0.51 | 0.93(0.76~1.14) | 0.48 | 0.94(0.77~1.15) | 0.53 |
| Q4组 | 1.39(1.15~1.68) | <0.01 | 1.22(1.00~1.47) | 0.04 | 1.21(0.99~1.46) | 0.05 | 1.23(0.97~1.57) | 0.08 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.13a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.05(0.87~1.25) | 0.63 | 1.01(0.84~1.21) | 0.92 | 1.00(0.84~1.20) | 0.97 | 0.99(0.83~1.19) | 0.95 |
| Q3组 | 1.29(1.08~1.54) | 0.01 | 1.19(0.99~1.43) | 0.06 | 1.18(0.99~1.42) | 0.06 | 1.16(0.96~1.39) | 0.11 |
| Q4组 | 1.34(1.12~1.60) | <0.01 | 1.22(0.02~1.47) | 0.02 | 1.21(1.01~1.46) | 0.03 | 1.12(0.90~1.39) | 0.31 |
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.09(0.99~1.22) | 0.09 | 1.03(0.93~1.14) | 0.58 | 1.02(0.92~1.14) | 0.67 | 1.02(0.92~1.13) | 0.74 |
| Q3组 | 1.25(1.13~1.39) | <0.01 | 1.10(1.00~1.22) | 0.06 | 1.10(0.99~1.22) | 0.06 | 1.09(0.98~1.21) | 0.12 |
| Q4组 | 1.48(1.34~1.63) | <0.01 | 1.27(1.15~1.40) | <0.01 | 1.26(1.14~1.39) | <0.01 | 1.19(1.06~1.34) | <0.01 |
| <40岁 | <0.01a | 0.09a | 0.07a | 0.40a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.57(0.25~1.32) | 0.18 | 0.51(0.22~1.17) | 0.11 | 0.50(0.21~1.15) | 0.10 | 0.48(0.21~1.12) | 0.09 |
| Q3组 | 1.60(0.86~2.98) | 0.14 | 1.26(0.67~2.38) | 0.47 | 1.30(0.69~2.46) | 0.41 | 1.22(0.65~2.32) | 0.53 |
| Q4组 | 1.87(1.02~3.43) | 0.04 | 1.39(0.74~2.61) | 0.30 | 1.42(0.75~2.66) | 0.28 | 1.08(0.52~2.24) | 0.83 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.34(1.01~1.78) | 0.04 | 1.26(0.95~1.68) | 0.10 | 1.26(0.95~1.67) | 0.11 | 1.25(0.94~1.66) | 0.12 |
| Q3组 | 1.45(1.11~1.91) | 0.01 | 1.25(0.95~1.65) | 0.11 | 1.26(0.96~1.66) | 0.10 | 1.24(0.94~1.64) | 0.12 |
| Q4组 | 1.77(1.36~2.30) | <0.01 | 1.47(1.12~1.91) | 0.01 | 1.49(1.14~1.95) | <0.01 | 1.43(1.04~1.96) | 0.02 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.12(0.94~1.33) | 0.21 | 1.05(0.89~1.25) | 0.55 | 1.05(0.89~1.25) | 0.55 | 1.05(0.89~1.25) | 0.55 |
| Q3组 | 1.18(0.99~1.39) | 0.05 | 1.04(0.88~1.23) | 0.63 | 1.04(0.88~1.23) | 0.63 | 1.04(0.88~1.23) | 0.64 |
| Q4组 | 1.49(1.27~1.74) | <0.01 | 1.27(1.08~1.50) | <0.01 | 1.27(1.08~1.49) | <0.01 | 1.26(1.03~1.53) | 0.02 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.19a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.00(0.86~1.16) | 0.97 | 0.96(0.82~1.12) | 0.57 | 0.95(0.81~1.11) | 0.49 | 0.94(0.81~1.10) | 0.42 |
| Q3组 | 1.16(0.99~1.35) | 0.06 | 1.07(0.92~1.25) | 0.36 | 1.07(0.92~1.25) | 0.36 | 1.04(0.89~1.22) | 0.58 |
| Q4组 | 1.32(1.14~1.53) | <0.01 | 1.20(1.03~1.40) | 0.01 | 1.19(1.02~1.38) | 0.02 | 1.09(0.91~1.30) | 0.35 |
表5 排除服用降脂药研究对象后不同CAR分组总人群及不同年龄段人群CVD发生率的Cox比例风险回归模型分析结果
Table 5 Results of Cox proportional hazards model analysis on the incidence of cvd in different car groups and different age groups after excluding study subjects taking lipid-lowering medications
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.09(0.99~1.22) | 0.09 | 1.03(0.93~1.14) | 0.58 | 1.02(0.92~1.14) | 0.67 | 1.02(0.92~1.13) | 0.74 |
| Q3组 | 1.25(1.13~1.39) | <0.01 | 1.10(1.00~1.22) | 0.06 | 1.10(0.99~1.22) | 0.06 | 1.09(0.98~1.21) | 0.12 |
| Q4组 | 1.48(1.34~1.63) | <0.01 | 1.27(1.15~1.40) | <0.01 | 1.26(1.14~1.39) | <0.01 | 1.19(1.06~1.34) | <0.01 |
| <40岁 | <0.01a | 0.09a | 0.07a | 0.40a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.57(0.25~1.32) | 0.18 | 0.51(0.22~1.17) | 0.11 | 0.50(0.21~1.15) | 0.10 | 0.48(0.21~1.12) | 0.09 |
| Q3组 | 1.60(0.86~2.98) | 0.14 | 1.26(0.67~2.38) | 0.47 | 1.30(0.69~2.46) | 0.41 | 1.22(0.65~2.32) | 0.53 |
| Q4组 | 1.87(1.02~3.43) | 0.04 | 1.39(0.74~2.61) | 0.30 | 1.42(0.75~2.66) | 0.28 | 1.08(0.52~2.24) | 0.83 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.34(1.01~1.78) | 0.04 | 1.26(0.95~1.68) | 0.10 | 1.26(0.95~1.67) | 0.11 | 1.25(0.94~1.66) | 0.12 |
| Q3组 | 1.45(1.11~1.91) | 0.01 | 1.25(0.95~1.65) | 0.11 | 1.26(0.96~1.66) | 0.10 | 1.24(0.94~1.64) | 0.12 |
| Q4组 | 1.77(1.36~2.30) | <0.01 | 1.47(1.12~1.91) | 0.01 | 1.49(1.14~1.95) | <0.01 | 1.43(1.04~1.96) | 0.02 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.12(0.94~1.33) | 0.21 | 1.05(0.89~1.25) | 0.55 | 1.05(0.89~1.25) | 0.55 | 1.05(0.89~1.25) | 0.55 |
| Q3组 | 1.18(0.99~1.39) | 0.05 | 1.04(0.88~1.23) | 0.63 | 1.04(0.88~1.23) | 0.63 | 1.04(0.88~1.23) | 0.64 |
| Q4组 | 1.49(1.27~1.74) | <0.01 | 1.27(1.08~1.50) | <0.01 | 1.27(1.08~1.49) | <0.01 | 1.26(1.03~1.53) | 0.02 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.19a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.00(0.86~1.16) | 0.97 | 0.96(0.82~1.12) | 0.57 | 0.95(0.81~1.11) | 0.49 | 0.94(0.81~1.10) | 0.42 |
| Q3组 | 1.16(0.99~1.35) | 0.06 | 1.07(0.92~1.25) | 0.36 | 1.07(0.92~1.25) | 0.36 | 1.04(0.89~1.22) | 0.58 |
| Q4组 | 1.32(1.14~1.53) | <0.01 | 1.20(1.03~1.40) | 0.01 | 1.19(1.02~1.38) | 0.02 | 1.09(0.91~1.30) | 0.35 |
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.13(1.01~1.26) | 0.02 | 1.07(0.96~1.20) | 0.22 | 1.06(0.95~1.19) | 0.28 | 1.06(0.95~1.18) | 0.33 |
| Q3组 | 1.26(1.13~1.40) | <0.01 | 1.12(1.00~1.25) | 0.04 | 1.11(0.99~1.24) | 0.05 | 1.10(0.98~1.22) | 0.10 |
| Q4组 | 1.51(1.36~1.67) | <0.01 | 1.31(1.18~1.46) | <0.01 | 1.30(1.17~1.44) | <0.01 | 1.21(1.07~1.38) | <0.01 |
| <40岁 | 0.01a | 0.15a | 0.12a | 0.48a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.65(0.29~1.45) | 0.28 | 0.57(0.26~1.29) | 0.17 | 0.57(0.25~1.28) | 0.17 | 0.56(0.25~1.25) | 0.15 |
| Q3组 | 1.61(0.86~3.00) | 0.13 | 1.28(0.68~2.41) | 0.44 | 1.33(0.71~2.51) | 0.38 | 1.25(0.66~2.37) | 0.49 |
| Q4组 | 1.77(0.96~3.27) | 0.06 | 1.33(0.70~2.51) | 0.38 | 1.35(0.71~2.56) | 0.35 | 1.05(0.50~2.21) | 0.90 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.39(1.04~1.86) | 0.02 | 1.31(0.98~1.76) | 0.06 | 1.31(0.98~1.75) | 0.07 | 1.30(0.97~1.74) | 0.08 |
| Q3组 | 1.42(1.07~1.89) | 0.01 | 1.23(0.93~1.64) | 0.15 | 1.24(0.94~1.65) | 0.13 | 1.23(0.92~1.63) | 0.16 |
| Q4组 | 1.82(1.39~2.38) | <0.01 | 1.53(1.16~2.01) | <0.01 | 1.55(1.18~2.03) | <0.01 | 1.47(1.07~2.04) | 0.01 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.10(0.91~1.31) | 0.32 | 1.05(0.87~1.26) | 0.61 | 1.04(0.87~1.25) | 0.65 | 1.04(0.87~1.25) | 0.66 |
| Q3组 | 1.18(0.99~1.40) | 0.06 | 1.06(0.89~1.26) | 0.52 | 1.05(0.89~1.26) | 0.55 | 1.05(0.88~1.25) | 0.58 |
| Q4组 | 1.50(1.27~1.77) | <0.01 | 1.32(1.11~1.56) | <0.01 | 1.30(1.10~1.55) | <0.01 | 1.28(1.04~1.58) | 0.01 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.24a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.06(0.91~1.25) | 0.45 | 1.03(0.87~1.21) | 0.76 | 1.02(0.87~1.20) | 0.84 | 1.01(0.85~1.18) | 0.95 |
| Q3组 | 1.18(1.00~1.39) | 0.04 | 1.10(0.93~1.29) | 0.27 | 1.09(0.93~1.29) | 0.29 | 1.06(0.90~1.25) | 0.48 |
| Q4组 | 1.35(1.16~1.58) | <0.01 | 1.24(1.06~1.46) | 0.01 | 1.23(1.05~1.44) | 0.01 | 1.10(0.91~1.33) | 0.30 |
表6 排除服用降糖药研究对象后不同CAR分组总人群及不同年龄段人群CVD发生率的Cox比例风险回归模型分析结果
Table 6 Results of Cox proportional hazards model analysis on the incidence of cvd in different car groups and different age groups after excluding study subjects taking antidiabetic medications
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.13(1.01~1.26) | 0.02 | 1.07(0.96~1.20) | 0.22 | 1.06(0.95~1.19) | 0.28 | 1.06(0.95~1.18) | 0.33 |
| Q3组 | 1.26(1.13~1.40) | <0.01 | 1.12(1.00~1.25) | 0.04 | 1.11(0.99~1.24) | 0.05 | 1.10(0.98~1.22) | 0.10 |
| Q4组 | 1.51(1.36~1.67) | <0.01 | 1.31(1.18~1.46) | <0.01 | 1.30(1.17~1.44) | <0.01 | 1.21(1.07~1.38) | <0.01 |
| <40岁 | 0.01a | 0.15a | 0.12a | 0.48a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.65(0.29~1.45) | 0.28 | 0.57(0.26~1.29) | 0.17 | 0.57(0.25~1.28) | 0.17 | 0.56(0.25~1.25) | 0.15 |
| Q3组 | 1.61(0.86~3.00) | 0.13 | 1.28(0.68~2.41) | 0.44 | 1.33(0.71~2.51) | 0.38 | 1.25(0.66~2.37) | 0.49 |
| Q4组 | 1.77(0.96~3.27) | 0.06 | 1.33(0.70~2.51) | 0.38 | 1.35(0.71~2.56) | 0.35 | 1.05(0.50~2.21) | 0.90 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.39(1.04~1.86) | 0.02 | 1.31(0.98~1.76) | 0.06 | 1.31(0.98~1.75) | 0.07 | 1.30(0.97~1.74) | 0.08 |
| Q3组 | 1.42(1.07~1.89) | 0.01 | 1.23(0.93~1.64) | 0.15 | 1.24(0.94~1.65) | 0.13 | 1.23(0.92~1.63) | 0.16 |
| Q4组 | 1.82(1.39~2.38) | <0.01 | 1.53(1.16~2.01) | <0.01 | 1.55(1.18~2.03) | <0.01 | 1.47(1.07~2.04) | 0.01 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.10(0.91~1.31) | 0.32 | 1.05(0.87~1.26) | 0.61 | 1.04(0.87~1.25) | 0.65 | 1.04(0.87~1.25) | 0.66 |
| Q3组 | 1.18(0.99~1.40) | 0.06 | 1.06(0.89~1.26) | 0.52 | 1.05(0.89~1.26) | 0.55 | 1.05(0.88~1.25) | 0.58 |
| Q4组 | 1.50(1.27~1.77) | <0.01 | 1.32(1.11~1.56) | <0.01 | 1.30(1.10~1.55) | <0.01 | 1.28(1.04~1.58) | 0.01 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.24a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.06(0.91~1.25) | 0.45 | 1.03(0.87~1.21) | 0.76 | 1.02(0.87~1.20) | 0.84 | 1.01(0.85~1.18) | 0.95 |
| Q3组 | 1.18(1.00~1.39) | 0.04 | 1.10(0.93~1.29) | 0.27 | 1.09(0.93~1.29) | 0.29 | 1.06(0.90~1.25) | 0.48 |
| Q4组 | 1.35(1.16~1.58) | <0.01 | 1.24(1.06~1.46) | 0.01 | 1.23(1.05~1.44) | 0.01 | 1.10(0.91~1.33) | 0.30 |
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.15(1.03~1.28) | 0.01 | 1.08(0.97~1.20) | 0.15 | 1.08(0.97~1.20) | 0.18 | 1.07(0.96~1.19) | 0.21 |
| Q3组 | 1.31(1.18~1.46) | <0.01 | 1.16(1.04~1.29) | 0.01 | 1.16(1.04~1.28) | 0.01 | 1.14(1.03~1.27) | 0.01 |
| Q4组 | 1.53(1.38~1.69) | <0.01 | 1.30(1.18~1.45) | <0.01 | 1.30(1.17~1.44) | <0.01 | 1.24(1.09~1.40) | <0.01 |
| <40岁 | <0.01a | 0.07a | 0.06a | 0.35a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.64(0.28~1.43) | 0.27 | 0.57(0.26~1.28) | 0.17 | 0.56(0.25~1.26) | 0.15 | 0.55(0.24~1.23) | 0.14 |
| Q3组 | 1.59(0.85~2.96) | 0.14 | 1.27(0.67~2.39) | 0.46 | 1.31(0.70~2.48) | 0.39 | 1.24(0.66~2.35) | 0.50 |
| Q4组 | 1.92(1.05~3.50) | 0.03 | 1.46(0.78~2.72) | 0.23 | 1.49(0.80~2.79) | 0.21 | 1.15(0.56~2.36) | 0.71 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.03a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.29(0.98~1.71) | 0.07 | 1.22(0.92~1.61) | 0.16 | 1.22(0.92~1.61) | 0.17 | 1.21(0.91~1.60) | 0.18 |
| Q3组 | 1.42(1.09~1.86) | 0.01 | 1.22(0.93~1.60) | 0.14 | 1.23(0.94~1.62) | 0.13 | 1.22(0.93~1.61) | 0.15 |
| Q4组 | 1.76(1.36~2.27) | <0.01 | 1.45(1.11~1.88) | 0.01 | 1.47(1.13~1.91) | <0.01 | 1.43(1.05~1.95) | 0.02 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.13(0.95~1.35) | 0.16 | 1.07(0.90~1.28) | 0.46 | 1.07(0.89~1.27) | 0.47 | 1.07(0.89~1.27) | 0.48 |
| Q3组 | 1.22(1.03~1.44) | 0.02 | 1.08(0.91~1.28) | 0.38 | 1.08(0.91~1.28) | 0.39 | 1.07(0.90~1.27) | 0.46 |
| Q4组 | 1.49(1.27~1.76) | <0.01 | 1.28(1.08~1.51) | <0.01 | 1.27(1.08~1.50) | <0.01 | 1.22(1.01~1.49) | 0.04 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.03a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.10(0.94~1.29) | 0.24 | 1.06(0.90~1.24) | 0.48 | 1.05(0.90~1.23) | 0.54 | 1.04(0.89~1.22) | 0.59 |
| Q3组 | 1.25(1.07~1.47) | 0.00 | 1.17(0.99~1.37) | 0.05 | 1.17(0.99~1.37) | 0.06 | 1.15(0.98~1.35) | 0.09 |
| Q4组 | 1.39(1.19~1.62) | <0.01 | 1.27(1.09~1.49) | <0.01 | 1.26(1.07~1.47) | <0.01 | 1.20(0.99~1.44) | 0.05 |
表7 排除随访时间<1年研究对象后不同CAR分组总人群及不同年龄段人群CVD发生率的Cox比例风险回归模型分析结果
Table 7 Results of Cox proportional hazards model analysis on the incidence of cvd in different car groups and different age groups after excluding study subjects with follow-up time <1 year
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| 总人群 | <0.01a | <0.01a | <0.01a | <0.01a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.15(1.03~1.28) | 0.01 | 1.08(0.97~1.20) | 0.15 | 1.08(0.97~1.20) | 0.18 | 1.07(0.96~1.19) | 0.21 |
| Q3组 | 1.31(1.18~1.46) | <0.01 | 1.16(1.04~1.29) | 0.01 | 1.16(1.04~1.28) | 0.01 | 1.14(1.03~1.27) | 0.01 |
| Q4组 | 1.53(1.38~1.69) | <0.01 | 1.30(1.18~1.45) | <0.01 | 1.30(1.17~1.44) | <0.01 | 1.24(1.09~1.40) | <0.01 |
| <40岁 | <0.01a | 0.07a | 0.06a | 0.35a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 0.64(0.28~1.43) | 0.27 | 0.57(0.26~1.28) | 0.17 | 0.56(0.25~1.26) | 0.15 | 0.55(0.24~1.23) | 0.14 |
| Q3组 | 1.59(0.85~2.96) | 0.14 | 1.27(0.67~2.39) | 0.46 | 1.31(0.70~2.48) | 0.39 | 1.24(0.66~2.35) | 0.50 |
| Q4组 | 1.92(1.05~3.50) | 0.03 | 1.46(0.78~2.72) | 0.23 | 1.49(0.80~2.79) | 0.21 | 1.15(0.56~2.36) | 0.71 |
| 40~49岁 | <0.01a | <0.01a | <0.01a | 0.03a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.29(0.98~1.71) | 0.07 | 1.22(0.92~1.61) | 0.16 | 1.22(0.92~1.61) | 0.17 | 1.21(0.91~1.60) | 0.18 |
| Q3组 | 1.42(1.09~1.86) | 0.01 | 1.22(0.93~1.60) | 0.14 | 1.23(0.94~1.62) | 0.13 | 1.22(0.93~1.61) | 0.15 |
| Q4组 | 1.76(1.36~2.27) | <0.01 | 1.45(1.11~1.88) | 0.01 | 1.47(1.13~1.91) | <0.01 | 1.43(1.05~1.95) | 0.02 |
| 50~59岁 | <0.01a | <0.01a | <0.01a | 0.04a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.13(0.95~1.35) | 0.16 | 1.07(0.90~1.28) | 0.46 | 1.07(0.89~1.27) | 0.47 | 1.07(0.89~1.27) | 0.48 |
| Q3组 | 1.22(1.03~1.44) | 0.02 | 1.08(0.91~1.28) | 0.38 | 1.08(0.91~1.28) | 0.39 | 1.07(0.90~1.27) | 0.46 |
| Q4组 | 1.49(1.27~1.76) | <0.01 | 1.28(1.08~1.51) | <0.01 | 1.27(1.08~1.50) | <0.01 | 1.22(1.01~1.49) | 0.04 |
| ≥60岁 | <0.01a | <0.01a | <0.01a | 0.03a | ||||
| Q1组 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Q2组 | 1.10(0.94~1.29) | 0.24 | 1.06(0.90~1.24) | 0.48 | 1.05(0.90~1.23) | 0.54 | 1.04(0.89~1.22) | 0.59 |
| Q3组 | 1.25(1.07~1.47) | 0.00 | 1.17(0.99~1.37) | 0.05 | 1.17(0.99~1.37) | 0.06 | 1.15(0.98~1.35) | 0.09 |
| Q4组 | 1.39(1.19~1.62) | <0.01 | 1.27(1.09~1.49) | <0.01 | 1.26(1.07~1.47) | <0.01 | 1.20(0.99~1.44) | 0.05 |
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| Q1组 | 1.00 | <0.01a | 1.00 | <0.01a | 1.00 | <0.01a | 1.00 | <0.01a |
| Q2组 | 1.03(0.89~1.20) | 0.70 | 0.99(0.85~1.15) | 0.91 | 0.98(0.85~1.14) | 0.82 | 0.98(0.84~1.13) | 0.73 |
| Q3组 | 1.19(1.02~1.38) | 0.02 | 1.11(0.95~1.29) | 0.18 | 1.10(0.95~1.28) | 0.20 | 1.08(0.93~1.26) | 0.33 |
| Q4组 | 1.33(1.15~1.54) | <0.01 | 1.21(1.05~1.41) | 0.01 | 1.20(1.03~1.39) | 0.01 | 1.11(0.93~1.33) | 0.24 |
表8 ≥60岁不同CAR分组人群CVD发生率的死亡竞争风险模型分析
Table 8 Analysis of the mortality competitive risk model for the incidence of CVD in different CAR groups aged ≥60 years
| 分组 | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|
| HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | HR(95%CI) | P(P趋势)值 | |
| Q1组 | 1.00 | <0.01a | 1.00 | <0.01a | 1.00 | <0.01a | 1.00 | <0.01a |
| Q2组 | 1.03(0.89~1.20) | 0.70 | 0.99(0.85~1.15) | 0.91 | 0.98(0.85~1.14) | 0.82 | 0.98(0.84~1.13) | 0.73 |
| Q3组 | 1.19(1.02~1.38) | 0.02 | 1.11(0.95~1.29) | 0.18 | 1.10(0.95~1.28) | 0.20 | 1.08(0.93~1.26) | 0.33 |
| Q4组 | 1.33(1.15~1.54) | <0.01 | 1.21(1.05~1.41) | 0.01 | 1.20(1.03~1.39) | 0.01 | 1.11(0.93~1.33) | 0.24 |
| [1] |
GBD 2021 Diseases and Injuries Collaborators. Global incidence,prevalence,years lived with disability(YLDs),disability-adjusted life-years(DALYs),and healthy life expectancy(HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations,1990-2021:a systematic analysis for the Global Burden of Disease Study 2021[J]. Lancet,2024,403(10440):2133-2161. DOI:10.1016/S0140-6736(24)00757-8.
|
| [2] |
GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations,1990-2021:a systematic analysis for the Global Burden of Disease Study 2021[J]. Lancet,2024,403(10440):2100-2132. DOI:10.1016/S0140-6736(24)00367-2.
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
Emerging Risk Factors Collaboration,
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
吴寿岭,赵晓琳,高明,等. 唐山地区健康成年人群血清高敏C反应蛋白的正常值参考范围[J]. 中华高血压杂志,2013,21(7):675-678. DOI:10.16439/j.cnki.1673-7245.2013.07.004.
|
| [38] |
|
| [1] | 柴智浩, 张维森, 罗娇玲, 朱峰, 朱彤, 靳雅丽, 潘静, 卢映君, 江朝强. 中老年人社会经济状况在少儿期父母文化与认知功能间的中介效应:基于广州生物库队列研究[J]. 中国全科医学, 2026, 29(21): 2959-2966. |
| [2] | 韩聪聪, 邱欣雨, 单春方, 宋宁, 陈清杰, 穆拉迪力·阿卜杜热合曼, 李晓梅, 杨毅宁, 赵倩. 代谢肥胖表型对急性冠脉综合征患者经皮冠状动脉介入治疗远期预后的影响研究[J]. 中国全科医学, 2026, 29(21): 2950-2958. |
| [3] | 刘帅, 苑世朝, 刘琰, 贾硕贤, 赵岩, 王紫怡, 周春华, 于静. 两性霉素B治疗侵袭性真菌病的疗效、安全性及经济性评价:一项回顾性队列研究[J]. 中国全科医学, 2026, 29(21): 2967-2974. |
| [4] | 热伊莱·麦麦提, 周燚然, 武云, 刘稹诚, 卢耀勤, 吴海燕. 高血压患者新型肥胖指标与心血管疾病发病风险的关联研究[J]. 中国全科医学, 2026, 29(20): 2836-2845. |
| [5] | 袁玉娟, 陶静, 王颖, 彭辉, 杨毅宁. 中性粒细胞百分比/白蛋白比值与急性心肌梗死患者院内全因死亡和心源性休克的相关性研究[J]. 中国全科医学, 2026, 29(18): 2489-2497. |
| [6] | 胡敏, 吕向东. 远程心电人工智能诊断的准确性研究[J]. 中国全科医学, 2026, 29(18): 2498-2503. |
| [7] | 邱欣雨, 赵倩, 陈玉斐, 加木勒·买买提依明, 韩聪聪, 爱克丹·艾尔肯, 李晓梅, 杨毅宁. 体重状态及其代谢特征对收缩压纵向轨迹的影响:一项队列研究[J]. 中国全科医学, 2026, 29(15): 2006-2013. |
| [8] | 甄锐, 谷旭放, 高晟玮, 张博文, 任真娟, 杨睿璇. 1990—2021年中国归因于代谢风险因素的心血管疾病负担及2022—2035年趋势预测研究[J]. 中国全科医学, 2026, 29(15): 2077-2083. |
| [9] | 邱艳丽, 高永银, 卞雪艳, 王雪, 李越. 脉搏波传导速度对癌症患者全因和心血管相关死亡率的预测价值研究[J]. 中国全科医学, 2026, 29(14): 1890-1897. |
| [10] | 刘翔, 陈红, 崔睿, 郭志超, 李盼盼, 曹子龙, 纪伊晴, 俞文雅. 特大城市儿童早期发展一致性与差异性:一项回顾性队列研究[J]. 中国全科医学, 2026, 29(11): 1411-1421. |
| [11] | 胡嘉琦, 李端, 方昊, 樊兴颖, 杜薇, 周涵妮. 基于体检人群队列的高尿酸血症非遗传因素风险预测模型构建研究[J]. 中国全科医学, 2026, 29(10): 1324-1333. |
| [12] | 杨旭, 樊洁婷, 宋红艳, 冯盼盼, 郝婧宇, 姚弥. 基层全科医生心血管疾病风险评估与沟通策略[J]. 中国全科医学, 2026, 29(10): 1294-1299. |
| [13] | 李秋春, 苏萍, 逄锦宏, 陈巧巧, 赵颖颖, 何蕊言, 王玥, 陈学禹, 乔俊鹏, 迟蔚蔚. 三酰甘油-葡萄糖指数与心血管-肾脏-代谢综合征0~3期人群心血管疾病的关联性:一项前瞻性队列研究[J]. 中国全科医学, 2026, 29(09): 1129-1136. |
| [14] | 张钧阳, 曾钇尧, 金富璐, 王培育, 蒋雨枫, 周亚峰, 赵良平. 糖化白蛋白和糖化血红蛋白与中重度主动脉瓣疾病患者主动脉瓣钙化的关系研究[J]. 中国全科医学, 2026, 29(08): 1008-1012. |
| [15] | 裴志怡, 张晓欣, 林佳艺, 张向毅, 康晓凤. 基于患者决策辅助工具国际标准的心血管领域患者决策辅助工具质量及应用效果的系统评价[J]. 中国全科医学, 2026, 29(07): 945-952. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










