中国全科医学 ›› 2024, Vol. 27 ›› Issue (33): 4147-4154.DOI: 10.12114/j.issn.1007-9572.2024.0032
周镇森1,2, 黄岩2, 程思为3, 张小玉2, 张晓雨4, 孙婷1, 杨先军2, 谢晖1, 马祖长2,3,*( )
)
ZHOU Zhensen1,2, HUANG Yan2, CHENG Siwei3, ZHANG Xiaoyu2, ZHANG Xiaoyu4, SUN Ting1, YANG Xianjun2, XIE Hui1, MA Zuchang2,3,*()
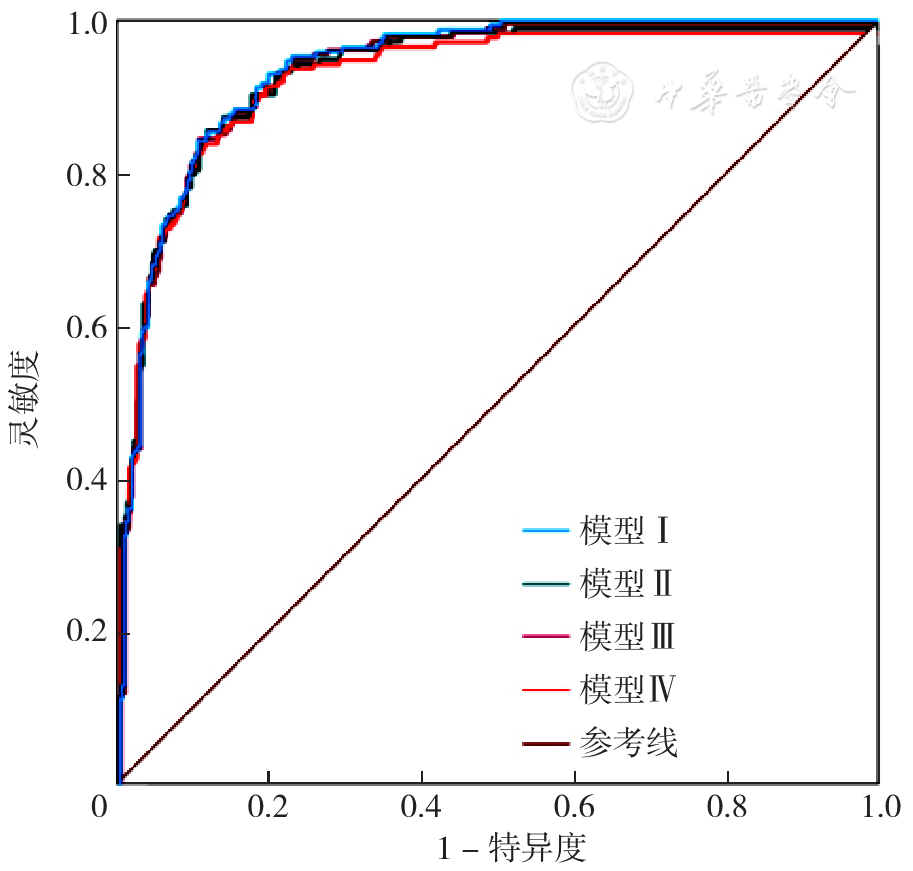
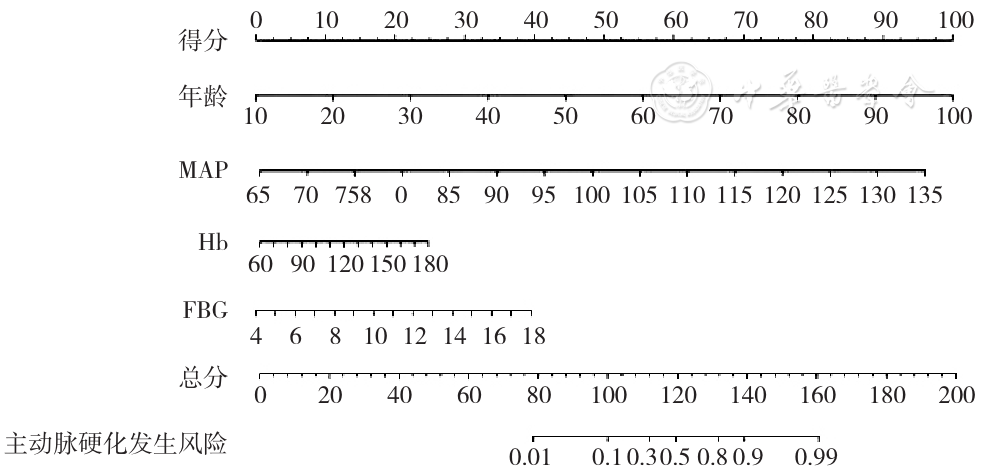
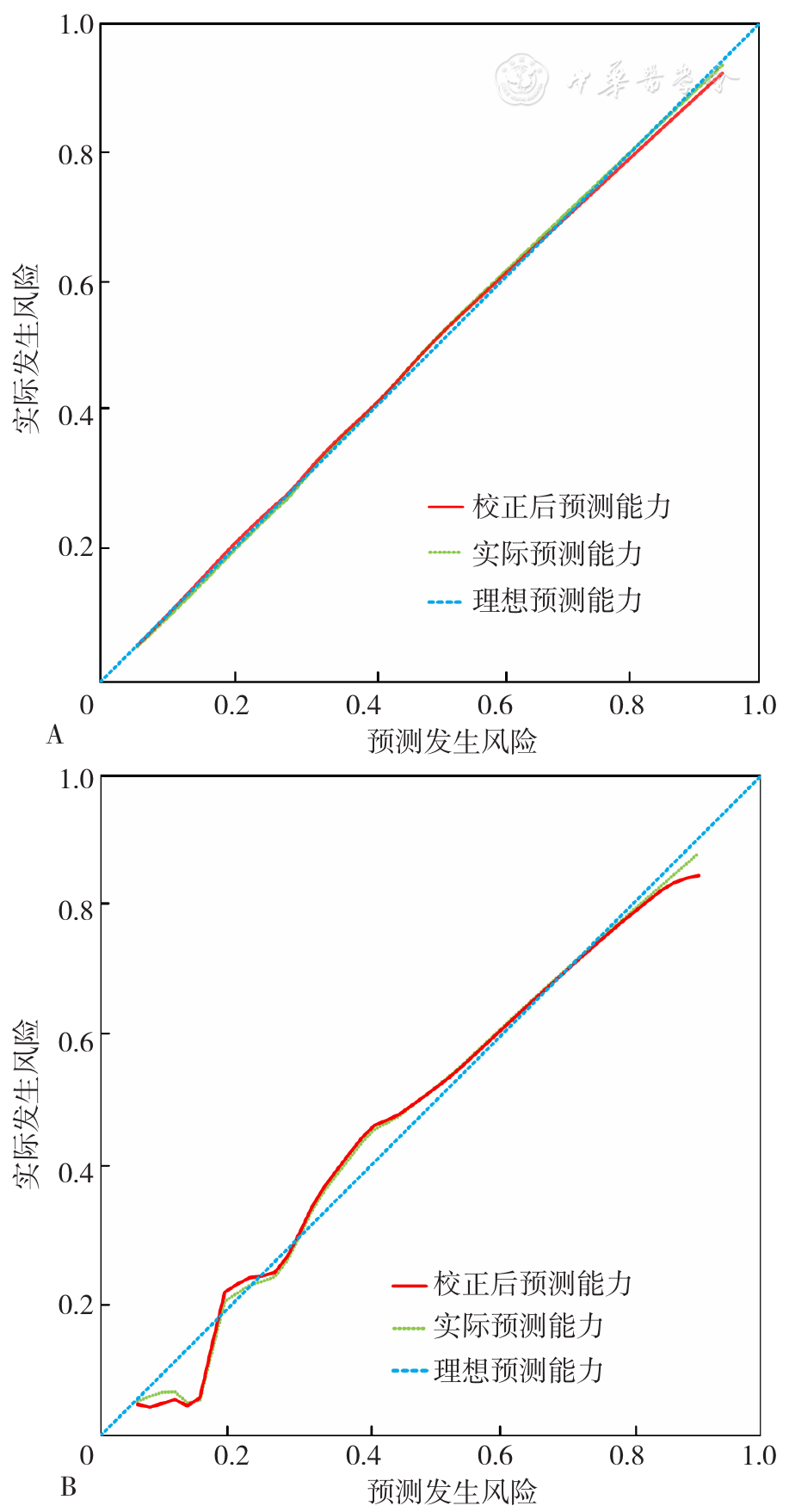
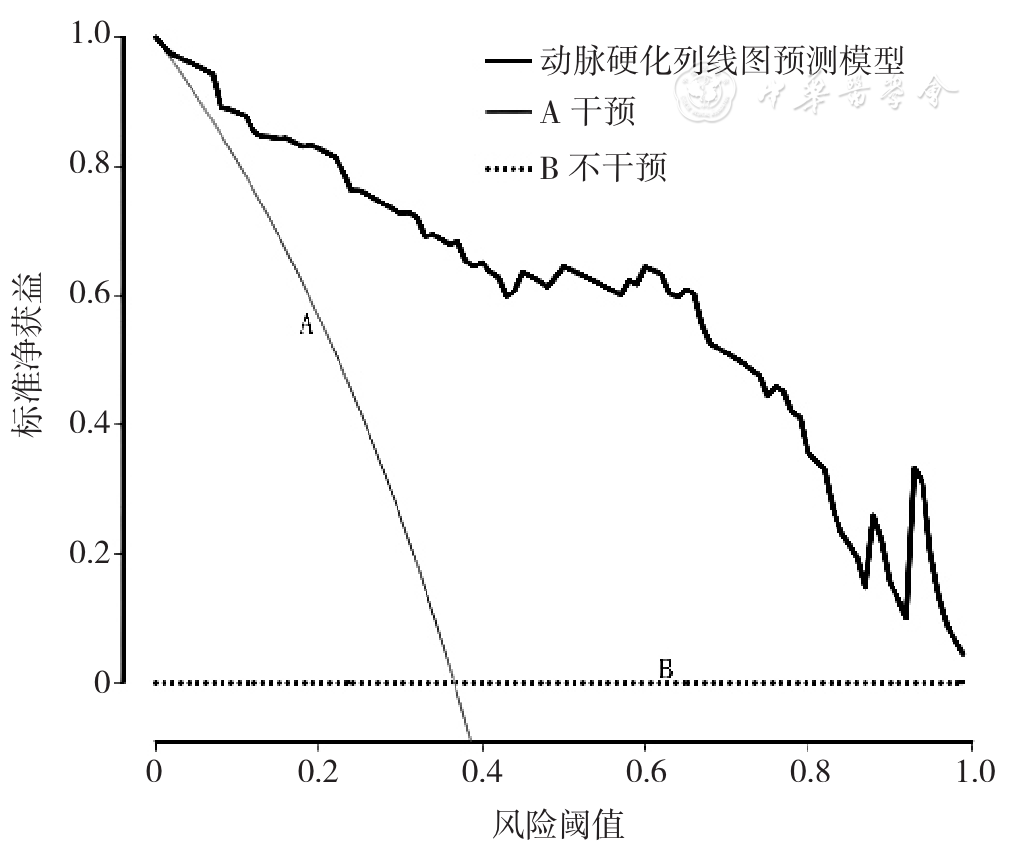
摘要: 背景 在心血管风险评估领域,主动脉僵硬度被认为是关键的预测指标,颈股脉搏波传导速度(cfPWV)被认为是无创评估主动脉硬化风险的金标准。由于技术难度等挑战,我国cfPWV检测尚未广泛开展。 目的 本研究旨在开发并验证一种基于心血管危险因素的早期主动脉硬化风险筛查模型,以期替代cfPWV复杂的测量过程,减少对传统测量方法的依赖。 方法 选取2023年5—11月在安徽医科大学第一附属医院体检中心招募的878名受试者作为研究对象,按照8∶2的比例进行随机抽样分为建模组(n=703)和验证组(n=175)。收集患者一般资料、实验室检查结果及cfPWV。依据cfPWV检查结果和相关指南,将建模组受试者分为无主动脉硬化风险(n=503)和有主动脉硬化风险(n=200)。采用多因素Logistic回归分析并筛选变量,建立列线图评估模型。绘制模型预测主动脉硬化发生风险的受试者工作特征曲线(ROC曲线),以ROC曲线下面积(AUC)、Hosmer-Lemeshow检验评估模型的区分度和校准度,采用Delong检验比较各模型的AUC,采用决策曲线分析(DCA)评估模型临床实用性,并采用Bootstrap法重复采样1 000次对模型进行内部验证。 结果 建模组有主动脉硬化风险者年龄、BMI、收缩压(SBP)、舒张压(DBP)、平均动脉压(MAP)、尿素、空腹血糖(FBG)、低密度脂蛋白胆固醇(LDL-C)、三酰甘油(TG)、总胆固醇(TC)、丙氨酸氨基转移酶(ALT)、天冬氨酸氨基转移酶(AST)、血红蛋白(Hb)、饮酒、血脂异常、糖尿病比例高于无主动脉硬化风险者,肾小球滤过率(GFR)、血小板计数(PLT)低于无主动脉硬化风险者(P<0.05)。多因素Logistic回归分析结果显示年龄(OR=1.112,95%CI=1.082~1.143)、MAP(OR=1.146,95%CI=1.107~1.188)、Hb(OR=1.026,95%CI=1.004~1.049)和FBG(OR=1.353,95%CI=1.076~1.701)是主动脉硬化的独立影响因素(P<0.05)。纳入多因素Logistic回归分析结果差异有统计学意义的指标(年龄、MAP、Hb、FBG)构建预测模型Ⅰ,同时分别纳入吸烟、性别、血脂异常构建模型Ⅱ、模型Ⅲ、模型Ⅳ,绘制模型Ⅰ~模型Ⅳ的ROC曲线,模型Ⅰ~模型Ⅳ的AUC分别为0.941(95%CI=0.923~0.964,P<0.05)、0.941(95%CI=0.922~0.962,P<0.05)、0.941(95%CI=0.922~0.963,P<0.05)、0.939(95%CI=0.919~0.962,P<0.05);Delong检验结果示,模型Ⅰ、模型Ⅱ、模型Ⅲ、模型Ⅳ的AUC比较,差异无统计学意义(P>0.05)。根据多因素Logistic回归分析结果,以年龄、MAP、FBG、Hb为预测因子构建列线图模型,预测模型训练集的AUC为0.941(95%CI=0.920~0.962),灵敏度为0.832,特异度为0.917。验证集的AUC为0.961(95%CI=0.914~1.000),灵敏度为0.872,特异度为0.964。DCA结果显示使用主动脉硬化早期筛查模型可以使受试者在临床中获益。 结论 本研究基于年龄、MAP、Hb和FBG 4个简易指标,建立了早期主动脉硬化风险筛查模型,提供了便捷、高效的早期血管功能筛查的方法。
中图分类号: