中国全科医学 ›› 2024, Vol. 27 ›› Issue (06): 670-678.DOI: 10.12114/j.issn.1007-9572.2023.0349
所属专题: 孕产妇健康研究最新文章合辑
袁仙仙1, 李静2, 王佳1, 张可欣1, 杨蕊华1, 郑薇1, 李光辉1,*( )
)
YUAN Xianxian1, LI Jing2, WANG Jia1, ZHANG Kexin1, YANG Ruihua1, ZHENG Wei1, LI Guanghui1,*()
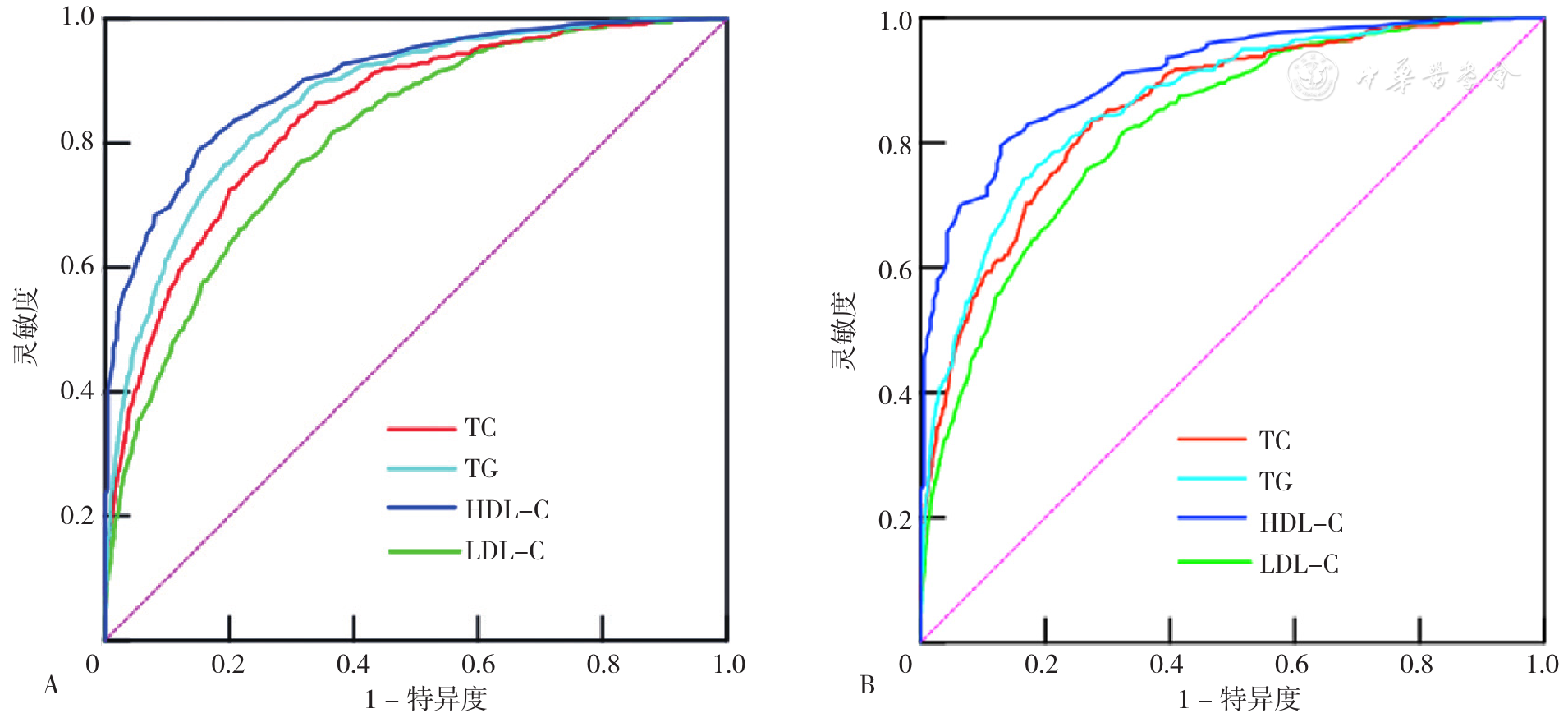
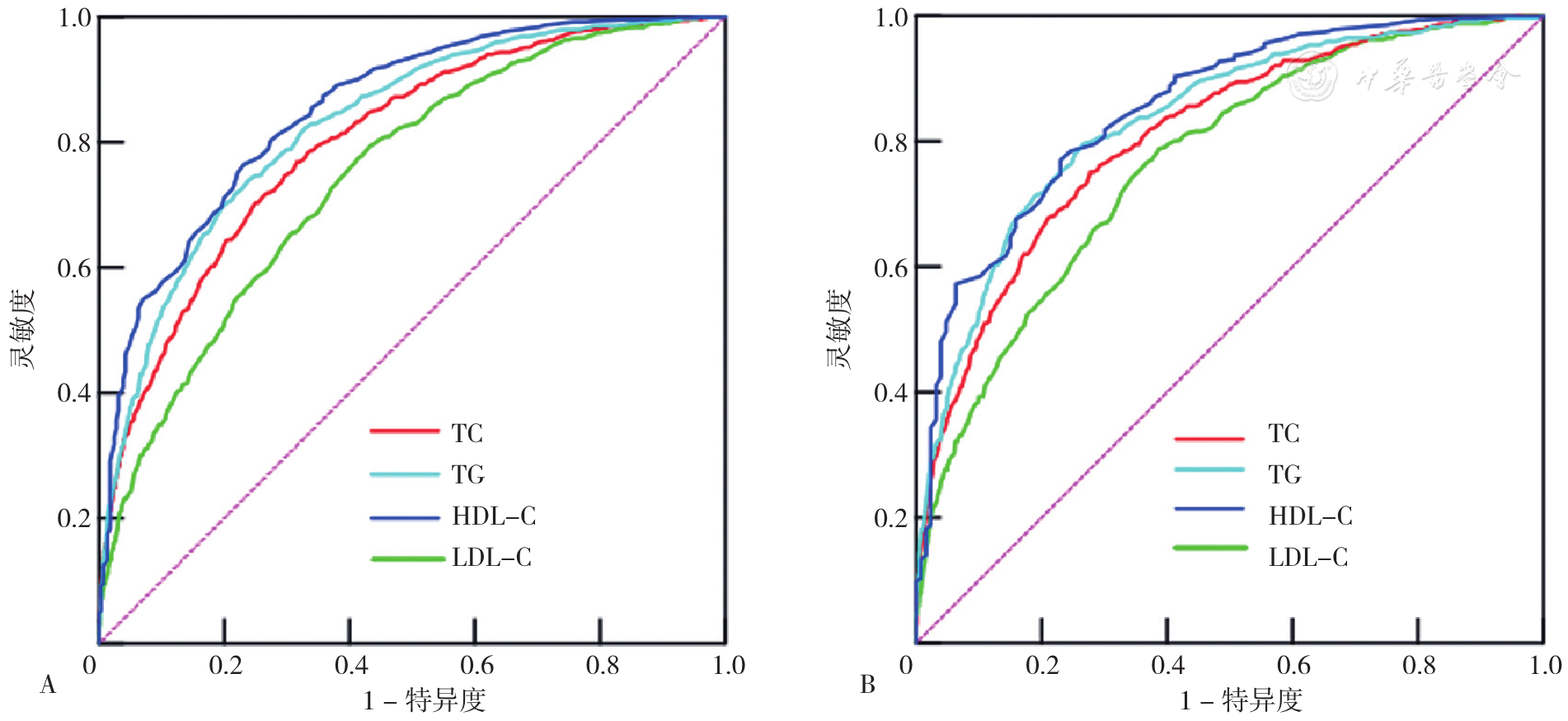
摘要: 背景 妊娠期血脂异常升高可对母儿健康造成不良影响,不仅增加了子痫前期、妊娠期糖尿病(GDM)、高甘油三酯胰腺炎、晚期流产、早产以及巨大儿的发生风险,亦显著增加了母儿产后心血管疾病的风险。目的 分析妊娠早、中、晚期血脂异常的分布特征及其早期血脂水平对妊娠中、晚期血脂异常的预测价值。方法 本研究为单中心回顾性研究,纳入2018年1月—2019年6月在首都医科大学附属北京妇产医院产科建档产检至分娩的单胎孕妇,收集临床资料及妊娠早、中、晚期血脂数据[总胆固醇(TC)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)、高密度脂蛋白胆固醇(HDL-C)]。以首都医科大学附属北京妇产医院妊娠期血脂参考范围作为血脂异常诊断标准:包括高总胆固醇血症、高甘油三酯血症、低高密度脂蛋白胆固醇血症和高低密度脂蛋白胆固醇血症。采用二分类Logistic回归分析妊娠早期血脂水平与妊娠中、晚期血脂异常的相关性,绘制受试者工作特征(ROC)曲线,计算曲线下面积(AUC),评价妊娠早期血脂水平对妊娠中、晚期血脂异常的预测价值,根据灵敏度和特异度确定最佳截断值。结果 研究共纳入单胎孕妇8 511名,平均年龄为(31.7±3.9)岁,平均孕前BMI为(21.7±3.2)kg/m2,其中孕前低体质量988名(11.6%)、正常体质量5 568名(65.4%)、超重1 271名(14.9%)、肥胖366名(4.3%),GDM孕妇1 415名(16.7%),妊娠期高血压疾病(HDP)孕妇650名(7.6%)。妊娠中、晚期TC、TG、LDL-C水平均高于妊娠早期(P<0.05),妊娠晚期HDL-C水平高于妊娠早期,但低于妊娠中期(P<0.05)。妊娠早期血脂异常患病率为23.4%(1 990/8 511),妊娠中、晚期血脂异常患病率低于妊娠早期(P<0.05)。孕前超重、肥胖孕妇妊娠早期血脂异常患病率高于孕前正常体质量孕妇,但妊娠晚期血脂异常患病率比较,差异无统计学意义(P>0.05);GDM组孕妇妊娠早、中期血脂异常患病率均高于非GDM孕妇,HDP孕妇妊娠早、中、晚期血脂异常患病率高于非HDP孕妇(P<0.05)。排除可能影响血脂的妊娠合并症及并发症后,妊娠早期预测妊娠中期血脂异常的最佳截断值分别为TC 4.485 mmol/L(AUC=0.854)、TG 1.325 mmol/L(AUC=0.864)、HDL-C 1.275 mmol/L(AUC=0.908)、LDL-C 2.265 mmol/L(AUC=0.823);妊娠早期预测妊娠晚期血脂异常的最佳截断值分别为TC 4.485 mmol/L(AUC=0.809)、TG 1.145 mmol/L(AUC=0.833)、HDL-C 1.285 mmol/L(AUC=0.851)、LDL-C 2.195 mmol/L(AUC=0.766)。结论 妊娠期血脂异常患病率并未增加,不同孕前BMI、GDM与非GDM、HDP与非HDP孕妇之间妊娠期血脂异常患病率具有显著差异,妊娠早期血脂水平有预测妊娠中晚期血脂异常的价值。