中国全科医学 ›› 2026, Vol. 29 ›› Issue (01): 108-114.DOI: 10.12114/j.issn.1007-9572.2025.0054
所属专题: 社区卫生服务最新研究合辑
李艳1, 黄豪1, 石建伟2, 宋玮1, 祝墡珠3, 唐岚4,*( )
)
LI Yan1, HUANG Hao1, SHI Jianwei2, SONG Wei1, ZHU Shanzhu3, TANG Lan4,*()
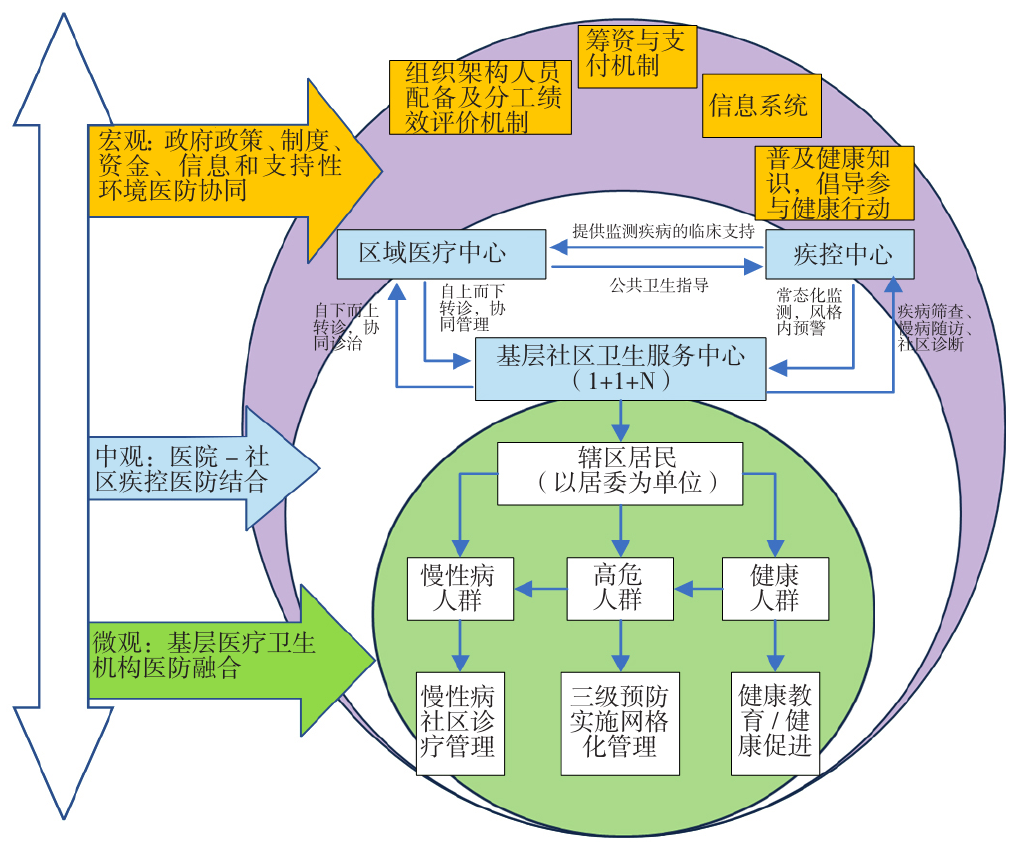
摘要: 背景 在人口老龄化与慢性病负担加剧的背景下,传统的"重治轻防"模式已难以应对挑战并亟须构建医防融合的综合防治体系。尽管国家层面已出台多项政策推动医防融合,但基层医疗卫生机构在实施过程中仍面临诸多困境:一是缺乏系统性的实施路径指导;二是各地实践模式差异较大,缺乏共性机制提炼;三是现有研究多聚焦于医共体层面,对基层医疗卫生机构作为独立主体的医防融合模式研究不足。因此本研究聚焦基层医疗卫生机构这一核心载体,通过多案例进行机制分析,旨在破解"如何实现有效融合"的共性路径问题并提出优化对策。 目的 分析基层医疗卫生机构实现慢性病医防融合业务模式的关键实现机制,为各地基层医疗卫生机构探索符合当地实际情况的医防融合式慢病管理服务模式提供参考。 方法 于2024年11月采用文献研究法梳理、总结医防融合的文献案例,然后借鉴彩虹模型的4个层面、7个条件运用定性比较分析针对基层医疗卫生机构开展的慢性病医防融合业务的14个案例进行良好慢性病医防融合效果的实现机制探索,进而开展半结构化访谈提出优化意见。 结果 共有4条组态路径能有效提升基层社区慢性病医防融合效果,组态路径1中微观整合型、组态路径2微观及支持要素层整合型、组态路径3多层面整合型和组态路径4全层面整合型,4条组态路径的组合覆盖率0.857,能够解释大多数案例中的良好医防融合效果,组合一致性1.000,能够很好地解释良好医防融合效果的产生路径。服务整合和功能整合是实现良好医防融合效果的核心基础,分别强调连续的慢性病健康管理和监督考核机制的重要性,而系统整合则凸显了政策支持的关键作用。不同组态在核心条件、整合层面和支持要素上的差异表明,医防融合的实现路径可因地区资源和政策条件的不同而灵活调整,并非单一模式。 结论 为实现基层医疗卫生机构慢性病医防融合业务的可持续良好发展,需要从宏观层面加强政策支持和系统整合,中观层面促进多层面协作和资源下沉,微观层面强化服务整合、注重团队人员整合以确保健康管理的连续性,支持要素方面建立有效的监督考核机制和绩效激励机制。