
中国全科医学 ›› 2022, Vol. 25 ›› Issue (26): 3263-3269.DOI: 10.12114/j.issn.1007-9572.2022.0293
所属专题: 肿瘤最新文章合辑
李艳1, 王昆仑1, 杨晖1, 赵二江2, 李炳旭3, 李胜磊1, 董小滔1, 袁翎1,*( )
)
收稿日期:2022-02-14
修回日期:2022-06-19
出版日期:2022-09-15
发布日期:2022-07-06
通讯作者:
袁翎
基金资助:
Yan LI1, Kunlun WANG1, Hui YANG1, Erjiang ZHAO2, Bingxu LI3, Shenglei LI1, Xiaotao DONG1, Ling YUAN1,*()
Received:2022-02-14
Revised:2022-06-19
Published:2022-09-15
Online:2022-07-06
Contact:
Ling YUAN
About author:摘要: 背景 仅有少量晚期食管鳞状细胞癌(ESCC)患者可从免疫治疗中获益,总体疗效不令人满意。因此,选择有效的预后观察指标十分重要。 目的 探讨乳酸脱氢酶(LDH)预测晚期ESCC患者免疫治疗的预后价值。 方法 选取2016年10月至2019年10月在河南省肿瘤医院经病理及影像学检查确诊为晚期ESCC患者为研究对象。从医院电子病历系统中回顾性收集患者基线资料,并收集患者免疫治疗第8周LDH水平。随访截至2021-08-31,记录随访结果。观察死亡情况、患者疾病缓解情况,并记录无进展生存期(PFS)和总生存期(OS)。采用Kaplan-Meier法绘制不同基线LDH水平患者PFS、OS生存曲线以进行生存分析,生存曲线的比较采用Log-rank检验;采用多因素Cox比例风险回归分析探究晚期ESCC患者免疫治疗PFS、OS的影响因素。 结果 44例患者中基线LDH低水平(基线LDH<200 U/L)者28例,基线LDH高水平(基线LDH≥200 U/L)者16例。基线LDH低水平的患者客观缓解率(ORR)高于基线LDH高水平患者(χ2=8.522,P=0.013)。44例患者中病情进展(PD)8例,无PD患者36例。PD患者?LDH(治疗过程中LDH的变化)高于无PD患者(t=2.394,P=0.021)。截至2021-08-31,9例(20.5%)患者存活;中位PFS为6(2,11)个月;中位OS为11(7,18)个月。基线LDH低水平与基线LDH高水平患者PFS、OS比较,差异均有统计学意义(χ2值分别为6.790、12.327,P值分别为0.009、<0.001)。多因素Cox比例风险回归分析结果显示,基线LDH水平是晚期ESCC患者免疫治疗后PFS的影响因素〔HR=2.686,95%CI(1.274,5.664),P=0.009〕;基线LDH水平〔HR=17.440,95%CI(2.254,134.962),P=0.001〕、血红蛋白〔HR=0.005,95%CI(<0.001,0.120),P=0.001〕、单核细胞计数〔HR=0.066,95%CI(0.008,0.525),P=0.010〕是晚期ESCC患者免疫治疗后OS的影响因素。 结论 基线LDH可作为晚期ESCC患者免疫治疗预后的预测指标,且基线LDH低水平者有更好的PFS及OS。
| 项目 | 总人群(n=44) | 基线LDH低水平者(n=28) | 基线LDH高水平者(n=16) | |
|---|---|---|---|---|
| 年龄〔M(P25,P75),岁〕 | 64.5(57.0,69.8) | 63.0(55.2,68.8) | 67.0(57.0,72.0) | |
| 性别〔n(%)〕 | ||||
| 男 | 34(77.3) | 22(78.6) | 12(75.0) | |
| 女 | 10(22.7) | 6(21.4) | 4(25.0) | |
| 病变部位〔n(%)〕 | ||||
| 颈段+上段 | 6(13.6) | 4(14.3) | 2(12.5) | |
| 中下段 | 38(86.4) | 24(85.7) | 14(87.5) | |
| 有无吸烟史〔n(%)〕 | ||||
| 有 | 22(50.0) | 15(53.6) | 7(43.8) | |
| 无 | 22(50.0) | 13(46.4) | 9(56.2) | |
| 肿瘤分化程度〔n(%)〕 | ||||
| 高分化+中分化 | 30(68.2) | 21(75.0) | 9(56.2) | |
| 低分化 | 14(31.8) | 7(25.0) | 7(43.8) | |
| 既往行手术治疗〔n(%)〕 | ||||
| 有 | 10(22.7) | 7(25.0) | 3(18.8) | |
| 无 | 34(77.3) | 21(75.0) | 13(81.2) | |
| 既往放射治疗 | ||||
| 有 | 29(65.9) | 18(64.3) | 11(68.8) | |
| 无 | 15(34.1) | 10(35.7) | 5(31.2) | |
| 转移累及器官数〔n(%)〕 | ||||
| ≤2个 | 36(81.8) | 24(85.7) | 12(75.0) | |
| ≥3个 | 8(18.2) | 4(14.3) | 4(25.0) | |
| 基线LDH水平〔M(P25,P75),U/L〕 | 190.0(158.5,237.0) | 177.0(136.0,188.2) | 273.0(217.0,328.0) | |
| 血清白蛋白〔M(P25,P75),g/L〕 | 40.00(36.20,43.10) | 41.00(37.40,44.10) | 39.00(35.75,40.05) | |
| 血红蛋白〔M(P25,P75),g/L〕 | 122.0(105.0,140.0) | 120.5(106.0,137.8) | 122.0(104.0,143.0) | |
| 淋巴细胞计数〔M(P25,P75),×109/L〕 | 1.01(0.71,1.44) | 0.98(0.65,1.36) | 1.09(0.95,1.91) | |
| 单核细胞计数〔M(P25,P75),×109/L〕 | 0.27(0.18,0.34) | 0.26(0.15,0.34) | 0.31(0.22,0.43) | |
表1 总体患者及不同基线LDH水平患者基线资料
Table 1 Baseline characteristics analysis of ESCC participants after immunotherapy on the whole and by baseline LDH level
| 项目 | 总人群(n=44) | 基线LDH低水平者(n=28) | 基线LDH高水平者(n=16) | |
|---|---|---|---|---|
| 年龄〔M(P25,P75),岁〕 | 64.5(57.0,69.8) | 63.0(55.2,68.8) | 67.0(57.0,72.0) | |
| 性别〔n(%)〕 | ||||
| 男 | 34(77.3) | 22(78.6) | 12(75.0) | |
| 女 | 10(22.7) | 6(21.4) | 4(25.0) | |
| 病变部位〔n(%)〕 | ||||
| 颈段+上段 | 6(13.6) | 4(14.3) | 2(12.5) | |
| 中下段 | 38(86.4) | 24(85.7) | 14(87.5) | |
| 有无吸烟史〔n(%)〕 | ||||
| 有 | 22(50.0) | 15(53.6) | 7(43.8) | |
| 无 | 22(50.0) | 13(46.4) | 9(56.2) | |
| 肿瘤分化程度〔n(%)〕 | ||||
| 高分化+中分化 | 30(68.2) | 21(75.0) | 9(56.2) | |
| 低分化 | 14(31.8) | 7(25.0) | 7(43.8) | |
| 既往行手术治疗〔n(%)〕 | ||||
| 有 | 10(22.7) | 7(25.0) | 3(18.8) | |
| 无 | 34(77.3) | 21(75.0) | 13(81.2) | |
| 既往放射治疗 | ||||
| 有 | 29(65.9) | 18(64.3) | 11(68.8) | |
| 无 | 15(34.1) | 10(35.7) | 5(31.2) | |
| 转移累及器官数〔n(%)〕 | ||||
| ≤2个 | 36(81.8) | 24(85.7) | 12(75.0) | |
| ≥3个 | 8(18.2) | 4(14.3) | 4(25.0) | |
| 基线LDH水平〔M(P25,P75),U/L〕 | 190.0(158.5,237.0) | 177.0(136.0,188.2) | 273.0(217.0,328.0) | |
| 血清白蛋白〔M(P25,P75),g/L〕 | 40.00(36.20,43.10) | 41.00(37.40,44.10) | 39.00(35.75,40.05) | |
| 血红蛋白〔M(P25,P75),g/L〕 | 122.0(105.0,140.0) | 120.5(106.0,137.8) | 122.0(104.0,143.0) | |
| 淋巴细胞计数〔M(P25,P75),×109/L〕 | 1.01(0.71,1.44) | 0.98(0.65,1.36) | 1.09(0.95,1.91) | |
| 单核细胞计数〔M(P25,P75),×109/L〕 | 0.27(0.18,0.34) | 0.26(0.15,0.34) | 0.31(0.22,0.43) | |
| 分类 | 例数 | ORR | SD | PD |
|---|---|---|---|---|
| 基线LDH低水平者 | 28 | 16(57.2) | 10(35.7) | 2(7.1) |
| 基线LDH高水平者 | 16 | 3(18.8) | 7(43.7) | 6(37.5) |
表2 基线LDH低水平与基线LDH高水平患者预后情况〔n(%)〕
Table 2 Prognosis of ESCC patients with low and high baseline LDH levels
| 分类 | 例数 | ORR | SD | PD |
|---|---|---|---|---|
| 基线LDH低水平者 | 28 | 16(57.2) | 10(35.7) | 2(7.1) |
| 基线LDH高水平者 | 16 | 3(18.8) | 7(43.7) | 6(37.5) |
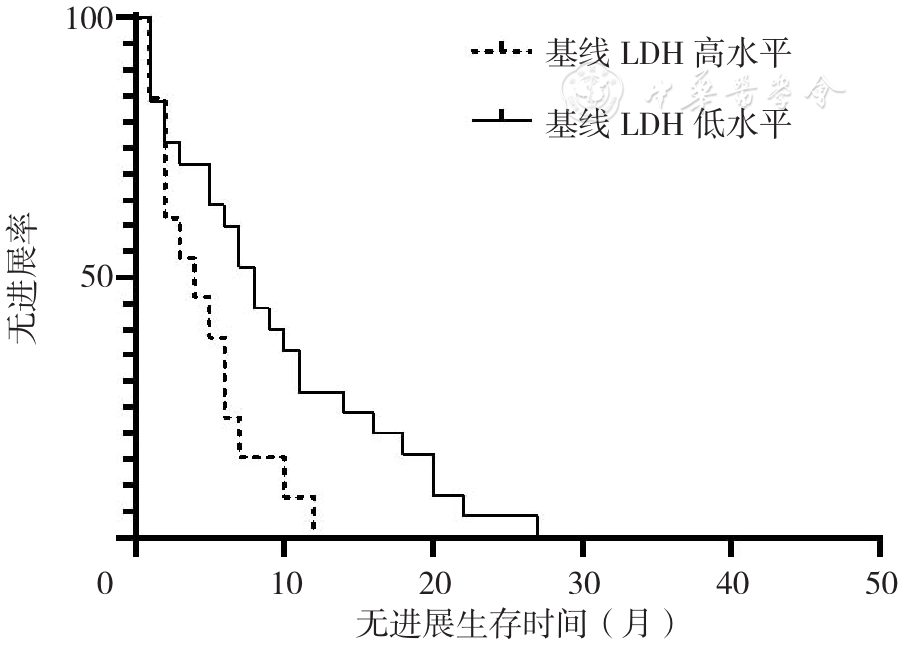
图1 基线LDH低水平与基线LDH高水平患者PFS生存曲线注:LDH=乳酸脱氢酶
Figure 1 Progression-free survival curves of ESCC patients with low and high baseline LDH
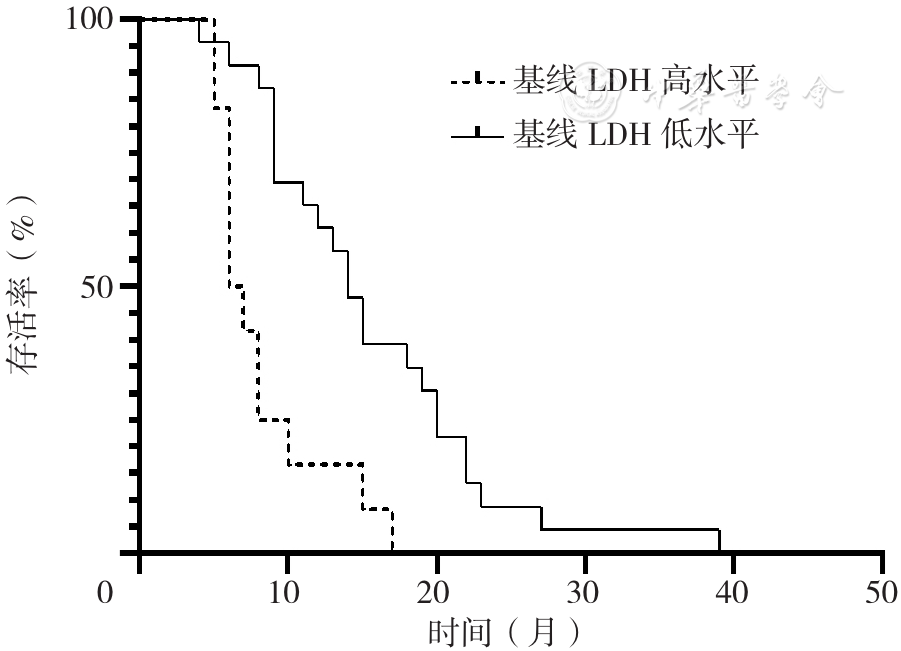
图2 基线LDH低水平与基线LDH高水平患者OS生存曲线
Figure 2 Overall survival curves of ESCC patients with low and high baseline LDH
| 变量 | 赋值 |
|---|---|
| 年龄 | 实测值 |
| 性别 | 男=0,女=1 |
| 病变部位 | 颈段+上段=0,中下段=1 |
| 有无吸烟史 | 无=0,有=1 |
| 肿瘤分化程度 | 低分化=0,高分化+中分化=1 |
| 既往行手术治疗 | 无=0,有=1 |
| 既往放射治疗 | 无=0,有=1 |
| 转移累及器官数 | ≤2个=0,≥3个=1 |
| 基线LDH水平 | <200 U/L=0,≥200 U/L=1 |
| 血清白蛋白 | <40 g/L=0,≥40 g/L=1 |
| 血红蛋白 | <130 g/L=0,≥130 g/L=1 |
| 淋巴细胞计数 | <1.39×109/L=0,≥1.39×109/L=1 |
| 单核细胞计数 | <0.39×109/L=0,≥0.39×109/L=1 |
表3 晚期ESCC患者免疫治疗后预后影响因素单因素和多因素Cox比例风险回归分析变量赋值
Table 3 Variable assignment for potential factors associated with prognosis in patients with advanced ESCC after immunotherapy analyzed using univariate and multivariate Cox regression
| 变量 | 赋值 |
|---|---|
| 年龄 | 实测值 |
| 性别 | 男=0,女=1 |
| 病变部位 | 颈段+上段=0,中下段=1 |
| 有无吸烟史 | 无=0,有=1 |
| 肿瘤分化程度 | 低分化=0,高分化+中分化=1 |
| 既往行手术治疗 | 无=0,有=1 |
| 既往放射治疗 | 无=0,有=1 |
| 转移累及器官数 | ≤2个=0,≥3个=1 |
| 基线LDH水平 | <200 U/L=0,≥200 U/L=1 |
| 血清白蛋白 | <40 g/L=0,≥40 g/L=1 |
| 血红蛋白 | <130 g/L=0,≥130 g/L=1 |
| 淋巴细胞计数 | <1.39×109/L=0,≥1.39×109/L=1 |
| 单核细胞计数 | <0.39×109/L=0,≥0.39×109/L=1 |
| 项目 | PFS | OS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | Wald χ2值 | P值 | HR(95%CI) | B | SE | Wald χ2值 | P值 | HR(95%CI) | |
| 年龄 | 0.002 | 0.018 | 0.018 | 0.894 | 1.002(0.967,1.039) | 0.002 | 0.020 | 0.006 | 0.937 | 1.002(0.962,1.043) |
| 性别 | -0.226 | 0.398 | 0.322 | 0.570 | 0.798(0.365,1.741) | 0.422 | 0.412 | 1.049 | 0.306 | 1.524(0.680,3.416) |
| 病变部位 | -0.687 | 0.624 | 1.210 | 0.271 | 0.503(0.148,1.711) | -1.023 | 0.567 | 3.248 | 0.072 | 0.360(0.118,1.094) |
| 有无吸烟史 | 0.292 | 0.328 | 0.793 | 0.373 | 1.339(0.704,2.545) | 0.241 | 0.360 | 0.449 | 0.503 | 1.272(0.629,2.575) |
| 肿瘤分化程度 | -0.340 | 0.352 | 0.935 | 0.334 | 0.711(0.357,1.419) | -0.560 | 0.385 | 2.113 | 0.146 | 0.571(0.268,1.215) |
| 既往行手术治疗 | 0.151 | 0.352 | 0.185 | 0.667 | 1.164(0.583,2.321) | 0.493 | 0.392 | 1.577 | 0.209 | 1.637(0.759,3.531) |
| 既往放射治疗 | 0.472 | 0.353 | 1.784 | 0.182 | 1.603(0.802,3.205) | 0.512 | 0.398 | 1.660 | 0.198 | 1.669(0.766,3.638) |
| 转移累及器官数 | 0.502 | 0.493 | 1.035 | 0.309 | 1.651(0.628,4.341) | 0.418 | 0.544 | 0.592 | 0.442 | 1.519(0.524,4.408) |
| 基线LDH | 0.884 | 0.367 | 5.794 | 0.016 | 2.420(1.178,4.971) | 1.291 | 0.407 | 10.070 | 0.004 | 3.637(1.638,8.074) |
| 血清白蛋白 | 0.714 | 0.453 | 2.480 | 0.115 | 2.042(0.840,4.964) | 0.398 | 0.491 | 0.658 | 0.417 | 1.489(0.569,3.898) |
| 血红蛋白 | -0.241 | 0.364 | 0.439 | 0.508 | 0.786(0.385,1.604) | -0.453 | 0.409 | 1.231 | 0.267 | 0.636(0.285,1.415) |
| 淋巴细胞计数 | -0.014 | 0.374 | 0.001 | 0.970 | 0.989(0.511,1.913) | -0.493 | 0.436 | 1.278 | 0.258 | 0.611(0.260,1.436) |
| 单核细胞计数 | -0.011 | 0.337 | 0.001 | 0.973 | 0.989(0.511,1.915) | -0.523 | 0.362 | 2.084 | 0.149 | 0.593(0.291,1.206) |
表4 晚期ESCC患者免疫治疗后PFS、OS影响因素的单因素Cox比例风险回归分析
Table 4 Univariate Cox regression analysis of influencing factors of progression-free survival and overall survival in patients with advanced ESCC after immunotherapy
| 项目 | PFS | OS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | Wald χ2值 | P值 | HR(95%CI) | B | SE | Wald χ2值 | P值 | HR(95%CI) | |
| 年龄 | 0.002 | 0.018 | 0.018 | 0.894 | 1.002(0.967,1.039) | 0.002 | 0.020 | 0.006 | 0.937 | 1.002(0.962,1.043) |
| 性别 | -0.226 | 0.398 | 0.322 | 0.570 | 0.798(0.365,1.741) | 0.422 | 0.412 | 1.049 | 0.306 | 1.524(0.680,3.416) |
| 病变部位 | -0.687 | 0.624 | 1.210 | 0.271 | 0.503(0.148,1.711) | -1.023 | 0.567 | 3.248 | 0.072 | 0.360(0.118,1.094) |
| 有无吸烟史 | 0.292 | 0.328 | 0.793 | 0.373 | 1.339(0.704,2.545) | 0.241 | 0.360 | 0.449 | 0.503 | 1.272(0.629,2.575) |
| 肿瘤分化程度 | -0.340 | 0.352 | 0.935 | 0.334 | 0.711(0.357,1.419) | -0.560 | 0.385 | 2.113 | 0.146 | 0.571(0.268,1.215) |
| 既往行手术治疗 | 0.151 | 0.352 | 0.185 | 0.667 | 1.164(0.583,2.321) | 0.493 | 0.392 | 1.577 | 0.209 | 1.637(0.759,3.531) |
| 既往放射治疗 | 0.472 | 0.353 | 1.784 | 0.182 | 1.603(0.802,3.205) | 0.512 | 0.398 | 1.660 | 0.198 | 1.669(0.766,3.638) |
| 转移累及器官数 | 0.502 | 0.493 | 1.035 | 0.309 | 1.651(0.628,4.341) | 0.418 | 0.544 | 0.592 | 0.442 | 1.519(0.524,4.408) |
| 基线LDH | 0.884 | 0.367 | 5.794 | 0.016 | 2.420(1.178,4.971) | 1.291 | 0.407 | 10.070 | 0.004 | 3.637(1.638,8.074) |
| 血清白蛋白 | 0.714 | 0.453 | 2.480 | 0.115 | 2.042(0.840,4.964) | 0.398 | 0.491 | 0.658 | 0.417 | 1.489(0.569,3.898) |
| 血红蛋白 | -0.241 | 0.364 | 0.439 | 0.508 | 0.786(0.385,1.604) | -0.453 | 0.409 | 1.231 | 0.267 | 0.636(0.285,1.415) |
| 淋巴细胞计数 | -0.014 | 0.374 | 0.001 | 0.970 | 0.989(0.511,1.913) | -0.493 | 0.436 | 1.278 | 0.258 | 0.611(0.260,1.436) |
| 单核细胞计数 | -0.011 | 0.337 | 0.001 | 0.973 | 0.989(0.511,1.915) | -0.523 | 0.362 | 2.084 | 0.149 | 0.593(0.291,1.206) |
| 项目 | B | SE | Wald χ2值 | P值 | HR(95%CI) |
|---|---|---|---|---|---|
| 基线LDH | 2.859 | 1.044 | 7.498 | 0.001 | 17.440(2.254,134.962) |
| 血红蛋白 | -5.321 | 1.633 | 10.614 | 0.001 | 0.005(<0.001,0.120) |
| 单核细胞计数 | -2.713 | 1.056 | 6.604 | 0.010 | 0.066(0.008,0.525) |
表5 晚期ESCC患者免疫治疗后OS影响因素的多因素Cox比例风险回归分析
Table 5 Multivariate Cox regression analysis of influencing factors of overall survivalin patients with advanced ESCC after immunotherapy
| 项目 | B | SE | Wald χ2值 | P值 | HR(95%CI) |
|---|---|---|---|---|---|
| 基线LDH | 2.859 | 1.044 | 7.498 | 0.001 | 17.440(2.254,134.962) |
| 血红蛋白 | -5.321 | 1.633 | 10.614 | 0.001 | 0.005(<0.001,0.120) |
| 单核细胞计数 | -2.713 | 1.056 | 6.604 | 0.010 | 0.066(0.008,0.525) |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
麦海强,莫浩元,洪明晃,等. 鼻咽癌放疗前血红蛋白浓度对局部控制的影响[J]. 癌症,2005,24(6):727-730. DOI:10.3321/j.issn:1000-467X.2005.06.020.
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [1] | 徐艳朋, 黄佩, 张平平, 罗艳, 施晓琪, 吴柳松, 陈艳, 何志旭. 急性T淋巴细胞白血病β-肾上腺素受体的表达情况及临床意义研究[J]. 中国全科医学, 2025, 28(27): 3391-3398. |
| [2] | 杨晨, 陈瞳, 张利方, 张洪旭, 李鹏飞, 张雪娟. 达格列净对老年乳腺癌幸存者射血分数保留的心力衰竭合并2型糖尿病患者的预后影响研究[J]. 中国全科医学, 2025, 28(24): 3053-3058. |
| [3] | 阮万百, 李俊峰, 尹艳梅, 彭磊, 朱克祥. 胰腺癌靶向治疗及免疫治疗的研究新进展[J]. 中国全科医学, 2025, 28(23): 2950-2960. |
| [4] | 陈飞, 王金英, 于海搏, 李新, 张佳佳, 申曼, 詹晓凯, 汤然, 范斯斌, 赵凤仪, 张天宇, 黄仲夏. 中性粒细胞明胶酶相关运载蛋白、T细胞免疫球蛋白粘蛋白受体1、血管细胞黏附分子-1和激活素A升高在新诊断多发性骨髓瘤患者中的意义研究[J]. 中国全科医学, 2025, 28(22): 2740-2749. |
| [5] | 曹干, 邓毅凡, 何胜虎, 张晶. 乳酸脱氢酶与白蛋白比值与急性ST段抬高型心肌梗死急诊经皮冠状动脉介入治疗术后患者预后的相关性研究[J]. 中国全科医学, 2025, 28(15): 1878-1883. |
| [6] | 张树静, 孙立新, 曹雨晴. 人乳头瘤病毒相关宫颈腺癌与非人乳头瘤相关宫颈腺癌的临床病理特征比较及预后研究[J]. 中国全科医学, 2025, 28(14): 1758-1764. |
| [7] | 李秋敬, 商娜, 高倩, 杨黎, 郭树彬. 基于腹部CT的骨骼肌量联合危重症评分对老年腹腔脓毒症患者预后的预测价值研究[J]. 中国全科医学, 2025, 28(12): 1459-1464. |
| [8] | 张玉双, 吴忠冰, 黄鸣, 贾蕾, 高爽, 赵伟鹏, 李晶. 基于非靶代谢组学探究食管鳞状细胞癌津血亏虚证患者的代谢特征[J]. 中国全科医学, 2025, 28(12): 1513-1519. |
| [9] | 王德祥, 原佳雯, 陆沁云, 杭宇豪, 鲁俊, 程璐. 清肺化瘀通腑方治疗时机对脓毒症相关急性呼吸窘迫综合征治疗效果及预后的影响研究[J]. 中国全科医学, 2025, 28(12): 1500-1505. |
| [10] | 张沛, 杨萌, 高春林, 夏正坤. 加味升降散治疗儿童急性肾损伤和急性肾脏病效果和预后的影响研究[J]. 中国全科医学, 2025, 28(11): 1376-1382. |
| [11] | 王一荃, 陈万佳, 刘旺意, 张璐芸, 邓跃毅. 发酵虫草菌粉治疗慢性肾脏病4期患者的预后效果:基于回顾性队列研究[J]. 中国全科医学, 2025, 28(09): 1084-1091. |
| [12] | 宋芬芬, 李胜棉. 基于卡瑞利珠单抗的方案治疗局部晚期及转移性食管癌的真实世界研究[J]. 中国全科医学, 2025, 28(07): 844-852. |
| [13] | 张少通, 王博, 张明瑞, 马桂燕, 柳少光. 使用降钙素原轨迹识别脓毒症亚表型及风险分层研究[J]. 中国全科医学, 2025, 28(05): 594-600. |
| [14] | 朱露, 艾军, 廖生武, 黄淑婷, 龚妮容, 孔耀中, 刘德慧, 窦献蕊, 张广清. 预后营养指数对腹膜透析患者心血管疾病死亡的影响:一项多中心回顾性队列研究[J]. 中国全科医学, 2025, 28(05): 568-574. |
| [15] | 杜慧杰, 刘星雨, 徐明欢, 杨学智, 张慧琴, 莫佳丽, 卢依, 况杰. 急性缺血性脑卒中预后预测研究的应用进展:以机器学习预测模型为例[J]. 中国全科医学, 2025, 28(05): 554-560. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










