中国全科医学 ›› 2022, Vol. 25 ›› Issue (09): 1077-1081.DOI: 10.12114/j.issn.1007-9572.2021.02.026
所属专题: 指南/共识最新文章合辑
李健*, 殷延华, 戚建国, 王洲, 任永凤, 王珊珊, 张伟莉, 王效军, 唐坤
Ultrasound-based Thyroid Nodule Malignancy Risk Stratification in Differentiating Benign and Malignant Thyroid Nodules:a Comparative Analysis between the C-TIRADS and ATA Guidelines
LI Jian*,YIN Yanhua,QI Jianguo,WANG Zhou,REN Yongfeng,WANG Shanshan,ZHANG Weili,WANG Xiaojun,TANG Kun
LI Jian*,YIN Yanhua,QI Jianguo,WANG Zhou,REN Yongfeng,WANG Shanshan,ZHANG Weili,WANG Xiaojun,TANG Kun
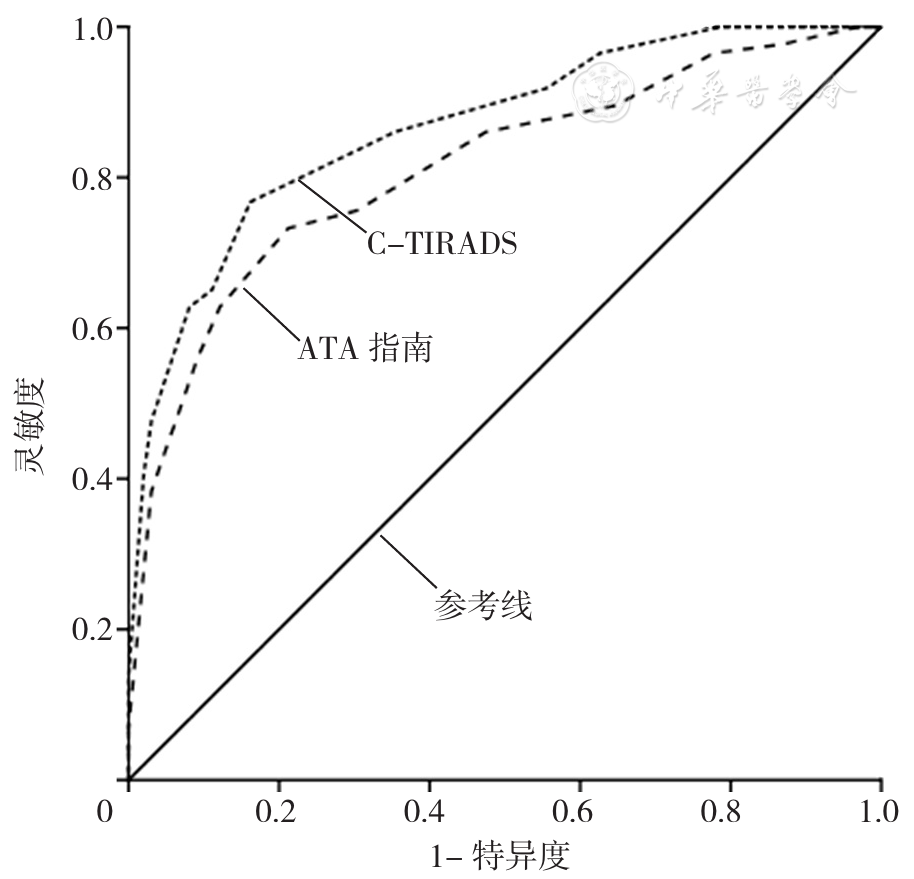
摘要: 背景2020年发布的《甲状腺结节超声恶性危险分层中国指南》(简称C-TIRADS)提出了甲状腺结节超声恶性风险分层方法,但目前关于其对甲状腺结节良恶性鉴别诊断价值的研究较少。目的探讨C-TIRADS与2015年美国甲状腺学会(ATA)发布的《成人甲状腺结节与分化型甲状腺癌诊治指南》(简称ATA指南)中甲状腺结节超声恶性风险分层方法对甲状腺结节良恶性的鉴别诊断价值。方法选取2019年1月至2021年5月在亳州市人民医院住院并行手术治疗和超声检查的甲状腺结节患者336例为研究对象。选取4名具有主治医师以上职称的超声科医师并随机分为A组和B组,每组2名;A组、B组超声科医师分别依据C-TIRADS、ATA指南中甲状腺结节超声恶性风险分层方法对所有患者超声检查结果进行评估。以术中或术后病理检查结果为"金标准",绘制受试者工作特征(ROC)曲线以分析C-TIRADS、ATA指南中甲状腺结节超声恶性风险分层方法对甲状腺结节良恶性的鉴别诊断价值。结果本组336例甲状腺结节患者经术中或术后病理检查共发现367个甲状腺结节,其中良性结节253个、恶性结节114个。A组超声科医师将良性结节评估为5类2个、4c类23个、4b类30个、4a类80个、3类103个、2类15个,将恶性结节评估为5类24个、4c类59个、4b类22个、4a类6个、3类3个、2类0个;B组超声科医师将良性结节评估为高度可疑恶性13个、中度可疑恶性53个、低度可疑恶性47个、极低度可疑恶性118个、良性结节22个,将恶性结节评估为高度可疑恶性76个、中度可疑恶性24个、低度可疑恶性8个、极低度可疑恶性6个、良性结节0个。C-TIRADS、ATA指南中甲状腺结节超声恶性风险分层方法鉴别诊断甲状腺结节良恶性的ROC曲线下面积分别为0.890〔95%CI(0.815,0.918)〕、0.780〔95%CI(0.750,0.876)〕,差异有统计学意义(Z=13.62,P<0.05)。依据C-TIRADS中甲状腺结节超声恶性风险分层方法,4b类、4a类鉴别诊断甲状腺结节良恶性的灵敏度分别为92.11%、97.37%,特异度分别为78.26%、46.64%,准确度分别为82.56%、62.40%,约登指数分别为0.70、0.44;依据ATA指南中甲状腺结节超声恶性风险分层方法,中度可疑恶性、低度可疑恶性鉴别诊断甲状腺结节良恶性的灵敏度分别为87.72%、94.74%,特异度分别为67.98%、44.66%,准确度分别为74.11%、60.22%,约登指数分别为0.56、0.39。结论C-TIRADS中甲状腺结节超声恶性风险分层方法对甲状腺结节良恶性的鉴别诊断价值高于ATA指南中的方法,且最佳截断值为4b类。
中图分类号: