中国全科医学 ›› 2026, Vol. 29 ›› Issue (09): 1161-1167.DOI: 10.12114/j.issn.1007-9572.2024.0565
夏宁1, 石岚1, 丁万宝1, 张洁1, 龙轶1, 戴辉1, 张灿2, 戴海龙2,*( )
)
XIA Ning1, SHI Lan1, DING Wanbao1, ZHANG Jie1, LONG Yi1, DAI Hui1, ZHANG Can2, DAI Hailong2,*()
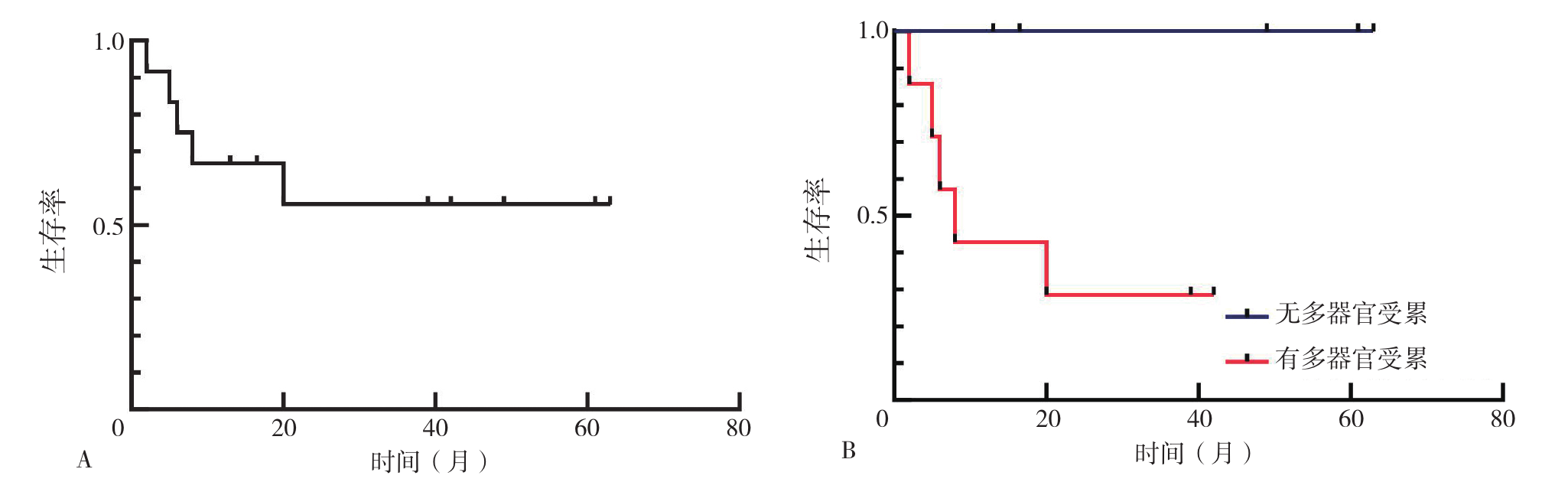
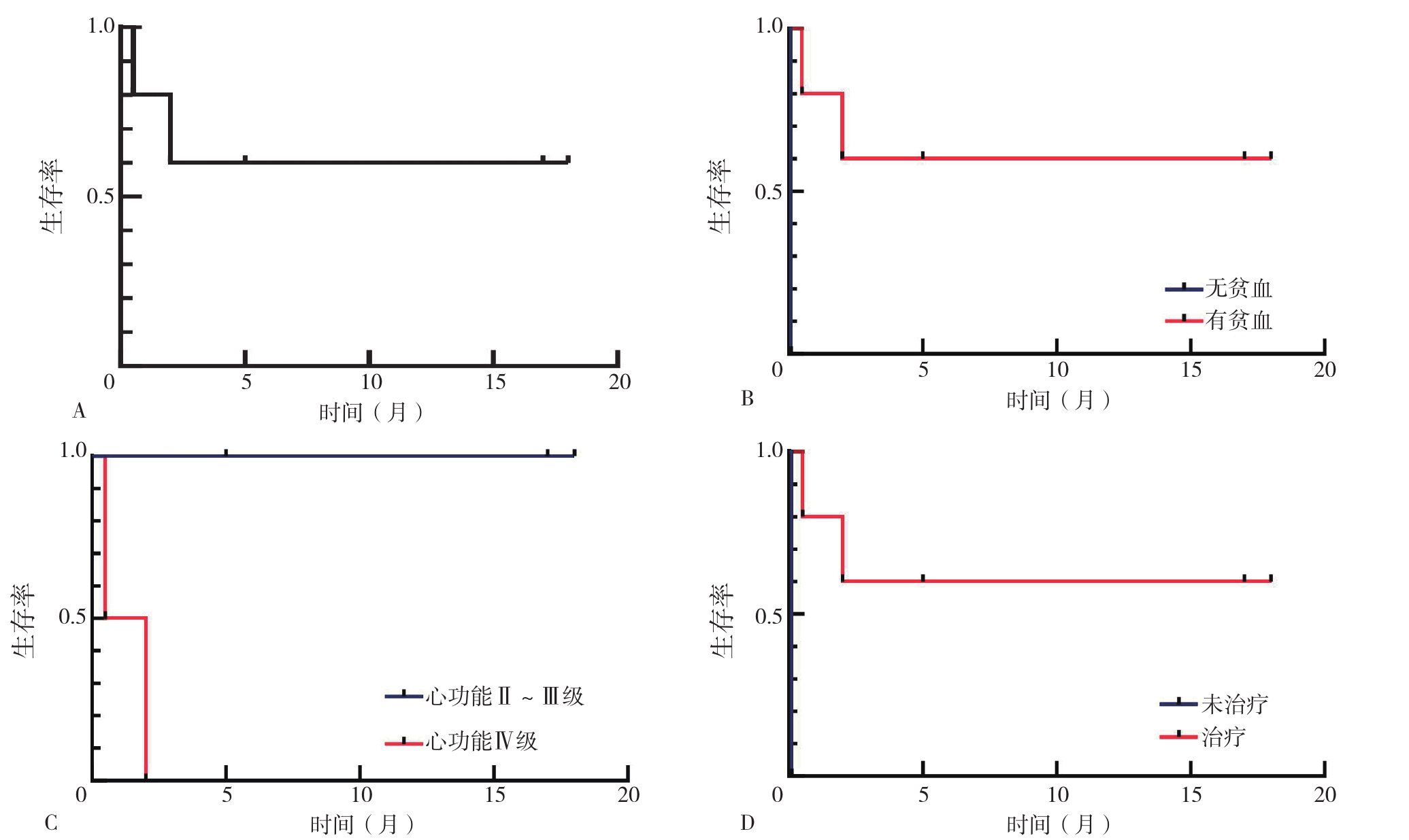
摘要: 背景 淀粉样变性患者临床表现多样且缺乏特异性,容易被漏诊、误诊,早期诊断及积极治疗对疾病预后至关重要。 目的 通过分析本中心诊断为淀粉样变性患者的临床特点及预后,提高对该疾病的认识。 方法 回顾性分析2015年1月—2023年10月于昆明医科大学附属延安医院69例确诊为淀粉样变性患者的临床资料,并通过电话随访收集患者生存情况,根据诊断为同种类型的淀粉样变性患者的生存结局分为死亡组与存活组。绘制患者的Kaplan-Meier生存曲线,进行Log-rank检验。 结果 共纳入69例淀粉样变性患者,其中脑血管淀粉样变性(CAA)35例,中位确诊年龄72(66,80)岁,临床特点主要为脑出血、认知障碍或痴呆,其中6例(17.1%)CAA患者初诊住院期间死于脑出血;皮肤淀粉样变性12例,中位确诊年龄67.0(53.5,75.5)岁,主要临床表现为胫前、四肢伸侧及背部等部位出现粟粒至绿豆大小的丘疹;喉淀粉样变性3例,主要表现为声音嘶哑、咽喉部不适、喉部异物感;多发性骨髓瘤(MM)合并轻链型淀粉样变性6例,平均年龄(60.8±9.0)岁,总体中位生存时间为3.5个月,5例(83.3%)患者有多器官受累(2个及以上器官受累),1例(16.7%)患者为单器官受累,6例患者均有水肿症状,5例(83.3%)伴有胸闷、气促,1例(16.7%)伴有骨痛,1例(16.7%)伴有四肢麻木,其中1例患者初诊时未开始治疗即死于心源性猝死;系统淀粉样变性13例[其中系统性轻链型(AL)淀粉样变性12例,AA型淀粉样变性1例],12例AL淀粉样变性患者多以乏力(10例,83.3%)、水肿(9例,75.0%)为首发症状,其次为泡沫尿(6例,50.0%)和胸闷(6例,50.0%),还可表现为气促、体质量减轻、肢体麻木、厌食、排便不规律等症状,其中累及1个器官者5例(41.7%),2个及以上器官受累者7例(58.3%),常见受累器官为肾脏(9例,75.0%)和心脏(8例,66.7%),其次为肝脏(3例,25.0%)。AL淀粉样变性患者死亡组24 h尿蛋白明显高于存活组(P<0.05)。Kaplan-Meier法分析结果显示AL淀粉样变性患者中位生存时间为18.3个月;Log-rank检验显示累及2个及以上器官的患者较累及单个器官的患者生存时间缩短(χ2=4.757,P=0.029)。MM合并轻链型淀粉样变性患者的总体中位生存时间为3.5个月,其中初诊死亡1例;MM合并轻链型淀粉样变性患者中,贫血患者生存时间较无贫血患者明显缩短(χ2=5.000,P=0.025);心功能Ⅳ级患者生存时间较心功能Ⅱ~Ⅲ级患者明显缩短(χ2=5.052,P=0.029);未接受治疗的患者生存时间较接受治疗的患者明显缩短(χ2=5.000,P=0.025)。 结论 淀粉样变性的临床表现多种多样,不同类型的淀粉样变性预后差异大;CAA为老年人易患病,且合并脑出血时急性期病死率高;MM合并轻链型淀粉样变性患者起病首发症状以淀粉样变性累及心、肾等重要器官的症状为主,有贫血及心功能分级Ⅳ级可能为预后不良因素,积极接受治疗可能为改善患者预后的有利因素;AL淀粉样变性患者累及多器官时提示预后不良。