
Chinese General Practice ›› 2023, Vol. 26 ›› Issue (18): 2227-2231.DOI: 10.12114/j.issn.1007-9572.2022.0873
Special Issue: 内分泌代谢性疾病最新文章合辑; 泌尿系统疾病最新文章合辑; 老年问题最新文章合辑
• Original Research • Previous Articles Next Articles
Received:2022-12-03
Revised:2022-12-25
Published:2023-06-20
Online:2023-01-12
Contact:
ZHAO Lizhen
通讯作者:
赵丽珍
作者简介:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2022.0873
| 组别 | 例数 | 性别〔n(%)〕 | 年龄(岁) | BMI (kg/m2) | T2DM病程(年) | 吸烟史〔n(%)〕 | 高血压病史〔n(%)〕 | FPG (mmol/L) | |
|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | ||||||||
| 非DKD组 | 112 | 58(51.8) | 54(48.2) | 70.7±5.2 | 23.7±3.0 | 6.8±3.5 | 30(26.8) | 84(75.0) | 7.71±1.14 |
| DKD组 | 215 | 114(53.0) | 101(47.0) | 71.4±6.3 | 24.5±4.5 | 13.6±7.1 | 54(25.1) | 117(54.4) | 8.14±1.67 |
| t(χ2)值 | 0.045a | -1.021 | -1.952 | -11.558 | 0.108a | 13.170a | -2.726 | ||
| P值 | 0.832 | 0.308 | 0.052 | <0.001 | 0.743 | <0.001 | 0.007 | ||
| 组别 | HbA1c(%) | TC(mmol/L) | TG(mmol/L) | LDL(mmol/L) | HDL(mmol/L) | BUN(mmol/L) | Scr(μmol/L) | UACR | |
| 非DKD组 | 7.14±1.05 | 4.82±1.07 | 1.71±0.47 | 2.74±0.60 | 1.11±0.36 | 6.78±1.13 | 77.87±7.80 | 10.96±8.56 | |
| DKD组 | 7.21±0.92 | 4.81±0.89 | 1.78±0.40 | 3.11±0.62 | 1.13±0.34 | 7.11±0.96 | 91.30±20.98 | 293.91±179.48 | |
| t(χ2)值 | -0.573 | 0.125 | -1.392 | -5.246 | -0.649 | -2.710 | -8.346 | -23.066 | |
| P值 | 0.567 | 0.901 | 0.165 | <0.001 | 0.517 | 0.007 | <0.001 | <0.001 | |
| 组别 | 中性粒细胞计数(×109/L) | 淋巴细胞计数(×109/L) | 单核细胞计数(×109/L) | 血小板计数(×109/L) | NLR | MLR | PLR | SII | |
| 非DKD组 | 3.97±1.05 | 1.85±0.41 | 0.37±0.09 | 221.27±39.34 | 2.26±0.78 | 0.21±0.07 | 125.80±39.15 | 431.56±118.26 | |
| DKD组 | 4.71±1.05 | 1.83±0.37 | 0.39±0.13 | 237.33±30.10 | 2.68±0.88 | 0.22±0.09 | 135.29±34.94 | 631.07±185.12 | |
| t(χ2)值 | -6.064 | 0.304 | -1.525 | -3.783 | -4.298 | -1.285 | -2.235 | -11.833 | |
| P值 | <0.001 | 0.768 | 0.128 | <0.001 | <0.001 | 0.200 | 0.026 | <0.001 | |
Table 1 Baseline characteristics of community-dwelling elderly T2DM patients with and without diabetic kidney disease
| 组别 | 例数 | 性别〔n(%)〕 | 年龄(岁) | BMI (kg/m2) | T2DM病程(年) | 吸烟史〔n(%)〕 | 高血压病史〔n(%)〕 | FPG (mmol/L) | |
|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | ||||||||
| 非DKD组 | 112 | 58(51.8) | 54(48.2) | 70.7±5.2 | 23.7±3.0 | 6.8±3.5 | 30(26.8) | 84(75.0) | 7.71±1.14 |
| DKD组 | 215 | 114(53.0) | 101(47.0) | 71.4±6.3 | 24.5±4.5 | 13.6±7.1 | 54(25.1) | 117(54.4) | 8.14±1.67 |
| t(χ2)值 | 0.045a | -1.021 | -1.952 | -11.558 | 0.108a | 13.170a | -2.726 | ||
| P值 | 0.832 | 0.308 | 0.052 | <0.001 | 0.743 | <0.001 | 0.007 | ||
| 组别 | HbA1c(%) | TC(mmol/L) | TG(mmol/L) | LDL(mmol/L) | HDL(mmol/L) | BUN(mmol/L) | Scr(μmol/L) | UACR | |
| 非DKD组 | 7.14±1.05 | 4.82±1.07 | 1.71±0.47 | 2.74±0.60 | 1.11±0.36 | 6.78±1.13 | 77.87±7.80 | 10.96±8.56 | |
| DKD组 | 7.21±0.92 | 4.81±0.89 | 1.78±0.40 | 3.11±0.62 | 1.13±0.34 | 7.11±0.96 | 91.30±20.98 | 293.91±179.48 | |
| t(χ2)值 | -0.573 | 0.125 | -1.392 | -5.246 | -0.649 | -2.710 | -8.346 | -23.066 | |
| P值 | 0.567 | 0.901 | 0.165 | <0.001 | 0.517 | 0.007 | <0.001 | <0.001 | |
| 组别 | 中性粒细胞计数(×109/L) | 淋巴细胞计数(×109/L) | 单核细胞计数(×109/L) | 血小板计数(×109/L) | NLR | MLR | PLR | SII | |
| 非DKD组 | 3.97±1.05 | 1.85±0.41 | 0.37±0.09 | 221.27±39.34 | 2.26±0.78 | 0.21±0.07 | 125.80±39.15 | 431.56±118.26 | |
| DKD组 | 4.71±1.05 | 1.83±0.37 | 0.39±0.13 | 237.33±30.10 | 2.68±0.88 | 0.22±0.09 | 135.29±34.94 | 631.07±185.12 | |
| t(χ2)值 | -6.064 | 0.304 | -1.525 | -3.783 | -4.298 | -1.285 | -2.235 | -11.833 | |
| P值 | <0.001 | 0.768 | 0.128 | <0.001 | <0.001 | 0.200 | 0.026 | <0.001 | |
| 变量 | r(rs)值 | P值 | 变量 | r(rs)值 | P值 |
|---|---|---|---|---|---|
| 性别 | -0.004a | 0.948 | HDL | 0.023 | 0.683 |
| 年龄 | 0.085 | 0.125 | BUN | 0.025 | 0.651 |
| BMI | 0.104 | 0.061 | Scr | 0.403 | <0.001 |
| T2DM病程 | 0.716 | <0.001 | 中性粒细胞计数 | 0.533 | <0.001 |
| 吸烟史 | 0.108a | 0.051 | 淋巴细胞计数 | 0.049 | 0.379 |
| 高血压病史 | -0.12a | 0.830 | 单核细胞计数 | 0.097 | 0.081 |
| FPG | 0.114 | 0.040 | 血小板计数 | 0.226 | <0.001 |
| HbA1c | 0.030 | 0.588 | NLR | 0.538 | <0.001 |
| TC | 0.044 | 0.423 | MLR | 0.066 | 0.236 |
| TG | 0.113 | 0.041 | PLR | 0.430 | <0.001 |
| LDL | 0.144 | 0.009 | SII | 0.494 | <0.001 |
Table 2 Correlation analysis of UACR and other various indicators
| 变量 | r(rs)值 | P值 | 变量 | r(rs)值 | P值 |
|---|---|---|---|---|---|
| 性别 | -0.004a | 0.948 | HDL | 0.023 | 0.683 |
| 年龄 | 0.085 | 0.125 | BUN | 0.025 | 0.651 |
| BMI | 0.104 | 0.061 | Scr | 0.403 | <0.001 |
| T2DM病程 | 0.716 | <0.001 | 中性粒细胞计数 | 0.533 | <0.001 |
| 吸烟史 | 0.108a | 0.051 | 淋巴细胞计数 | 0.049 | 0.379 |
| 高血压病史 | -0.12a | 0.830 | 单核细胞计数 | 0.097 | 0.081 |
| FPG | 0.114 | 0.040 | 血小板计数 | 0.226 | <0.001 |
| HbA1c | 0.030 | 0.588 | NLR | 0.538 | <0.001 |
| TC | 0.044 | 0.423 | MLR | 0.066 | 0.236 |
| TG | 0.113 | 0.041 | PLR | 0.430 | <0.001 |
| LDL | 0.144 | 0.009 | SII | 0.494 | <0.001 |
| 变量 | β | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| T2DM病程 | 0.262 | 0.053 | 24.870 | 1.300(1.173,1.441) | <0.001 |
| 高血压病史 | -1.236 | 0.417 | 8.801 | 0.290(0.128,0.657) | 0.053 |
| FPG | 0.191 | 0.130 | 2.161 | 1.210(0.938,1.560) | 0.142 |
| LDL | 0.942 | 0.339 | 7.720 | 2.565(1.320,4.985) | 0.005 |
| BUN | 0.115 | 0.199 | 0.333 | 1.122(0.760,1.656) | 0.564 |
| Scr | 0.089 | 0.023 | 15.643 | 1.093(1.046,1.143) | <0.001 |
| UACR | 0.850 | 18.573 | 0.002 | 2.340(0,20.105) | 0.963 |
| 中性粒细胞计数 | -0.541 | 0.269 | 4.054 | 0.584(0.344,0.986) | 0.054 |
| 血小板计数 | 0.012 | 0.007 | 3.147 | 1.012(0.999,1.026) | 0.076 |
| NLR | 0.961 | 0.399 | 7.720 | 2.565(1.320,4.985) | 0.005 |
| PLR | -0.016 | 0.009 | 3.319 | 0.984(0.968,1.001) | 0.068 |
| SII | 0.011 | 0.002 | 24.464 | 1.011(1.007,1.015) | <0.001 |
Table 3 Multivariate Logistic regression analysis for factors associated with diabetic kidney disease in community-dwelling elderly T2DM patients
| 变量 | β | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| T2DM病程 | 0.262 | 0.053 | 24.870 | 1.300(1.173,1.441) | <0.001 |
| 高血压病史 | -1.236 | 0.417 | 8.801 | 0.290(0.128,0.657) | 0.053 |
| FPG | 0.191 | 0.130 | 2.161 | 1.210(0.938,1.560) | 0.142 |
| LDL | 0.942 | 0.339 | 7.720 | 2.565(1.320,4.985) | 0.005 |
| BUN | 0.115 | 0.199 | 0.333 | 1.122(0.760,1.656) | 0.564 |
| Scr | 0.089 | 0.023 | 15.643 | 1.093(1.046,1.143) | <0.001 |
| UACR | 0.850 | 18.573 | 0.002 | 2.340(0,20.105) | 0.963 |
| 中性粒细胞计数 | -0.541 | 0.269 | 4.054 | 0.584(0.344,0.986) | 0.054 |
| 血小板计数 | 0.012 | 0.007 | 3.147 | 1.012(0.999,1.026) | 0.076 |
| NLR | 0.961 | 0.399 | 7.720 | 2.565(1.320,4.985) | 0.005 |
| PLR | -0.016 | 0.009 | 3.319 | 0.984(0.968,1.001) | 0.068 |
| SII | 0.011 | 0.002 | 24.464 | 1.011(1.007,1.015) | <0.001 |
| 指标 | 约登指数 | AUC(95%CI) | 灵敏度(%) | 特异度(%) | 最佳截断值 | P值 |
|---|---|---|---|---|---|---|
| NLR | 0.426 | 0.755(0.696,0.814) | 72.1 | 70.5 | 2.49 | <0.001 |
| PLR | 0.339 | 0.689(0.624,0.754) | 90.2 | 43.8 | 112.81 | <0.001 |
| SII | 0.537 | 0.836(0.791,0.881) | 80.5 | 73.2 | 492.08 | <0.001 |
Table 4 ROC analysis of NLR,PLR and SII for predicting diabetic kidney disease in community-dwelling elderly T2DM patients
| 指标 | 约登指数 | AUC(95%CI) | 灵敏度(%) | 特异度(%) | 最佳截断值 | P值 |
|---|---|---|---|---|---|---|
| NLR | 0.426 | 0.755(0.696,0.814) | 72.1 | 70.5 | 2.49 | <0.001 |
| PLR | 0.339 | 0.689(0.624,0.754) | 90.2 | 43.8 | 112.81 | <0.001 |
| SII | 0.537 | 0.836(0.791,0.881) | 80.5 | 73.2 | 492.08 | <0.001 |
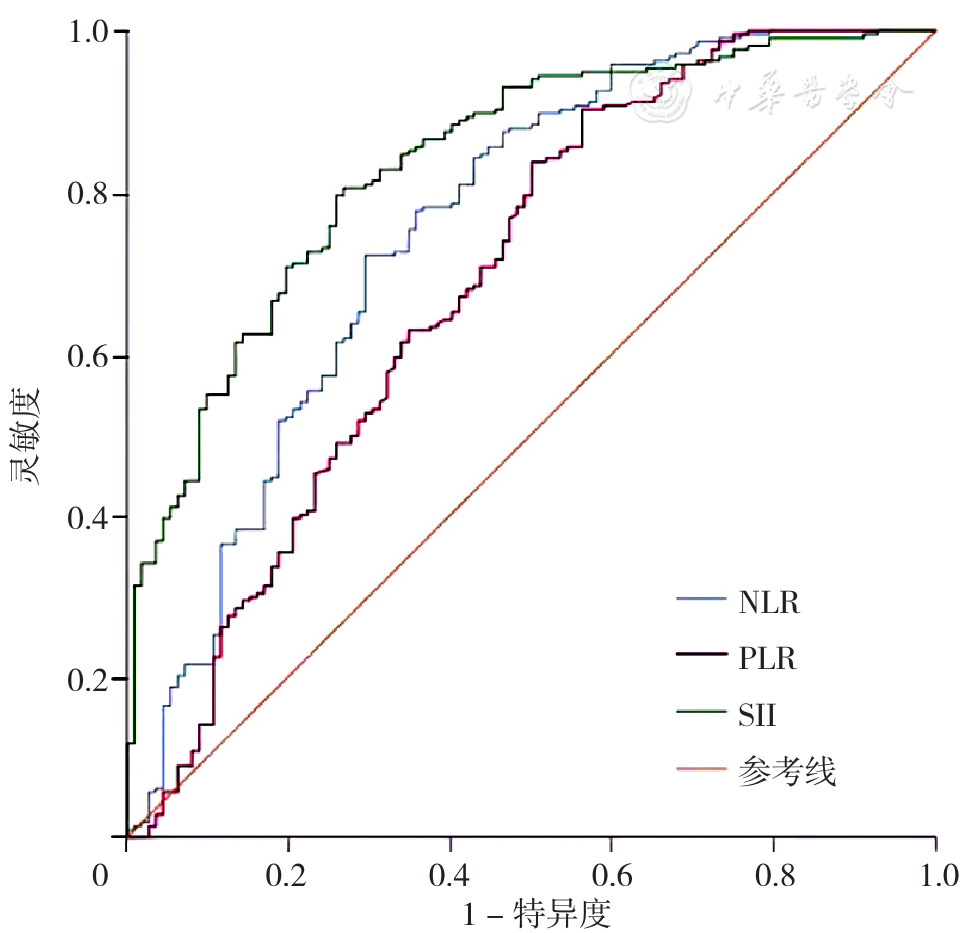
Figure 1 ROC curve of NLR,PLR and SII for predicting diabetic kidney disease in community-dwelling elderly T2DM patients
| [1] |
|
| [2] |
中华医学会糖尿病学分会微血管并发症学组. 中国糖尿病肾脏病防治指南(2021年版)[J]. 中华糖尿病杂志,2021,13(8):762-784. DOI:10.3760/cma.j.cn115791-20210706-00369.
|
| [3] |
何枝荣,吴媛,陈鹏飞. NLR联合ACR评估2型糖尿病早期肾损伤的临床分析[J]. 临床医学工程,2020,27(2):173-174. DOI:10.3969/j.issn.1674-4659.2020.02.0173.
|
| [4] |
中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华糖尿病杂志,2021,13(4):315-409. DOI:10.3760/cma.j.cn115791-20210221-00095.
|
| [5] |
夏文亚,甘言刚,陈安珉,等. SII、NLR、肌酐和CRP对新冠肺炎患者并发AKI的预测价值[J]. 徐州医科大学学报,2021,41(10):753-758. DOI:10.3969/j.issn.2096-3882.2021.10.009.
|
| [6] |
申国旗,马凯,李晶,等. 全身免疫炎症指数与非ST段抬高型急性冠脉综合征患者PCI治疗后对比剂诱导急性肾损伤相关性分析[J]. 江苏医药,2022,48(4):375-380. DOI:10.19460/j.cnki.0253-3685.2022.04.013.
|
| [7] |
|
| [8] |
|
| [9] |
黄冉冉,徐英英,陈矢. 比较中性粒细胞/淋巴细胞、血小板/淋巴细胞和平均血小板体积对早期糖尿病肾病的预测价值[J]. 中华内分泌外科杂志,2019,13(1):76-80. DOI:10.3760/cma.j.issn.1674-6090.2019.01.018.
|
| [10] |
王亚柱,马珂琳,祝丽丽,等. 中性粒细胞/淋巴细胞比值、单核细胞/淋巴细胞比值与2型糖尿病合并冠心病的相关性研究[J]. 临床误诊误治,2021,34(2):44-48. DOI:10.3969/j.issn.1002-3429.2021.02.011.
|
| [11] |
|
| [12] |
|
| [13] |
郭赟. 尿白蛋白/肌酐比值在2型糖尿病早期肾损伤中的应用价值[J]. 医学理论与实践,2018,31(5):734-736. DOI:10.19381/j.issn.1001-7585.2018.05.063.
|
| [14] |
赵锐,孟祥东,靳蕊霞. 中性粒细胞/淋巴细胞比值与2型糖尿病肾病的相关性探讨[J]. 中国现代医学杂志,2017,27(19):101-105. DOI:10.3969/j.issn.1005-8982.2017.19.021.
|
| [15] |
叶晓梅,张敏,曹含弘,等. 中性粒细胞与淋巴细胞比值在糖尿病肾病中的变化及对早期糖尿病肾病的预测价值[J]. 临床内科杂志,2018,35(9):602-605. DOI:10.3969/j.issn.1001-9057.2018.09.008.
|
| [1] | XU Jialan, YAN Hong, WEN Jun, ZHOU Zitong, WANG Siyu. Prevalence of Potentially Inappropriate Medication in Older Adults with Cancer: a Meta-analysis [J]. Chinese General Practice, 2025, 28(30): 3815-3822. |
| [2] | LI Ling, LI Yaping, QIAN Shixing, NIE Jing, LU Chunhua, LI Xia. Research on Influencing Factors and Risk Prediction of Cognitive Function in Community-dwelling Middle-aged and Elderly People [J]. Chinese General Practice, 2025, 28(30): 3773-3778. |
| [3] | ZHANG Ruimin, DONG Zheyi, LI Shuang, WANG Qian, CHEN Xiangmei. Traditional Chinese Medicine Factors Associated with Diabetic Nephropathy Diagnosed by Renal Biopsy [J]. Chinese General Practice, 2025, 28(26): 3307-3313. |
| [4] | JI Bing, JIANG Dudu, CHEN Chen, ZHENG Yanling, SHI Jianwei, FANG Lizheng, DU Xueping. Constructing a Comprehensive Community Clinical Pathway for Herpes Zoster under Graded Treatment Framework [J]. Chinese General Practice, 2025, 28(25): 3110-3118. |
| [5] | YU Wenhua, LI Jianguo, DUAN Wenyan, GAO Xuyan, LI Xiaxia, ZHANG Zilong, ZHANG Li, MA Lina. Reliability and Validity of the Function Impairment Screening Tool among Community-dwelling Older Adults [J]. Chinese General Practice, 2025, 28(24): 3000-3004. |
| [6] | YANG Chen, CHEN Tong, ZHANG Lifang, ZHANG Hongxu, LI Pengfei, ZHANG Xuejuan. Prognostic Impact of Dapagliflozin in Elderly Breast Cancer Survivors with Heart Failure with Preserved Ejection Fraction and Type 2 Diabetes [J]. Chinese General Practice, 2025, 28(24): 3053-3058. |
| [7] | LI Jiaxin, LIU Zhonghui, XIE Shuo, FU Zhifang, SUN Dan, JIAO Hongmei. Trajectory in Biomarkers of Metabolic and Inflammatory States as Early Predictors of Chronic Critical Illness in Aging Patients [J]. Chinese General Practice, 2025, 28(24): 2993-2999. |
| [8] | LI Jinhong, WANG Yu, XU Yaoming, LIU Yang, HOU Jinghui. Exploring the Application Effect of the Joint Outpatient Teaching of General Practice-Specialist-Community Practice Base in Standardized Training of General Practice Residents [J]. Chinese General Practice, 2025, 28(22): 2726-2730. |
| [9] | SHI Jiarui, WANG Zili, ZHANG Xueqing, SONG Yulei, XU Guihua, BAI Yamei. The Current Status of Initial Cognitive Screening Services in Community-based Cognitive Services Centers in Nanjing [J]. Chinese General Practice, 2025, 28(22): 2784-2790. |
| [10] | CHEN Youlan, LAN Yanqi, WU Ahua, ZHANG Haixia, HUANG Jiankang, GUO Zhinan. The Health Management Effect of Contracted Family Doctor Services under the Joint Management of Three Teachers in Xiamen City on Elderly Hypertensive Patients [J]. Chinese General Practice, 2025, 28(22): 2769-2775. |
| [11] | ZHAO Xiaoqing, GUO Tongtong, ZHANG Xinyi, LI Linhong, ZHANG Ya, JI Lihong, DONG Zhiwei, GAO Qianqian, CAI Weiqing, ZHENG Wengui, JING Qi. Construction and Validation of a Risk Prediction Model for Cognitive Impairment in Community-dwelling Older Adults [J]. Chinese General Practice, 2025, 28(22): 2776-2783. |
| [12] | SHI Xiaotian, WANG Shan, YANG Huayu, YANG Yifan, LI Xu, MA Qing. Association between Body Mass Index and Mortality among Older Chinese: a Cohort Study [J]. Chinese General Practice, 2025, 28(22): 2791-2797. |
| [13] | LIU Meixia, YIN Jinnian, WU Mei, YANG Xing, ZHOU Quanxiang, YANG Jingyuan. Impact of Body Mass Index on the Association of Triglyceride Glucose Index with Cognitive Function: a Cross-sectional Study in Rural Older Adults in Guizhou Province [J]. Chinese General Practice, 2025, 28(22): 2806-2812. |
| [14] | WANG Ying, YAN Yijun, LIU Lei, HU Yumin, ZHANG Yang, LIU Kai, JIANG Boren. Effects of Resistance Exercise Combined with Nutritional Intervention on Blood Glucose Stability in Elderly Patients with Type 2 Diabetes Mellitus with Sarcopenia [J]. Chinese General Practice, 2025, 28(21): 2604-2610. |
| [15] | ADILI Tuersun, CHENG Gang. Meta-analysis of the Efficacy and Safety of Finerenone in the Treatment of Type 2 Diabetic Nephropathy [J]. Chinese General Practice, 2025, 28(21): 2686-2691. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||