
中国全科医学 ›› 2022, Vol. 25 ›› Issue (24): 2965-2974.DOI: 10.12114/j.issn.1007-9572.2022.0237
所属专题: 心血管最新文章合集
李琴1,2,3, 檀鑫3, 姜文溪3, 袁梦3, 倪慧3, 王媛3, 杜杰1,2,3,*( )
)
收稿日期:2022-02-11
修回日期:2022-05-23
出版日期:2022-08-20
发布日期:2022-06-30
通讯作者:
杜杰
基金资助:
Qin LI1,2,3, Xin TAN3, Wenxi JIANG3, Meng YUAN3, Hui NI3, Yuan WANG3, Jie DU1,2,3,*()
Received:2022-02-11
Revised:2022-05-23
Published:2022-08-20
Online:2022-06-30
Contact:
Jie DU
About author:摘要: 背景 对急性心肌梗死(AMI)患者进行风险分层对临床决策和预后评估具有重要临床意义,由于AMI患者临床特征及治疗模式正在不断发生改变,现有的风险评分可能并不适用于临床实际情况,因此需要提高AMI患者经皮冠状动脉介入治疗(PCI)后远期主要不良心血管事件的预测准确性以制订患者个性化的管理策略。 目的 构建预测AMI患者PCI后远期主要不良心血管事件的风险模型。 方法 纳入2019年1—7月于首都医科大学附属北京安贞医院接受PCI的AMI患者1 130例,根据纳入、排除标准最终纳入962例患者,收集其一般资料和实验室检查指标。对所有患者进行电话随访,中位随访时间为2.4年,以全因死亡、非致死性心肌梗死、非致死性卒中、恶性心律失常、新发心力衰竭或心力衰竭加重再入院、非计划内的血运重建作为主要不良心血管事件。根据患者随访期间是否发生主要不良心血管事件分为事件组122例和非事件组840例。采用Lasso回归筛选远期主要不良心血管事件的危险因素,多因素Logistic回归分析构建预测模型,并绘制列线图。采用受试者工作特征(ROC)曲线分析模型预测AMI患者PCI后发生远期主要不良心血管事件的效能,使用净重分类改善指标(NRI)和综合判别指数(IDI)对预测模型与全球急性冠状动脉事件注册(GRACE)评分进行比较,评价模型对AMI患者PCI后预后评估的改善效果。 结果 962例AMI患者中122例(12.7%)患者出现远期主要不良心血管事件。Lasso回归筛选出5个预测变量,包括心电图ST段偏移、糖尿病、左心室射血分数(LVEF)、估算肾小球滤过率(eGFR)、血红蛋白(Hb)。通过多因素Logistic回归分析构建的预测模型的回归方程为:logit(P)=3.596-0.023×X1-0.014×X2-0.036×X3+0.726×X4+1.372×X5(X1表示Hb,X2表示eGFR,X3表示LVEF,X4表示糖尿病,X5表示心电图ST段偏移)。心电图ST段偏移、糖尿病、LVEF、Hb是AMI患者PCI后发生远期主要不良心血管事件的影响因素(P<0.05);心电图ST段偏移、糖尿病、eGFR、Hb是ST段抬高型心肌梗死(STEMI)患者PCI后发生远期主要不良心血管事件的影响因素(P<0.05);心电图ST段偏移、糖尿病、Hb是非ST段抬高型心肌梗死(NSTEMI)患者PCI后发生远期主要不良心血管事件的影响因素(P<0.05)。预测模型预测开发队列与验证队列患者PCI后发生远期主要不良心血管事件的ROC曲线下面积(AUC)分别为0.774〔95%CI(0.710,0.834)〕、0.751〔95%CI(0.686,0.815)〕。AMI、STEMI、NSTEMI患者中NRI分别为0.493〔95%CI(0.303,0.682)〕、0.459〔95%CI(0.195,0.724)〕、0.455〔95%CI(0.181,0.728〕,IDI分别为0.055〔95%CI(0.028,0.081)〕、0.042〔95%CI(0.015,0.070〕、0.069〔95%CI(0.022,0.116)〕。3组患者中预测模型的预测效能均优于GRACE评分(P<0.05)。全研究人群队列分析发现预测模型的评价效能优于GRACE评分〔ΔAUC=0.050,P=0.015;IDI=0.055,95%CI(0.028,0.081),P<0.001;NRI=0.493,95%CI(0.303,0.682),P<0.001)〕。 结论 由心电图ST段偏移、糖尿病、LVEF、eGFR、Hb共5个预测变量构建的预测模型可用于评估AMI患者PCI后远期预后,有助于患者早期风险分层。
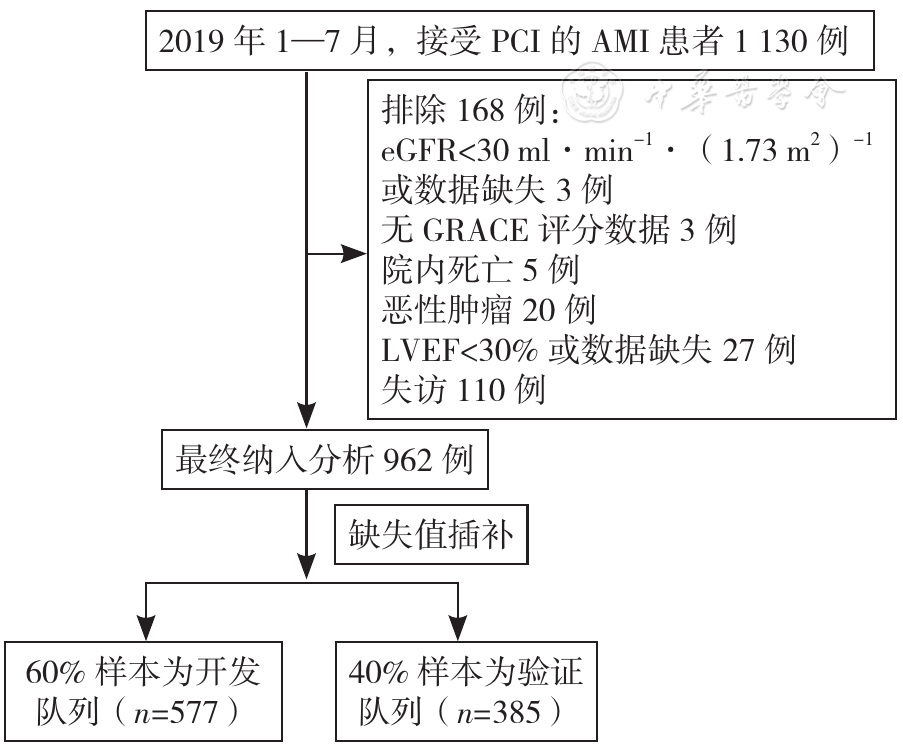
图1 研究样本纳入流程图注:PCI=经皮冠状动脉介入治疗,AMI=急性心肌梗死,eGFR=估算肾小球滤过率,GRACE=全球急性冠状动脉事件注册,LVEF=左心室射血分数
Figure 1 Flow chart of study sample enrollment
| 指标 | 事件组(n=122) | 非事件组(n=840) | 检验统计量值 | P值 | 指标 | 事件组(n=122) | 非事件组(n=840) | 检验统计量值 | P值 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 年龄( | 61.8±10.3 | 57.5±11.2 | -3.991a | <0.001 | 肌酐〔M(Q1,Q3),mg/dl〕 | 0.9(0.8,1.1) | 0.9(0.8,1.0) | -1.344c | 0.178 | |
| 男性〔n(%)〕 | 94(77.1) | 688(81.9) | 1.651b | 0.199 | 心肌酶〔M(Q1,Q3),U/L〕 | 1.4(0.2,10.7) | 1.1(0.2,7.7) | -0.298c | 0.765 | |
| 心电图ST段偏移〔n(%)〕 | 84(68.9) | 307(36.6) | 46.083b | <0.001 | eGFR〔M(Q1,Q3),ml·min-1·(1.73 m2)-1〕 | 91.0(78.6,100.0) | 95.1(87.0,103.2) | 3.464c | 0.001 | |
| 心功能Killip分级≥Ⅱ级〔n(%)〕 | 26(21.3) | 83(9.9) | 13.854b | <0.001 | 尿素〔M(Q1,Q3),mmol/L〕 | 5.9(4.7,7.1) | 5.4(4.5,6.6) | -2.843c | 0.005 | |
| 发病时间〔n(%)〕 | 0.449b | 0.799 | 尿酸〔M(Q1,Q3),mmol/L〕 | 360.0(291.8,401.8) | 346.8(293.4,408.5) | 0.076c | 0.940 | |||
| <6 h | 25(20.5) | 165(19.6) | 白细胞计数〔M(Q1,Q3),×109/L〕 | 8.4(7.0,11.2) | 8.3(6.7,10.3) | -0.965c | 0.335 | |||
| 6~12 h | 16(13.1) | 95(11.3) | Hb〔M(Q1,Q3),g/L〕 | 141.0(127.0,152.0) | 149.0(138.0,158.0) | 4.529c | <0.001 | |||
| >12 h | 81(66.4) | 580(69.1) | NLR〔M(Q1,Q3)〕 | 3.5(2.3,5.3) | 3.2(2.2,5.0) | -0.893c | 0.372 | |||
| 门球时间≤90 min〔n(%)〕 | 27(22.1) | 178(21.2) | 0.056b | 0.813 | PLR〔M(Q1,Q3)〕 | 124.3(98.5,168.0) | 130.1(101.6,179.0) | 0.738c | 0.461 | |
| 术后TIMI分级≤2级〔n(%)〕 | 5(4.1) | 7(0.8) | 9.219b | 0.002 | 红细胞分布宽度〔M(Q1,Q3),%〕 | 13.0(12.4,13.5) | 12.8(12.4,13.2) | -2.983c | 0.003 | |
| 高血压〔n(%)〕 | 85(69.7) | 511(60.8) | 3.531b | 0.060 | 钠〔M(Q1,Q3),mmol/L〕 | 139.8(137.8,141.4) | 139.5(137.5,141.3) | -0.449c | 0.653 | |
| 高脂血症〔n(%)〕 | 112(91.8) | 756(90.2) | 0.302b | 0.583 | 钾〔M(Q1,Q3),mmol/L〕 | 4.1(3.8,4.4) | 4.0(3.8,4.3) | -1.266c | 0.206 | |
| 糖尿病〔n(%)〕 | 58(47.5) | 264(31.4) | 12.419b | <0.001 | 氯〔M(Q1,Q3),mmol/L〕 | 102.0(99.1,103.8) | 101.4(99.0,103.7) | -0.549c | 0.583 | |
| 心房颤动〔n(%)〕 | 6(4.9) | 25(3.0) | 1.288b | 0.256 | 白蛋白〔M(Q1,Q3),g/L〕 | 39.1(36.6,42.2) | 40.7(38.2,43.2) | 3.889c | <0.001 | |
| 缺血性脑卒中〔n(%)〕 | 17(13.9) | 58(6.9) | 7.323b | 0.007 | 超敏C反应蛋白〔M(Q1,Q3),mg/L〕 | 8.0(2.6,25.0) | 5.5(1.9,18.6) | -1.878c | 0.060 | |
| 既往心肌梗死〔n(%)〕 | 19(15.6) | 70(8.3) | 6.652b | 0.010 | 游离三碘甲状腺原氨酸〔M(Q1,Q3),pmol/L〕 | 4.5(4.2,5.0) | 4.7(4.3,5.3) | 2.769c | 0.006 | |
| 既往PCI〔n(%)〕 | 25(20.5) | 85(10.1) | 11.318b | 0.001 | 游离甲状腺素〔M(Q1,Q3),pmol/L〕 | 11.6(10.5,13.7) | 11.9(10.6,13.2) | -0.613c | 0.540 | |
| 收缩压( | 126±18 | 126±20 | -0.017a | 0.986 | 糖化血清白蛋白〔M(Q1,Q3),%〕 | 15.8(14.1,19.6) | 14.5(13.1,17.8) | -3.749c | <0.001 | |
| 心率( | 76±16 | 73±11 | -2.597a | 0.010 | 糖化血红蛋白〔M(Q1,Q3),%〕 | 6.4(5.9,7.9) | 6.0(5.6,7.2) | -3.064c | 0.002 | |
| LVEF〔M(Q1,Q3),%〕 | 56.5(48.0,62.0) | 58.0(52.0,63.0) | 2.818c | 0.005 | 纤维蛋白原〔M(Q1,Q3),g/L〕 | 3.6(3.1,4.1) | 3.4(3.0,4.0) | -1.304c | 0.192 | |
| 左心室舒张末期容积〔M(Q1,Q3),ml〕 | 49.0(46.0,53.0) | 48.0(45.0,51.0) | -1.715c | 0.086 | D-二聚体〔M(Q1,Q3),μg/L〕 | 128.5(76.0,219.0) | 101.0(67.0,163.0) | -2.835c | 0.005 | |
| 左心室收缩末期容积〔M(Q1,Q3),ml〕 | 32.0(29.0,36.0) | 32.0(29.0,36.0) | -1.395c | 0.163 | 纤维蛋白原降解产物〔M(Q1,Q3),mg/L〕 | 0.9(0.6,1.6) | 0.7(0.3,1.2) | -4.225c | <0.001 | |
| GRACE评分〔M(Q1,Q3),分〕 | 139.0(122.0,161.0) | 122.0(105.0,137.0) | -7.055c | <0.001 | B型利钠肽〔M(Q1,Q3),ng/L〕 | 206.0(71.0,320.0) | 112.0(53.0,240.0) | -3.483c | 0.001 | |
表1 事件组与非事件组患者临床资料比较
Table 1 Comparison of clinical data between two groups of AMI patients divided by long-term MACEs prevalence
| 指标 | 事件组(n=122) | 非事件组(n=840) | 检验统计量值 | P值 | 指标 | 事件组(n=122) | 非事件组(n=840) | 检验统计量值 | P值 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 年龄( | 61.8±10.3 | 57.5±11.2 | -3.991a | <0.001 | 肌酐〔M(Q1,Q3),mg/dl〕 | 0.9(0.8,1.1) | 0.9(0.8,1.0) | -1.344c | 0.178 | |
| 男性〔n(%)〕 | 94(77.1) | 688(81.9) | 1.651b | 0.199 | 心肌酶〔M(Q1,Q3),U/L〕 | 1.4(0.2,10.7) | 1.1(0.2,7.7) | -0.298c | 0.765 | |
| 心电图ST段偏移〔n(%)〕 | 84(68.9) | 307(36.6) | 46.083b | <0.001 | eGFR〔M(Q1,Q3),ml·min-1·(1.73 m2)-1〕 | 91.0(78.6,100.0) | 95.1(87.0,103.2) | 3.464c | 0.001 | |
| 心功能Killip分级≥Ⅱ级〔n(%)〕 | 26(21.3) | 83(9.9) | 13.854b | <0.001 | 尿素〔M(Q1,Q3),mmol/L〕 | 5.9(4.7,7.1) | 5.4(4.5,6.6) | -2.843c | 0.005 | |
| 发病时间〔n(%)〕 | 0.449b | 0.799 | 尿酸〔M(Q1,Q3),mmol/L〕 | 360.0(291.8,401.8) | 346.8(293.4,408.5) | 0.076c | 0.940 | |||
| <6 h | 25(20.5) | 165(19.6) | 白细胞计数〔M(Q1,Q3),×109/L〕 | 8.4(7.0,11.2) | 8.3(6.7,10.3) | -0.965c | 0.335 | |||
| 6~12 h | 16(13.1) | 95(11.3) | Hb〔M(Q1,Q3),g/L〕 | 141.0(127.0,152.0) | 149.0(138.0,158.0) | 4.529c | <0.001 | |||
| >12 h | 81(66.4) | 580(69.1) | NLR〔M(Q1,Q3)〕 | 3.5(2.3,5.3) | 3.2(2.2,5.0) | -0.893c | 0.372 | |||
| 门球时间≤90 min〔n(%)〕 | 27(22.1) | 178(21.2) | 0.056b | 0.813 | PLR〔M(Q1,Q3)〕 | 124.3(98.5,168.0) | 130.1(101.6,179.0) | 0.738c | 0.461 | |
| 术后TIMI分级≤2级〔n(%)〕 | 5(4.1) | 7(0.8) | 9.219b | 0.002 | 红细胞分布宽度〔M(Q1,Q3),%〕 | 13.0(12.4,13.5) | 12.8(12.4,13.2) | -2.983c | 0.003 | |
| 高血压〔n(%)〕 | 85(69.7) | 511(60.8) | 3.531b | 0.060 | 钠〔M(Q1,Q3),mmol/L〕 | 139.8(137.8,141.4) | 139.5(137.5,141.3) | -0.449c | 0.653 | |
| 高脂血症〔n(%)〕 | 112(91.8) | 756(90.2) | 0.302b | 0.583 | 钾〔M(Q1,Q3),mmol/L〕 | 4.1(3.8,4.4) | 4.0(3.8,4.3) | -1.266c | 0.206 | |
| 糖尿病〔n(%)〕 | 58(47.5) | 264(31.4) | 12.419b | <0.001 | 氯〔M(Q1,Q3),mmol/L〕 | 102.0(99.1,103.8) | 101.4(99.0,103.7) | -0.549c | 0.583 | |
| 心房颤动〔n(%)〕 | 6(4.9) | 25(3.0) | 1.288b | 0.256 | 白蛋白〔M(Q1,Q3),g/L〕 | 39.1(36.6,42.2) | 40.7(38.2,43.2) | 3.889c | <0.001 | |
| 缺血性脑卒中〔n(%)〕 | 17(13.9) | 58(6.9) | 7.323b | 0.007 | 超敏C反应蛋白〔M(Q1,Q3),mg/L〕 | 8.0(2.6,25.0) | 5.5(1.9,18.6) | -1.878c | 0.060 | |
| 既往心肌梗死〔n(%)〕 | 19(15.6) | 70(8.3) | 6.652b | 0.010 | 游离三碘甲状腺原氨酸〔M(Q1,Q3),pmol/L〕 | 4.5(4.2,5.0) | 4.7(4.3,5.3) | 2.769c | 0.006 | |
| 既往PCI〔n(%)〕 | 25(20.5) | 85(10.1) | 11.318b | 0.001 | 游离甲状腺素〔M(Q1,Q3),pmol/L〕 | 11.6(10.5,13.7) | 11.9(10.6,13.2) | -0.613c | 0.540 | |
| 收缩压( | 126±18 | 126±20 | -0.017a | 0.986 | 糖化血清白蛋白〔M(Q1,Q3),%〕 | 15.8(14.1,19.6) | 14.5(13.1,17.8) | -3.749c | <0.001 | |
| 心率( | 76±16 | 73±11 | -2.597a | 0.010 | 糖化血红蛋白〔M(Q1,Q3),%〕 | 6.4(5.9,7.9) | 6.0(5.6,7.2) | -3.064c | 0.002 | |
| LVEF〔M(Q1,Q3),%〕 | 56.5(48.0,62.0) | 58.0(52.0,63.0) | 2.818c | 0.005 | 纤维蛋白原〔M(Q1,Q3),g/L〕 | 3.6(3.1,4.1) | 3.4(3.0,4.0) | -1.304c | 0.192 | |
| 左心室舒张末期容积〔M(Q1,Q3),ml〕 | 49.0(46.0,53.0) | 48.0(45.0,51.0) | -1.715c | 0.086 | D-二聚体〔M(Q1,Q3),μg/L〕 | 128.5(76.0,219.0) | 101.0(67.0,163.0) | -2.835c | 0.005 | |
| 左心室收缩末期容积〔M(Q1,Q3),ml〕 | 32.0(29.0,36.0) | 32.0(29.0,36.0) | -1.395c | 0.163 | 纤维蛋白原降解产物〔M(Q1,Q3),mg/L〕 | 0.9(0.6,1.6) | 0.7(0.3,1.2) | -4.225c | <0.001 | |
| GRACE评分〔M(Q1,Q3),分〕 | 139.0(122.0,161.0) | 122.0(105.0,137.0) | -7.055c | <0.001 | B型利钠肽〔M(Q1,Q3),ng/L〕 | 206.0(71.0,320.0) | 112.0(53.0,240.0) | -3.483c | 0.001 | |
| 指标 | 开发队列(n=577) | 验证队列(n=385) | 检验统计量值 | P值 | 指标 | 开发队列(n=577) | 验证队列(n=385) | 检验统计量值 | P值 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 年龄( | 58.2±10.9 | 57.8±11.6 | 0.458a | 0.647 | 心肌酶〔M(Q1,Q3),U/L〕 | 1.0(0.2,7.8) | 1.3(0.2,8.2) | -0.842 | 0.400 | |
| 男性〔n(%)〕 | 461(79.9) | 321(83.4) | 1.839b | 0.175 | eGFR〔M(Q1,Q3),ml·min-1·(1.73m2)-1〕 | 94.8(86.1,103.2) | 94.5(86.1,102.4) | 0.797c | 0.425 | |
| 心电图ST段偏移〔n(%)〕 | 230(39.9) | 161(41.8) | 0.367b | 0.545 | 尿素〔M(Q1,Q3),mmol/L〕 | 5.5(4.6,6.7) | 5.5(4.5,6.7) | -0.092c | 0.927 | |
| 心功能Killip分级≥Ⅱ级〔n(%)〕 | 64(11.1) | 45(11.7) | 0.082b | 0.775 | 尿酸〔M(Q1,Q3),mmol/L〕 | 347.5(293.1,404.8) | 346.8(292.9,410.5) | -0.628c | 0.530 | |
| 发病时间〔n(%)〕 | 1.140b | 0.566 | 白细胞计数〔M(Q1,Q3),×109/L〕 | 8.3(6.7,10.4) | 8.4(6.8,10.4) | -0.437c | 0.662 | |||
| <6 h | 112(19.4) | 78(20.3) | Hb〔M(Q1,Q3),g/L〕 | 148.0(137.0,158.0) | 146.0(136.0,157.0) | 0.858c | 0.391 | |||
| 6~12 h | 62(10.8) | 49(12.7) | NLR〔M(Q1,Q3)〕 | 3.3(2.2,5.0) | 3.2(2.2,5.1) | 0.028c | 0.978 | |||
| >12 h | 403(69.8) | 258(67.0) | PLR〔M(Q1,Q3)〕 | 129.3(100.6,176.2) | 128.8(102.7,181.6) | -0.664c | 0.507 | |||
| 门球时间≤90 min〔n(%)〕 | 115(19.9) | 90(23.4) | 1.635b | 0.201 | 红细胞分布宽度〔M(Q1,Q3),%〕 | 12.8(12.4,13.2) | 12.8(12.4,13.4) | -0.618c | 0.537 | |
| 术后TIMI分级≤2级〔n(%)〕 | 9(1.6) | 3(0.8) | 1.142b | 0.285 | 钠〔M(Q1,Q3),mmol/L〕 | 139.5(137.6,141.1) | 139.6(137.5,141.5) | -0.660c | 0.509 | |
| 高血压〔n(%)〕 | 355(61.5) | 241(62.6) | 0.113b | 0.737 | 钾〔M(Q1,Q3),mmol/L〕 | 4.1(3.8,4.3) | 4.0(3.8,4.3) | 0.631c | 0.528 | |
| 高脂血症〔n(%)〕 | 521(90.3) | 349(90.7) | 0.034b | 0.855 | 氯〔M(Q1,Q3),mmol/L〕 | 101.6(99.3,103.7) | 101.4(98.4,103.6) | 1.111c | 0.267 | |
| 糖尿病〔n(%)〕 | 204(35.4) | 118(30.7) | 2.297b | 0.130 | 白蛋白〔M(Q1,Q3),g/L〕 | 40.5(38.0,43.1) | 40.6(38.1,43.1) | -0.117c | 0.907 | |
| 心房颤动〔n(%)〕 | 17(3.0) | 14(3.6) | 0.353b | 0.553 | 超敏C反应蛋白〔M(Q1,Q3),mg/L〕 | 5.2(1.8,18.9) | 6.1(2.3,20.5) | -1.258c | 0.208 | |
| 缺血性脑卒中〔n(%)〕 | 47(8.2) | 28(7.3) | 0.245b | 0.621 | 游离三碘甲状腺原氨酸〔M(Q1,Q3),pmol/L〕 | 4.7(4.3,5.3) | 4.7(4.2,5.2) | 1.149c | 0.251 | |
| 既往心肌梗死〔n(%)〕 | 54(9.4) | 35(9.1) | 0.020b | 0.888 | 游离甲状腺素〔M(Q1,Q3),pmol/L〕 | 11.8(10.4,13.3) | 11.9(10.7,13.2) | -0.925c | 0.355 | |
| 既往PCI〔n(%)〕 | 72(12.5) | 38(9.9) | 1.551b | 0.213 | 糖化血清白蛋白〔M(Q1,Q3),%〕 | 14.9(13.2,18.2) | 14.5(13.2,17.7) | 0.902c | 0.367 | |
| 收缩压( | 126±18 | 125±18 | 1.153a | 0.249 | 糖化血红蛋白〔M(Q1,Q3),%〕 | 6.1(5.7,7.4) | 6.1(5.7,7.2) | 0.301c | 0.763 | |
| 心率( | 73±11 | 74±12 | -1.342a | 0.180 | 纤维蛋白原〔M(Q1,Q3),g/L〕 | 3.5(3.0,4.0) | 3.4(2.6,4.0) | -0.239c | 0.811 | |
| LVEF〔M(Q1,Q3),%〕 | 58.0(52.0,63.0) | 58.0(52.0,63.0) | -0.863c | 0.388 | D-二聚体〔M(Q1,Q3),μg/L〕 | 102.0(66.0,173.0) | 105.0(69.0,171.0) | -0.488c | 0.623 | |
| 左心室舒张末期容积〔M(Q1,Q3),ml〕 | 48.0(45.0,52.0) | 49.0(45.0,52.0) | 0.423c | 0.673 | 纤维蛋白原降解产物〔M(Q1,Q3),mg/L〕 | 0.7(0.4,1.3) | 0.7(0.3,1.2) | 0.353c | 0.724 | |
| 左心室收缩末期容积〔M(Q1,Q3),ml〕 | 32.0(29.0,35.0) | 32.0(29.0,35.0) | -1.395c | 0.262 | B型利钠肽〔M(Q1,Q3),ng/L〕 | 106.0(47.0,255.0) | 127.0(61.0,253.0) | -2.007c | 0.045 | |
| GRACE评分〔M(Q1,Q3),分〕 | 122.0(106.0,139.0) | 123.0(105.0,144.0) | -0.539c | 0.590 | 远期主要不良心血管事件〔n(%)〕 | 69(12.0) | 53(13.8) | 0.682b | 0.409 | |
| 肌酐〔M(Q1,Q3),mg/dl〕 | 0.9(0.7,1.0) | 0.9(0.8,1.0) | -2.347c | 0.019 | ||||||
表2 开发队列和验证队列患者临床资料比较
Table 2 Comparison of basic demographics and laboratory parameters in development and validation sub-cohorts of AMI patients after PCI
| 指标 | 开发队列(n=577) | 验证队列(n=385) | 检验统计量值 | P值 | 指标 | 开发队列(n=577) | 验证队列(n=385) | 检验统计量值 | P值 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 年龄( | 58.2±10.9 | 57.8±11.6 | 0.458a | 0.647 | 心肌酶〔M(Q1,Q3),U/L〕 | 1.0(0.2,7.8) | 1.3(0.2,8.2) | -0.842 | 0.400 | |
| 男性〔n(%)〕 | 461(79.9) | 321(83.4) | 1.839b | 0.175 | eGFR〔M(Q1,Q3),ml·min-1·(1.73m2)-1〕 | 94.8(86.1,103.2) | 94.5(86.1,102.4) | 0.797c | 0.425 | |
| 心电图ST段偏移〔n(%)〕 | 230(39.9) | 161(41.8) | 0.367b | 0.545 | 尿素〔M(Q1,Q3),mmol/L〕 | 5.5(4.6,6.7) | 5.5(4.5,6.7) | -0.092c | 0.927 | |
| 心功能Killip分级≥Ⅱ级〔n(%)〕 | 64(11.1) | 45(11.7) | 0.082b | 0.775 | 尿酸〔M(Q1,Q3),mmol/L〕 | 347.5(293.1,404.8) | 346.8(292.9,410.5) | -0.628c | 0.530 | |
| 发病时间〔n(%)〕 | 1.140b | 0.566 | 白细胞计数〔M(Q1,Q3),×109/L〕 | 8.3(6.7,10.4) | 8.4(6.8,10.4) | -0.437c | 0.662 | |||
| <6 h | 112(19.4) | 78(20.3) | Hb〔M(Q1,Q3),g/L〕 | 148.0(137.0,158.0) | 146.0(136.0,157.0) | 0.858c | 0.391 | |||
| 6~12 h | 62(10.8) | 49(12.7) | NLR〔M(Q1,Q3)〕 | 3.3(2.2,5.0) | 3.2(2.2,5.1) | 0.028c | 0.978 | |||
| >12 h | 403(69.8) | 258(67.0) | PLR〔M(Q1,Q3)〕 | 129.3(100.6,176.2) | 128.8(102.7,181.6) | -0.664c | 0.507 | |||
| 门球时间≤90 min〔n(%)〕 | 115(19.9) | 90(23.4) | 1.635b | 0.201 | 红细胞分布宽度〔M(Q1,Q3),%〕 | 12.8(12.4,13.2) | 12.8(12.4,13.4) | -0.618c | 0.537 | |
| 术后TIMI分级≤2级〔n(%)〕 | 9(1.6) | 3(0.8) | 1.142b | 0.285 | 钠〔M(Q1,Q3),mmol/L〕 | 139.5(137.6,141.1) | 139.6(137.5,141.5) | -0.660c | 0.509 | |
| 高血压〔n(%)〕 | 355(61.5) | 241(62.6) | 0.113b | 0.737 | 钾〔M(Q1,Q3),mmol/L〕 | 4.1(3.8,4.3) | 4.0(3.8,4.3) | 0.631c | 0.528 | |
| 高脂血症〔n(%)〕 | 521(90.3) | 349(90.7) | 0.034b | 0.855 | 氯〔M(Q1,Q3),mmol/L〕 | 101.6(99.3,103.7) | 101.4(98.4,103.6) | 1.111c | 0.267 | |
| 糖尿病〔n(%)〕 | 204(35.4) | 118(30.7) | 2.297b | 0.130 | 白蛋白〔M(Q1,Q3),g/L〕 | 40.5(38.0,43.1) | 40.6(38.1,43.1) | -0.117c | 0.907 | |
| 心房颤动〔n(%)〕 | 17(3.0) | 14(3.6) | 0.353b | 0.553 | 超敏C反应蛋白〔M(Q1,Q3),mg/L〕 | 5.2(1.8,18.9) | 6.1(2.3,20.5) | -1.258c | 0.208 | |
| 缺血性脑卒中〔n(%)〕 | 47(8.2) | 28(7.3) | 0.245b | 0.621 | 游离三碘甲状腺原氨酸〔M(Q1,Q3),pmol/L〕 | 4.7(4.3,5.3) | 4.7(4.2,5.2) | 1.149c | 0.251 | |
| 既往心肌梗死〔n(%)〕 | 54(9.4) | 35(9.1) | 0.020b | 0.888 | 游离甲状腺素〔M(Q1,Q3),pmol/L〕 | 11.8(10.4,13.3) | 11.9(10.7,13.2) | -0.925c | 0.355 | |
| 既往PCI〔n(%)〕 | 72(12.5) | 38(9.9) | 1.551b | 0.213 | 糖化血清白蛋白〔M(Q1,Q3),%〕 | 14.9(13.2,18.2) | 14.5(13.2,17.7) | 0.902c | 0.367 | |
| 收缩压( | 126±18 | 125±18 | 1.153a | 0.249 | 糖化血红蛋白〔M(Q1,Q3),%〕 | 6.1(5.7,7.4) | 6.1(5.7,7.2) | 0.301c | 0.763 | |
| 心率( | 73±11 | 74±12 | -1.342a | 0.180 | 纤维蛋白原〔M(Q1,Q3),g/L〕 | 3.5(3.0,4.0) | 3.4(2.6,4.0) | -0.239c | 0.811 | |
| LVEF〔M(Q1,Q3),%〕 | 58.0(52.0,63.0) | 58.0(52.0,63.0) | -0.863c | 0.388 | D-二聚体〔M(Q1,Q3),μg/L〕 | 102.0(66.0,173.0) | 105.0(69.0,171.0) | -0.488c | 0.623 | |
| 左心室舒张末期容积〔M(Q1,Q3),ml〕 | 48.0(45.0,52.0) | 49.0(45.0,52.0) | 0.423c | 0.673 | 纤维蛋白原降解产物〔M(Q1,Q3),mg/L〕 | 0.7(0.4,1.3) | 0.7(0.3,1.2) | 0.353c | 0.724 | |
| 左心室收缩末期容积〔M(Q1,Q3),ml〕 | 32.0(29.0,35.0) | 32.0(29.0,35.0) | -1.395c | 0.262 | B型利钠肽〔M(Q1,Q3),ng/L〕 | 106.0(47.0,255.0) | 127.0(61.0,253.0) | -2.007c | 0.045 | |
| GRACE评分〔M(Q1,Q3),分〕 | 122.0(106.0,139.0) | 123.0(105.0,144.0) | -0.539c | 0.590 | 远期主要不良心血管事件〔n(%)〕 | 69(12.0) | 53(13.8) | 0.682b | 0.409 | |
| 肌酐〔M(Q1,Q3),mg/dl〕 | 0.9(0.7,1.0) | 0.9(0.8,1.0) | -2.347c | 0.019 | ||||||
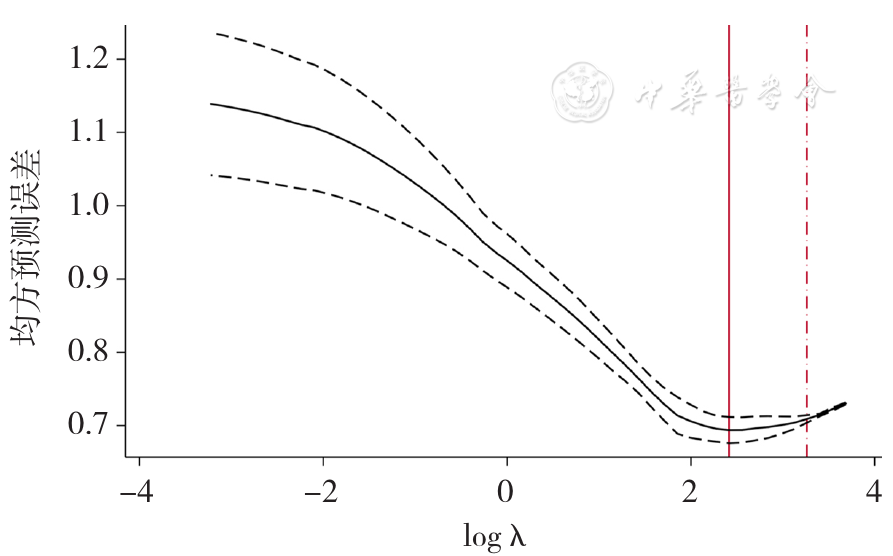
图2 采用Lasso回归进行预测变量的筛选
Figure 2 Selection of potential predictors of long-term MACEs in AMI patients after PCI by Lasso regression

图3 AMI患者PCI后发生远期主要不良心血管事件风险的预测模型列线图注:Hb=血红蛋白
Figure 3 Nomogram in predicting long-term MACEs in AMI patients after PCI
| 预测变量 | β | SE | Waldχ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 心电图ST段偏移 | 1.372 | 0.285 | 23.183 | <0.001 | 3.943 | (2.256,6.892) |
| 糖尿病 | 0.726 | 0.274 | 7.027 | 0.008 | 2.066 | (1.208,3.533) |
| LVEF | -0.036 | 0.015 | 6.083 | 0.014 | 0.964 | (0.937,0.993) |
| eGFR | -0.014 | 0.010 | 2.217 | 0.136 | 0.986 | (0.967,1.005) |
| Hb | -0.023 | 0.009 | 6.518 | 0.011 | 0.978 | (0.961,0.995) |
| 常量 | 3.596 | 1.592 | 5.106 | 0.024 | — | — |
表3 AMI患者PCI后发生远期主要不良心血管事件影响因素的多因素Logistic回归分析
Table 3 Multivariate Logistic regression analysis of the factors associated with the risk of long-term MACEs in patients with AMI after PCI
| 预测变量 | β | SE | Waldχ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 心电图ST段偏移 | 1.372 | 0.285 | 23.183 | <0.001 | 3.943 | (2.256,6.892) |
| 糖尿病 | 0.726 | 0.274 | 7.027 | 0.008 | 2.066 | (1.208,3.533) |
| LVEF | -0.036 | 0.015 | 6.083 | 0.014 | 0.964 | (0.937,0.993) |
| eGFR | -0.014 | 0.010 | 2.217 | 0.136 | 0.986 | (0.967,1.005) |
| Hb | -0.023 | 0.009 | 6.518 | 0.011 | 0.978 | (0.961,0.995) |
| 常量 | 3.596 | 1.592 | 5.106 | 0.024 | — | — |
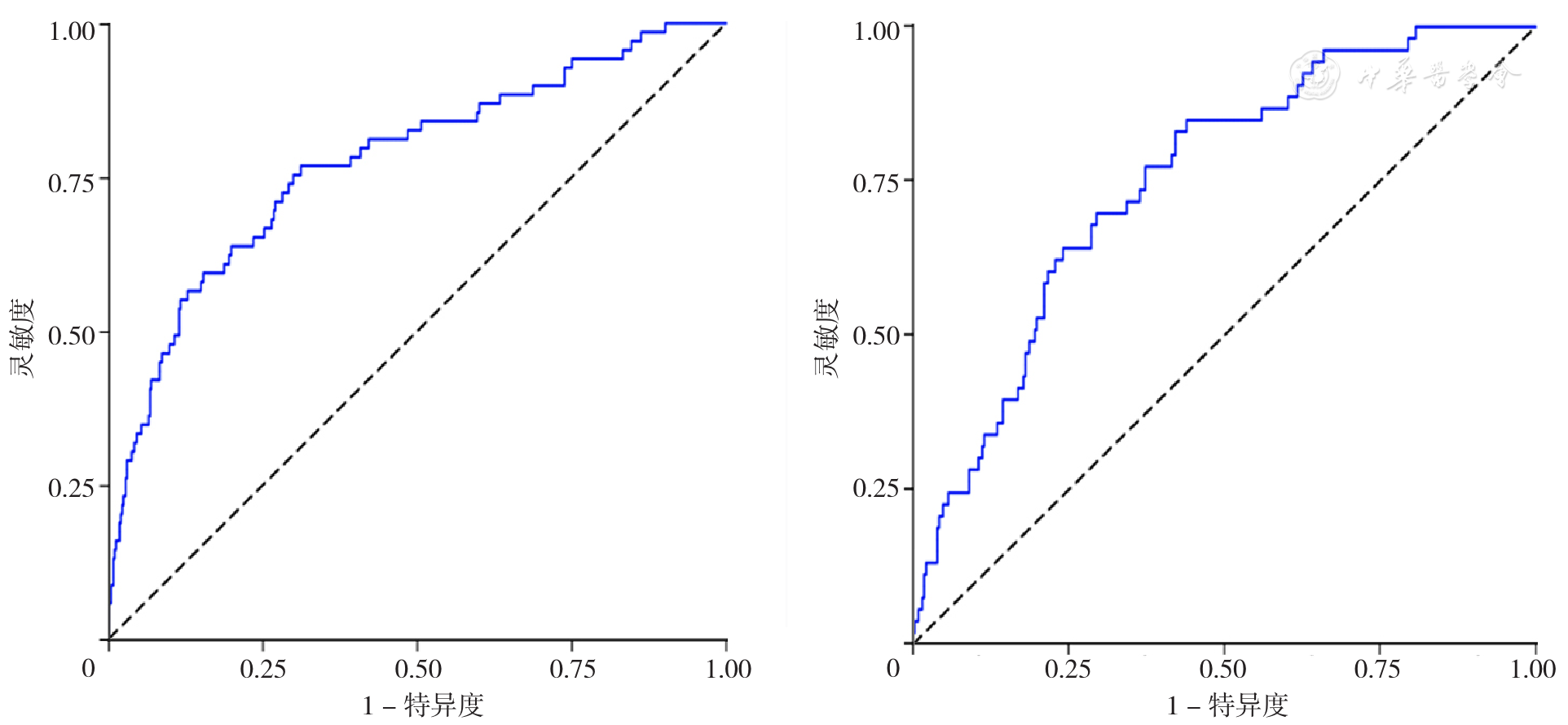
图4 模型预测AMI患者PCI后发生远期主要不良心血管事件的ROC曲线注:A为开发队列,B为验证队列
Figure 4 ROC curve of the model for predicting long-term MACEs in AMI patients after PCI
| 预测变量 | β | SE | Wald χ2值 | P值 | OR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| STEMI组 | |||||||
| 心电图ST段偏移 | 1.227 | 0.293 | 17.481 | <0.001 | 3.410 | (1.919,6.059) | |
| 糖尿病 | 0.666 | 0.290 | 5.291 | 0.021 | 1.947 | (1.104,3.435) | |
| LVEF | -0.023 | 0.016 | 2.037 | 0.153 | 0.977 | (0.947,1.009) | |
| eGFR | -0.021 | 0.010 | 4.558 | 0.033 | 0.979 | (0.960,0.998) | |
| Hb | -0.018 | 0.008 | 4.679 | 0.031 | 0.982 | (0.966,0.998) | |
| 常量 | 3.126 | 1.643 | 3.621 | 0.057 | — | — | |
| NSTEMI组 | |||||||
| 心电图ST段偏移 | 1.368 | 0.321 | 18.142 | <0.001 | 3.928 | (2.093,7.373) | |
| 糖尿病 | 0.643 | 0.300 | 4.583 | 0.032 | 1.902 | (1.056,3.428) | |
| LVEF | -0.033 | 0.019 | 3.131 | 0.077 | 0.968 | (0.933,1.004) | |
| eGFR | -0.009 | 0.009 | 1.001 | 0.317 | 0.991 | (0.973,1.009) | |
| Hb | -0.028 | 0.010 | 7.536 | 0.006 | 0.972 | (0.953,0.992) | |
| 常量 | 3.764 | 1.787 | 4.435 | 0.035 | — | — | |
表4 STEMI组与NSTEMI组患者PCI后发生远期主要不良心血管事件影响因素的多因素Logistic回归分析
Table 4 Multivariate Logistic regression analysis of the factors associated with the risk of long-term MACEs in patients with STEMI or non-STEMI after PCI
| 预测变量 | β | SE | Wald χ2值 | P值 | OR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| STEMI组 | |||||||
| 心电图ST段偏移 | 1.227 | 0.293 | 17.481 | <0.001 | 3.410 | (1.919,6.059) | |
| 糖尿病 | 0.666 | 0.290 | 5.291 | 0.021 | 1.947 | (1.104,3.435) | |
| LVEF | -0.023 | 0.016 | 2.037 | 0.153 | 0.977 | (0.947,1.009) | |
| eGFR | -0.021 | 0.010 | 4.558 | 0.033 | 0.979 | (0.960,0.998) | |
| Hb | -0.018 | 0.008 | 4.679 | 0.031 | 0.982 | (0.966,0.998) | |
| 常量 | 3.126 | 1.643 | 3.621 | 0.057 | — | — | |
| NSTEMI组 | |||||||
| 心电图ST段偏移 | 1.368 | 0.321 | 18.142 | <0.001 | 3.928 | (2.093,7.373) | |
| 糖尿病 | 0.643 | 0.300 | 4.583 | 0.032 | 1.902 | (1.056,3.428) | |
| LVEF | -0.033 | 0.019 | 3.131 | 0.077 | 0.968 | (0.933,1.004) | |
| eGFR | -0.009 | 0.009 | 1.001 | 0.317 | 0.991 | (0.973,1.009) | |
| Hb | -0.028 | 0.010 | 7.536 | 0.006 | 0.972 | (0.953,0.992) | |
| 常量 | 3.764 | 1.787 | 4.435 | 0.035 | — | — | |
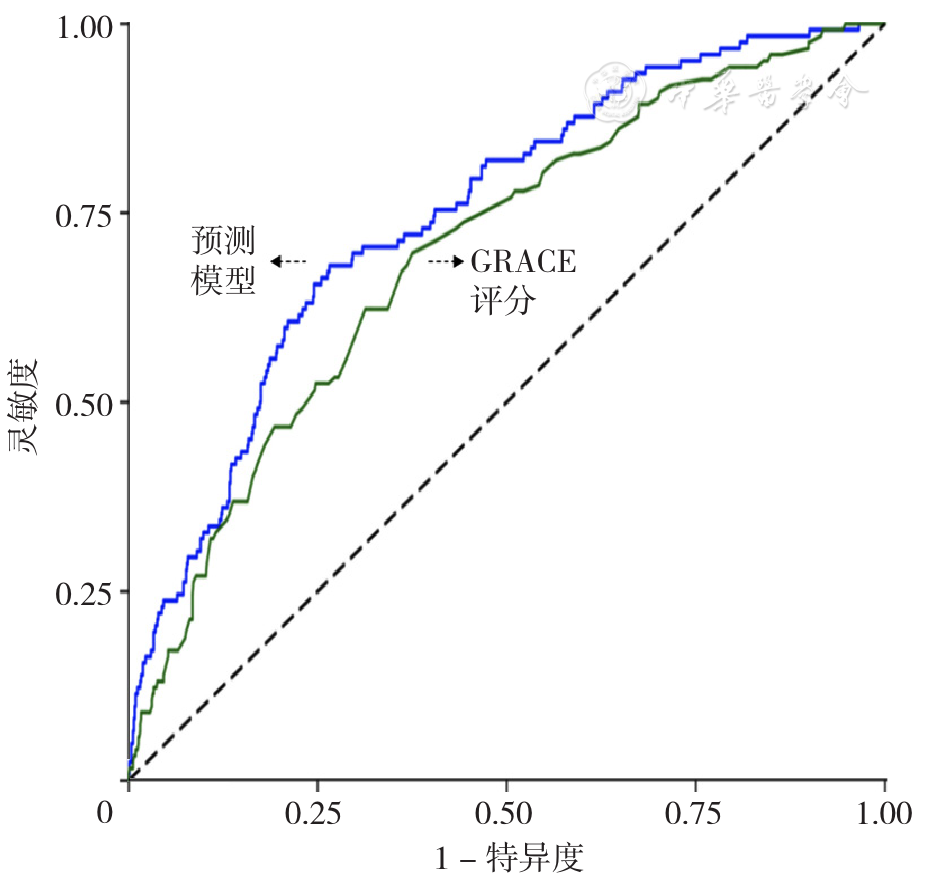
图5 预测模型、GRACE评分预测AMI患者PCI后发生远期主要不良心血管事件的ROC曲线
Figure 5 ROC curve of the model and GRACE score for predicting MACEs in AMI patients after PCI
| 疾病类型 | 例数 | 预测模型C index(95%CI) | GRACE评分C index(95%CI) | ΔC index | NRI(95%CI) | P值 | IDI(95%CI) | P值 |
|---|---|---|---|---|---|---|---|---|
| AMI | 962 | 0.745(0.703,0.788) | 0.696(0.650,0.742) | 0.049 | 0.493(0.303,0.682) | <0.001 | 0.055(0.028,0.081) | <0.001 |
| STEMI | 452 | 0.742(0.686,0.797) | 0.681(0.619,0.742) | 0.061 | 0.459(0.195,0.724) | 0.001 | 0.042(0.015,0.070) | 0.003 |
| NSTEMI | 510 | 0.759(0.694,0.823) | 0.704(0.635,0.773) | 0.055 | 0.455(0.181,0.728) | 0.001 | 0.069(0.022,0.116) | 0.004 |
表5 分别在AMI患者及STEMI、NSTEMI患者中构建的预测模型与GRACE评分效能比较
Table 5 Efficacy evaluation of the predictive model and GRACE score in AMI,STEMI and non-STEMI patients after PCI
| 疾病类型 | 例数 | 预测模型C index(95%CI) | GRACE评分C index(95%CI) | ΔC index | NRI(95%CI) | P值 | IDI(95%CI) | P值 |
|---|---|---|---|---|---|---|---|---|
| AMI | 962 | 0.745(0.703,0.788) | 0.696(0.650,0.742) | 0.049 | 0.493(0.303,0.682) | <0.001 | 0.055(0.028,0.081) | <0.001 |
| STEMI | 452 | 0.742(0.686,0.797) | 0.681(0.619,0.742) | 0.061 | 0.459(0.195,0.724) | 0.001 | 0.042(0.015,0.070) | 0.003 |
| NSTEMI | 510 | 0.759(0.694,0.823) | 0.704(0.635,0.773) | 0.055 | 0.455(0.181,0.728) | 0.001 | 0.069(0.022,0.116) | 0.004 |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
中华医学会心血管病学分会,中华心血管病杂志编辑委员会,中国循环杂志编辑委员会,等. 急性心肌梗死诊断和治疗指南[J]. 中华心血管病杂志,2001(12):9-24. DOI:10.3760/j:issn:0253-3758.2001.12.003.
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
周晓娟,马礼坤,魏艳,等. 急性心肌梗死患者院内心源性休克风险列线图预测模型的构建[J]. 临床心血管病杂志,2021,37(5):421-427. DOI:10.13201/j.issn.1001-1439.2021.05.007.
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [1] | 王秋实, 李虹伟. CHA2DS2-VASc卒中风险评分对冠心病三支血管或左主干病变患者主要不良心血管事件的预测价值研究[J]. 中国全科医学, 2023, 26(33): 4130-4136. |
| [2] | 王瑜, 陈焱, 韩元元, 徐清, 陈胜岳, 吕智博, 卢川, 郑铭鑫, 赵昕. 血小板-淋巴细胞比值可预测老年急性心肌梗死患者住院期间死亡风险[J]. 中国全科医学, 2023, 26(33): 4137-4142. |
| [3] | 张继方, 陈芳, 唐佳雯, 李红亮. 肿瘤出芽及肿瘤浸润淋巴细胞对食管鳞状细胞癌淋巴结转移的预测价值研究[J]. 中国全科医学, 2023, 26(32): 4038-4042. |
| [4] | 温雯, 张凯楠, 陈玉岚, 李瑜, 张向阳. 代谢指数作为预测因子与阻塞性睡眠呼吸暂停的相关性分析[J]. 中国全科医学, 2023, 26(30): 3740-3747. |
| [5] | 马艳艳, 任付先, 王宇, 高登峰. (中性粒细胞+单核细胞)/淋巴细胞比值对心力衰竭患者住院死亡的预测价值研究[J]. 中国全科医学, 2023, 26(30): 3791-3796. |
| [6] | 王珍, 申国旗, 李亚南, 朱英华, 仇航, 郑迪, 徐通达, 李文华. 急性心肌梗死患者行经皮冠状动脉介入治疗术后发生对比剂急性肾损伤风险预测模型的建立与验证研究[J]. 中国全科医学, 2023, 26(29): 3650-3656. |
| [7] | 苗广瑞, 庞硕, 周远航, 段铭烜, 白琳鹏, 张擎阳, 赵晓燕, 董建增. 早期液体平衡和乳酸清除率对体外膜肺氧合辅助治疗急性心肌梗死合并心源性休克患者的短期预后价值研究[J]. 中国全科医学, 2023, 26(27): 3397-3402. |
| [8] | 兰永昊, 科尔沁, 韩蕊, 梅迎晨, 刘巍. 经远端桡动脉入径行经皮冠状动脉介入治疗:优势、劣势、机遇和挑战[J]. 中国全科医学, 2023, 26(27): 3355-3360. |
| [9] | 袁铭培, 林耀望, 贝伟杰, 刘华东, 董少红, 孙鑫. 经远端桡动脉入径逆向开通闭塞桡动脉的可行性:单中心前瞻性研究[J]. 中国全科医学, 2023, 26(27): 3373-3377. |
| [10] | 蔡高军, 师干伟, 李峰, 李文华, 严永敏, 薛社亮, 肖建强, 顾君, 宋艳斌, 张刘燕, 卢伟, 龚春. 如何提高经远端桡动脉入径穿刺成功率、"曲径通幽"?基于两千余病例的经验总结[J]. 中国全科医学, 2023, 26(27): 3361-3365. |
| [11] | 刘明浩, 王攀, 高立建, 徐淑清, 王欢欢, 赵光贤, 陈珏, 乔树宾, 徐波, 袁晋青. 经远端桡动脉入径行二次经皮冠状动脉介入治疗的可行性、安全性和手术时机研究[J]. 中国全科医学, 2023, 26(27): 3366-3372. |
| [12] | 李梓盟, 王荣, 陈帅, 赵彩丽, 王晓聪, 温雅璐, 刘龙. 基于metaPRS与APOEε4优化轻度认知障碍遗传风险统计建模策略的应用研究[J]. 中国全科医学, 2023, 26(25): 3104-3111. |
| [13] | 胡晓飞, 赵平, 曹廷华, 彭兰兰. 腹部脂肪含量及分布对急性胰腺炎及其重症的预测价值研究[J]. 中国全科医学, 2023, 26(21): 2614-2619. |
| [14] | 王丹, 王建辉, 董建秀, 常文红, 秦璐, 刘琪, 陈晨. 基于网络干预对经皮冠状动脉介入治疗术后患者运动行为的影响研究[J]. 中国全科医学, 2023, 26(21): 2603-2608. |
| [15] | 陈焱, 陈胜岳, 韩元元, 吕志博, 徐清, 赵昕. 中性粒细胞/淋巴细胞比值和血小板/淋巴细胞比值对急性心肌梗死患者住院死亡风险的联合预测价值[J]. 中国全科医学, 2023, 26(20): 2482-2487. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










