
Chinese General Practice ›› 2023, Vol. 26 ›› Issue (26): 3252-3258.DOI: 10.12114/j.issn.1007-9572.2023.0103
Special Issue: 内分泌代谢性疾病最新文章合辑; 消化系统疾病最新文章合辑
• Original Research·Monographic Research·Type 2 Diabetic • Previous Articles Next Articles
Received:2022-12-02
Revised:2023-03-25
Published:2023-09-15
Online:2023-04-25
Contact:
MA Huijuan
通讯作者:
马慧娟
作者简介:基金资助:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2023.0103
| 组别 | 例数 | 年龄〔M(P25,P75),岁〕 | 性别(男/女) | 病程〔M(P25,P75),年〕 | BMI〔M(P25,P75),kg/m2〕 | 吸烟〔例(%)〕 | 饮酒〔例(%)〕 | 高血压〔例(%)〕 | FBG〔M(P25,P75),mmol/L〕 |
|---|---|---|---|---|---|---|---|---|---|
| 合并MAFLD组 | 734 | 56(46,66) | 458/276 | 7(2,15) | 26.8(25.1,29.3) | 242(33.0) | 210(28.8) | 404(55.0) | 8.64(6.65,11.43) |
| 未合并MAFLD组 | 700 | 62(53,71) | 397/303 | 10(4,18) | 24.2(21.9,26.3) | 189(27.0) | 140(20.0) | 340(48.6) | 7.88(6.14,11.02) |
| Z(χ2)值 | -7.39 | 4.67a | -5.79 | -16.11 | 5.57a | 13.59a | 6.01a | -3.22 | |
| P值 | <0.001 | 0.310 | <0.001 | <0.001 | 0.018 | <0.001 | 0.014 | 0.001 | |
| 组别 | HbA1c〔M(P25,P75),%〕 | UA〔M(P25,P75),μmol/L〕 | Scr〔M(P25,P75),μmol/L〕 | TC〔M(P25,P75),mmol/L〕 | TG〔M(P25,P75),mmol/L〕 | HDL-C〔M(P25,P75),mmol/L〕 | LDL-C〔M(P25,P75),mmol/L〕 | ||
| 合并MAFLD组 | 8.70(7.50,10.48) | 317.30(261.50,380.30) | 72.40(64.50,82.70) | 4.88(4.01,5.63) | 1.75(1.23,2.64) | 0.98(0.85,1.17) | 3.14(2.57,3.70) | ||
| 未合并MAFLD组 | 8.50(7.10,10.60) | 288.10(228.60,341.65) | 71.20(62.90,81.70) | 4.49(3.77,5.30) | 1.18(0.87,1.73) | 1.06(0.89,1.26) | 2.91(2.32,3.50) | ||
| Z(χ2)值 | -1.89 | -6.79 | -1.15 | -4.49 | -11.98 | -4.91 | -4.37 | ||
| P值 | 0.590 | <0.001 | 0.249 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| 组别 | AST〔M(P25,P75),U/L〕 | ALT〔M(P25,P75),U/L〕 | GGT〔M(P25,P75),U/L〕 | BA〔M(P25,P75),μmol/L〕 | ALB〔M(P25,P75),g/L〕 | eGDR〔M(P25,P75)〕 | |||
| 合并MAFLD组 | 19.90(16.15,26.15) | 20.80(14.95,33.70) | 28.80(19.53,44.88) | 3.06(2.06,4.82) | 41.40(38.52,43.80) | 5.50(4.12,7.30) | |||
| 未合并MAFLD组 | 18.10(14.60,22.50) | 15.80(11.85,22.25) | 21.00(14.73,30.38) | 2.94(1.83,4.90) | 39.30(36.68,42.60) | 6.51(5.12,8.22) | |||
| Z(χ2)值 | -5.49 | -9.61 | -9.63 | -0.84 | -7.80 | -7.63 | |||
| P值 | <0.001 | <0.001 | <0.001 | 0.401 | <0.001 | <0.001 |
Table 1 Comparison of baseline data between patients with and without MAFLD
| 组别 | 例数 | 年龄〔M(P25,P75),岁〕 | 性别(男/女) | 病程〔M(P25,P75),年〕 | BMI〔M(P25,P75),kg/m2〕 | 吸烟〔例(%)〕 | 饮酒〔例(%)〕 | 高血压〔例(%)〕 | FBG〔M(P25,P75),mmol/L〕 |
|---|---|---|---|---|---|---|---|---|---|
| 合并MAFLD组 | 734 | 56(46,66) | 458/276 | 7(2,15) | 26.8(25.1,29.3) | 242(33.0) | 210(28.8) | 404(55.0) | 8.64(6.65,11.43) |
| 未合并MAFLD组 | 700 | 62(53,71) | 397/303 | 10(4,18) | 24.2(21.9,26.3) | 189(27.0) | 140(20.0) | 340(48.6) | 7.88(6.14,11.02) |
| Z(χ2)值 | -7.39 | 4.67a | -5.79 | -16.11 | 5.57a | 13.59a | 6.01a | -3.22 | |
| P值 | <0.001 | 0.310 | <0.001 | <0.001 | 0.018 | <0.001 | 0.014 | 0.001 | |
| 组别 | HbA1c〔M(P25,P75),%〕 | UA〔M(P25,P75),μmol/L〕 | Scr〔M(P25,P75),μmol/L〕 | TC〔M(P25,P75),mmol/L〕 | TG〔M(P25,P75),mmol/L〕 | HDL-C〔M(P25,P75),mmol/L〕 | LDL-C〔M(P25,P75),mmol/L〕 | ||
| 合并MAFLD组 | 8.70(7.50,10.48) | 317.30(261.50,380.30) | 72.40(64.50,82.70) | 4.88(4.01,5.63) | 1.75(1.23,2.64) | 0.98(0.85,1.17) | 3.14(2.57,3.70) | ||
| 未合并MAFLD组 | 8.50(7.10,10.60) | 288.10(228.60,341.65) | 71.20(62.90,81.70) | 4.49(3.77,5.30) | 1.18(0.87,1.73) | 1.06(0.89,1.26) | 2.91(2.32,3.50) | ||
| Z(χ2)值 | -1.89 | -6.79 | -1.15 | -4.49 | -11.98 | -4.91 | -4.37 | ||
| P值 | 0.590 | <0.001 | 0.249 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| 组别 | AST〔M(P25,P75),U/L〕 | ALT〔M(P25,P75),U/L〕 | GGT〔M(P25,P75),U/L〕 | BA〔M(P25,P75),μmol/L〕 | ALB〔M(P25,P75),g/L〕 | eGDR〔M(P25,P75)〕 | |||
| 合并MAFLD组 | 19.90(16.15,26.15) | 20.80(14.95,33.70) | 28.80(19.53,44.88) | 3.06(2.06,4.82) | 41.40(38.52,43.80) | 5.50(4.12,7.30) | |||
| 未合并MAFLD组 | 18.10(14.60,22.50) | 15.80(11.85,22.25) | 21.00(14.73,30.38) | 2.94(1.83,4.90) | 39.30(36.68,42.60) | 6.51(5.12,8.22) | |||
| Z(χ2)值 | -5.49 | -9.61 | -9.63 | -0.84 | -7.80 | -7.63 | |||
| P值 | <0.001 | <0.001 | <0.001 | 0.401 | <0.001 | <0.001 |
| 组别 | 例数 | 年龄〔M(P25,P75),岁〕 | 性别(男/女) | 病程〔M(P25,P75),年〕 | 合并MAFLD〔例(%)〕 | BMI〔M(P25,P75),kg/m2〕 | 吸烟〔例(%)〕 | 饮酒〔例(%)〕 | 高血压〔例(%)〕 |
|---|---|---|---|---|---|---|---|---|---|
| T1组 | 477 | 60(49,69) | 272/205 | 10(3,18) | 311(65.1) | 27.3(25.4,30.2) | 165(34.5) | 108(22.7) | 429(89.9) |
| T2组 | 478 | 60(49,70) | 298/180 | 9(3,15) | 233(48.9) | 25.3(23.4,27.0)a | 171(35.8) | 137(28.8) | 288(60.3) |
| T3组 | 479 | 55(47,64)ab | 303/176 | 8(3,14) | 202(42.2) | 24.2(22.2,26.5)ab | 146(30.8) | 116(24.5) | 23(4.8) |
| H(χ2)值 | 20.36 | 4.27c | 2.68 | 48.26c | 213.15 | 2.52c | 4.17c | 648.66c | |
| P值 | <0.001 | 0.118 | 0.262 | <0.001 | <0.001 | 0.286 | 0.125 | <0.001 | |
| 组别 | FBG〔M(P25,P75),mmol/L〕 | HbA1c〔M(P25,P75),%〕 | UA〔M(P25,P75),μmol/L〕 | Scr〔M(P25,P75),μmol/L〕 | TC〔M(P25,P75),mmol/L〕 | TG〔M(P25,P75),mmol/L〕 | |||
| T1组 | 9.70(7.17,12.21) | 9.80(8.60,11.20) | 314.35(249.15,382.38) | 73.25(64.70,85.43) | 4.73(3.89,5.67) | 1.65(1.13,2.46) | |||
| T2组 | 7.94(6.12,11.44)a | 8.20(6.90,11.00)a | 303.30(246.10,365.60) | 73.20(64.50,83.15) | 4.69(3.89,5.52) | 1.41(1.03,2.25)a | |||
| T3组 | 7.57(6.17,9.57)ab | 7.90(6.70,9.10)ab | 291.10(237.13,343.95)a | 69.60(61.98,77.78)ab | 4.69(3.96,5.43) | 1.38(0.88,2.03)ab | |||
| H(χ2)值 | 59.51 | 210.07 | 12.72 | 24.38 | 0.39 | 28.99 | |||
| P值 | <0.001 | <0.001 | 0.002 | <0.001 | 0.823 | <0.001 | |||
| 组别 | HDL-C〔M(P25,P75),mmol/L〕 | LDL-C〔M(P25,P75),mmol/L〕 | AST〔M(P25,P75),U/L〕 | ALT〔M(P25,P75),U/L〕 | GGT〔M(P25,P75),U/L〕 | BA〔M(P25,P75),μmol/L〕 | ALB〔M(P25,P75),g/L〕 | ||
| T1组 | 0.98(0.84,1.17) | 3.05(2.46,3.71) | 19.00(15.30,24.10) | 18.70(13.65,28.85) | 25.90(18.45,41.10) | 3.08(2.02,4.85) | 40.10(37.40,42.70) | ||
| T2组 | 1.02(0.86,1.21) | 3.06(2.47,3.64) | 19.30(15.63,23.60) | 17.85(13.50,26.00) | 24.60(17.70,37.48) | 2.97(1.92,4.95) | 40.90(37.60,43.10) | ||
| T3组 | 1.07(0.91,1.25)ab | 3.00(2.49,3.58) | 19.00(15.60,24.48) | 18.45(13.33,26.88) | 23.15(15.98,35.88)a | 3.00(1.90,4.80) | 41.10(38.70,43.90)ab | ||
| H(χ2)值 | 19.98 | 0.40 | 0.39 | 2.79 | 7.39 | 0.08 | 21.57 | ||
| P值 | <0.001 | 0.819 | 0.823 | 0.248 | 0.025 | 0.961 | <0.001 |
Table 2 Comparison of baseline data of subjects among groups with different eGDR levels
| 组别 | 例数 | 年龄〔M(P25,P75),岁〕 | 性别(男/女) | 病程〔M(P25,P75),年〕 | 合并MAFLD〔例(%)〕 | BMI〔M(P25,P75),kg/m2〕 | 吸烟〔例(%)〕 | 饮酒〔例(%)〕 | 高血压〔例(%)〕 |
|---|---|---|---|---|---|---|---|---|---|
| T1组 | 477 | 60(49,69) | 272/205 | 10(3,18) | 311(65.1) | 27.3(25.4,30.2) | 165(34.5) | 108(22.7) | 429(89.9) |
| T2组 | 478 | 60(49,70) | 298/180 | 9(3,15) | 233(48.9) | 25.3(23.4,27.0)a | 171(35.8) | 137(28.8) | 288(60.3) |
| T3组 | 479 | 55(47,64)ab | 303/176 | 8(3,14) | 202(42.2) | 24.2(22.2,26.5)ab | 146(30.8) | 116(24.5) | 23(4.8) |
| H(χ2)值 | 20.36 | 4.27c | 2.68 | 48.26c | 213.15 | 2.52c | 4.17c | 648.66c | |
| P值 | <0.001 | 0.118 | 0.262 | <0.001 | <0.001 | 0.286 | 0.125 | <0.001 | |
| 组别 | FBG〔M(P25,P75),mmol/L〕 | HbA1c〔M(P25,P75),%〕 | UA〔M(P25,P75),μmol/L〕 | Scr〔M(P25,P75),μmol/L〕 | TC〔M(P25,P75),mmol/L〕 | TG〔M(P25,P75),mmol/L〕 | |||
| T1组 | 9.70(7.17,12.21) | 9.80(8.60,11.20) | 314.35(249.15,382.38) | 73.25(64.70,85.43) | 4.73(3.89,5.67) | 1.65(1.13,2.46) | |||
| T2组 | 7.94(6.12,11.44)a | 8.20(6.90,11.00)a | 303.30(246.10,365.60) | 73.20(64.50,83.15) | 4.69(3.89,5.52) | 1.41(1.03,2.25)a | |||
| T3组 | 7.57(6.17,9.57)ab | 7.90(6.70,9.10)ab | 291.10(237.13,343.95)a | 69.60(61.98,77.78)ab | 4.69(3.96,5.43) | 1.38(0.88,2.03)ab | |||
| H(χ2)值 | 59.51 | 210.07 | 12.72 | 24.38 | 0.39 | 28.99 | |||
| P值 | <0.001 | <0.001 | 0.002 | <0.001 | 0.823 | <0.001 | |||
| 组别 | HDL-C〔M(P25,P75),mmol/L〕 | LDL-C〔M(P25,P75),mmol/L〕 | AST〔M(P25,P75),U/L〕 | ALT〔M(P25,P75),U/L〕 | GGT〔M(P25,P75),U/L〕 | BA〔M(P25,P75),μmol/L〕 | ALB〔M(P25,P75),g/L〕 | ||
| T1组 | 0.98(0.84,1.17) | 3.05(2.46,3.71) | 19.00(15.30,24.10) | 18.70(13.65,28.85) | 25.90(18.45,41.10) | 3.08(2.02,4.85) | 40.10(37.40,42.70) | ||
| T2组 | 1.02(0.86,1.21) | 3.06(2.47,3.64) | 19.30(15.63,23.60) | 17.85(13.50,26.00) | 24.60(17.70,37.48) | 2.97(1.92,4.95) | 40.90(37.60,43.10) | ||
| T3组 | 1.07(0.91,1.25)ab | 3.00(2.49,3.58) | 19.00(15.60,24.48) | 18.45(13.33,26.88) | 23.15(15.98,35.88)a | 3.00(1.90,4.80) | 41.10(38.70,43.90)ab | ||
| H(χ2)值 | 19.98 | 0.40 | 0.39 | 2.79 | 7.39 | 0.08 | 21.57 | ||
| P值 | <0.001 | 0.819 | 0.823 | 0.248 | 0.025 | 0.961 | <0.001 |
| 项目 | 合并MAFLD组 | 未合并MAFLD组 | 项目 | 合并MAFLD组 | 未合并MAFLD组 |
|---|---|---|---|---|---|
| 年龄 | -0.096a | -0.159a | HDL-C | 0.068 | 0.194a |
| 病程 | -0.004 | -0.119a | LDL-C | -0.019 | 0.012 |
| FBG | -0.224a | -0.250a | AST | -0.038 | 0.117a |
| UA | -0.065 | -0.027 | ALT | -0.032 | 0.053 |
| Scr | -0.056 | -0.145a | GGT | -0.044 | 0.080a |
| TC | -0.017 | 0.039 | BA | -0.051 | 0.028 |
| TG | -0.064 | -0.179a | ALB | -0.188a | -0.236a |
Table 3 Correlation analysis between eGDR and baseline data
| 项目 | 合并MAFLD组 | 未合并MAFLD组 | 项目 | 合并MAFLD组 | 未合并MAFLD组 |
|---|---|---|---|---|---|
| 年龄 | -0.096a | -0.159a | HDL-C | 0.068 | 0.194a |
| 病程 | -0.004 | -0.119a | LDL-C | -0.019 | 0.012 |
| FBG | -0.224a | -0.250a | AST | -0.038 | 0.117a |
| UA | -0.065 | -0.027 | ALT | -0.032 | 0.053 |
| Scr | -0.056 | -0.145a | GGT | -0.044 | 0.080a |
| TC | -0.017 | 0.039 | BA | -0.051 | 0.028 |
| TG | -0.064 | -0.179a | ALB | -0.188a | -0.236a |
| 变量 | β | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| 年龄 | -0.026 | 0.004 | 50.038 | 0.974(0.967,0.981) | <0.001 |
| 性别 | -0.233 | 0.108 | 4.664 | 0.792(0.641,0.979) | 0.031 |
| 病程 | <0.001 | <0.001 | 0.401 | 1.000(0.999,1.001) | 0.527 |
| 吸烟 | 0.278 | 0.118 | 5.553 | 1.320(1.048,1.663) | 0.018 |
| 饮酒 | 0.477 | 0.130 | 13.469 | 1.611(1.249,2.078) | <0.001 |
| FBG | <0.001 | <0.001 | 0.404 | 1.000(0.999,1.001) | 0.525 |
| UA | 0.004 | 0.001 | 42.755 | 1.004(1.003,1.005) | <0.001 |
| TC | -0.001 | 0.010 | 0.006 | 0.999(0.980,1.019) | 0.941 |
| TG | 0.073 | 0.026 | 7.506 | 1.075(1.021,1.132) | 0.006 |
| HDL-C | -0.608 | 0.187 | 10.537 | 0.545(0.377,0.786) | 0.001 |
| LDL-C | 0.194 | 0.059 | 10.858 | 1.214(1.082,1.362) | 0.001 |
| AST. | 0.021 | 0.005 | 18.338 | 1.021(1.011,1.030) | <0.001 |
| ALT | 0.028 | 0.004 | 47.739 | 1.029(1.020,1.037) | <0.001 |
| GGT | 0.005 | 0.001 | 11.730 | 1.005(1.002,1.008) | 0.001 |
| BA | -0.021 | 0.010 | 4.241 | 0.979(0.959,0.999) | 0.039 |
| ALB | 0.106 | 0.013 | 62.552 | 1.112(1.083,1.142) | <0.001 |
| eGDR | -0.206 | 0.027 | 59.131 | 0.814(0.772,0.858) | <0.001 |
Table 4 Univariate Logistic regression analysis of influencing factors for MAFLD in T2DM patients
| 变量 | β | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| 年龄 | -0.026 | 0.004 | 50.038 | 0.974(0.967,0.981) | <0.001 |
| 性别 | -0.233 | 0.108 | 4.664 | 0.792(0.641,0.979) | 0.031 |
| 病程 | <0.001 | <0.001 | 0.401 | 1.000(0.999,1.001) | 0.527 |
| 吸烟 | 0.278 | 0.118 | 5.553 | 1.320(1.048,1.663) | 0.018 |
| 饮酒 | 0.477 | 0.130 | 13.469 | 1.611(1.249,2.078) | <0.001 |
| FBG | <0.001 | <0.001 | 0.404 | 1.000(0.999,1.001) | 0.525 |
| UA | 0.004 | 0.001 | 42.755 | 1.004(1.003,1.005) | <0.001 |
| TC | -0.001 | 0.010 | 0.006 | 0.999(0.980,1.019) | 0.941 |
| TG | 0.073 | 0.026 | 7.506 | 1.075(1.021,1.132) | 0.006 |
| HDL-C | -0.608 | 0.187 | 10.537 | 0.545(0.377,0.786) | 0.001 |
| LDL-C | 0.194 | 0.059 | 10.858 | 1.214(1.082,1.362) | 0.001 |
| AST. | 0.021 | 0.005 | 18.338 | 1.021(1.011,1.030) | <0.001 |
| ALT | 0.028 | 0.004 | 47.739 | 1.029(1.020,1.037) | <0.001 |
| GGT | 0.005 | 0.001 | 11.730 | 1.005(1.002,1.008) | 0.001 |
| BA | -0.021 | 0.010 | 4.241 | 0.979(0.959,0.999) | 0.039 |
| ALB | 0.106 | 0.013 | 62.552 | 1.112(1.083,1.142) | <0.001 |
| eGDR | -0.206 | 0.027 | 59.131 | 0.814(0.772,0.858) | <0.001 |
| 变量 | 模型1 | 模型2 | 模型3 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2值 | OR(95%CI) | P值 | β | SE | Wald χ2值 | OR(95%CI) | P值 | β | SE | Wald χ2值 | OR(95%CI) | P值 | |
| eGDR | -0.247 | 0.033 | 54.322 | 0.781(0.732,0.834) | <0.001 | -0.244 | 0.032 | 60.129 | 0.783(0.736,0.833) | <0.001 | -0.206 | 0.027 | 59.131 | 0.814(0.772,0.858) | <0.001 |
| eGDR分组(以T3组为参照) | |||||||||||||||
| T1组 | 0.351 | 0.158 | 4.957 | 1.420(1.043,1.934) | 0.026 | 0.381 | 0.151 | 6.328 | 1.464(1.088,1.969) | 0.012 | 0.270 | 0.136 | 3.916 | 1.31(1.003,1.712) | 0.048 |
| T2组 | 1.076 | 0.169 | 40.448 | 2.934(2.106,4.089) | <0.001 | 1.090 | 0.160 | 46.324 | 2.973(2.172,4.068) | <0.001 | 0.938 | 0.14 | 44.935 | 2.554(1.941,3.359) | <0.001 |
Table 5 Multivariate Logistic regression analysis of eGDR and its grouping for T2DM with MAFLD
| 变量 | 模型1 | 模型2 | 模型3 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2值 | OR(95%CI) | P值 | β | SE | Wald χ2值 | OR(95%CI) | P值 | β | SE | Wald χ2值 | OR(95%CI) | P值 | |
| eGDR | -0.247 | 0.033 | 54.322 | 0.781(0.732,0.834) | <0.001 | -0.244 | 0.032 | 60.129 | 0.783(0.736,0.833) | <0.001 | -0.206 | 0.027 | 59.131 | 0.814(0.772,0.858) | <0.001 |
| eGDR分组(以T3组为参照) | |||||||||||||||
| T1组 | 0.351 | 0.158 | 4.957 | 1.420(1.043,1.934) | 0.026 | 0.381 | 0.151 | 6.328 | 1.464(1.088,1.969) | 0.012 | 0.270 | 0.136 | 3.916 | 1.31(1.003,1.712) | 0.048 |
| T2组 | 1.076 | 0.169 | 40.448 | 2.934(2.106,4.089) | <0.001 | 1.090 | 0.160 | 46.324 | 2.973(2.172,4.068) | <0.001 | 0.938 | 0.14 | 44.935 | 2.554(1.941,3.359) | <0.001 |
| 变量 | β | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| 性别 | |||||
| 男性 | 1.000 | 0.220 | 20.740 | 2.719(1.768,4.183) | <0.001 |
| 女性 | 1.168 | 0.281 | 17.246 | 3.215(1.853,5.580) | <0.001 |
| 年龄 | |||||
| >65岁 | 1.140 | 0.322 | 12.496 | 3.125(1.662,5.879) | <0.001 |
| ≤65岁 | 1.065 | 0.206 | 26.850 | 2.900(1.939,4.339) | <0.001 |
| HbA1c | |||||
| ≤9% | 1.168 | 0.254 | 21.089 | 3.108(1.896,5.094) | <0.001 |
| >9% | 1.297 | 0.284 | 20.814 | 3.657(2.095,6.383) | <0.001 |
| BMI | |||||
| ≤24 kg/m2 | 0.744 | 0.444 | 2.809 | 2.104(0.882,5.024) | 0.904 |
| >24 kg/m2 | 0.688 | 0.204 | 11.315 | 1.989(1.332,2.969) | 0.001 |
| GGT | |||||
| ≤31.5 U/L | 0.886 | 0.209 | 17.934 | 2.427(1.610,3.658) | <0.001 |
| >31.5 U/L | 1.309 | 0.319 | 16.806 | 3.702(1.980,6.921) | <0.001 |
| 高血压 | |||||
| 有 | 2.252 | 0.671 | 11.251 | 9.509(2.550,35.455) | 0.001 |
| 无 | 0.729 | 0.442 | 2.718 | 2.073(0.871,4.933) | 0.099 |
Table 6 Subgroup analysis of eGDR and MAFLD with T2DM
| 变量 | β | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| 性别 | |||||
| 男性 | 1.000 | 0.220 | 20.740 | 2.719(1.768,4.183) | <0.001 |
| 女性 | 1.168 | 0.281 | 17.246 | 3.215(1.853,5.580) | <0.001 |
| 年龄 | |||||
| >65岁 | 1.140 | 0.322 | 12.496 | 3.125(1.662,5.879) | <0.001 |
| ≤65岁 | 1.065 | 0.206 | 26.850 | 2.900(1.939,4.339) | <0.001 |
| HbA1c | |||||
| ≤9% | 1.168 | 0.254 | 21.089 | 3.108(1.896,5.094) | <0.001 |
| >9% | 1.297 | 0.284 | 20.814 | 3.657(2.095,6.383) | <0.001 |
| BMI | |||||
| ≤24 kg/m2 | 0.744 | 0.444 | 2.809 | 2.104(0.882,5.024) | 0.904 |
| >24 kg/m2 | 0.688 | 0.204 | 11.315 | 1.989(1.332,2.969) | 0.001 |
| GGT | |||||
| ≤31.5 U/L | 0.886 | 0.209 | 17.934 | 2.427(1.610,3.658) | <0.001 |
| >31.5 U/L | 1.309 | 0.319 | 16.806 | 3.702(1.980,6.921) | <0.001 |
| 高血压 | |||||
| 有 | 2.252 | 0.671 | 11.251 | 9.509(2.550,35.455) | 0.001 |
| 无 | 0.729 | 0.442 | 2.718 | 2.073(0.871,4.933) | 0.099 |
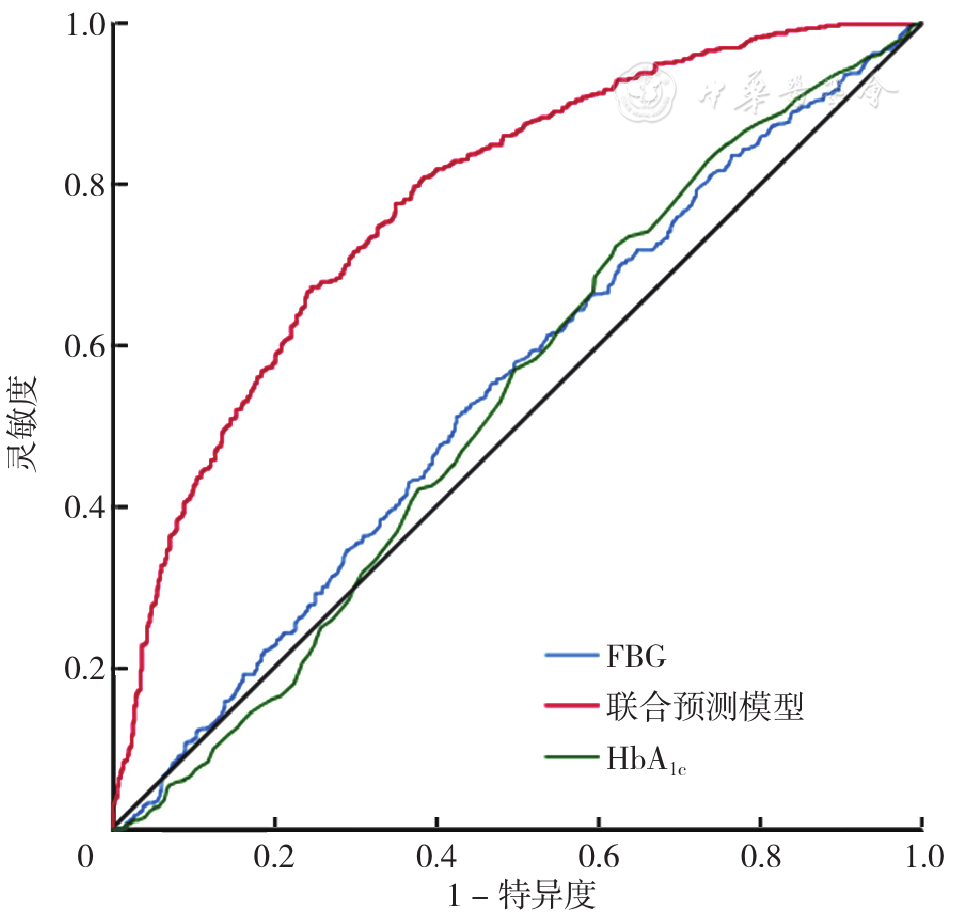
Figure 1 ROC curve of combined prediction model,FBG and HbA1c to predict MAFLD in T2DM
| 项目 | 最佳截断值 | AUC(95%CI) | 灵敏度(%) | 特异度(%) |
|---|---|---|---|---|
| FBG | 8.495 mmol/L | 0.550(0.520,0.581) | 52.5 | 57.2 |
| 联合预测模型 | 0.559 | 0.743(0.715,0.771) | 59.3 | 77.3 |
| HbA1c | 7.750% | 0.530(0.499,0.561) | 71.2 | 38.9 |
Table 7 Predictive value of combined prediction model,FBG and HbA1c for MAFLD in T2DM
| 项目 | 最佳截断值 | AUC(95%CI) | 灵敏度(%) | 特异度(%) |
|---|---|---|---|---|
| FBG | 8.495 mmol/L | 0.550(0.520,0.581) | 52.5 | 57.2 |
| 联合预测模型 | 0.559 | 0.743(0.715,0.771) | 59.3 | 77.3 |
| HbA1c | 7.750% | 0.530(0.499,0.561) | 71.2 | 38.9 |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
中华医学会肝病学分会脂肪肝和酒精性肝病学组. 非酒精性脂肪性肝病诊疗指南(2010年修订版)[J]. 中华肝脏病杂志. 2010,18(3):163-166. DOI:10.3760/cma.j.issn.1007-3418.2010.03.002.
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||