Background Pulmonary diffusing capacity testing is widely used in clinical practice for assisting in the diagnosis and quantitative evaluation of interstitial lung diseases, differentiating emphysema, and assessing whether other pulmonary diseases are complicated with pulmonary diffusing capacity impairment, among other applications. In recent years, several new domestic pulmonary diffusing capacity testing instruments have been successively developed, registered and launched on the market; however, their reliability in clinical use remains to be verified.
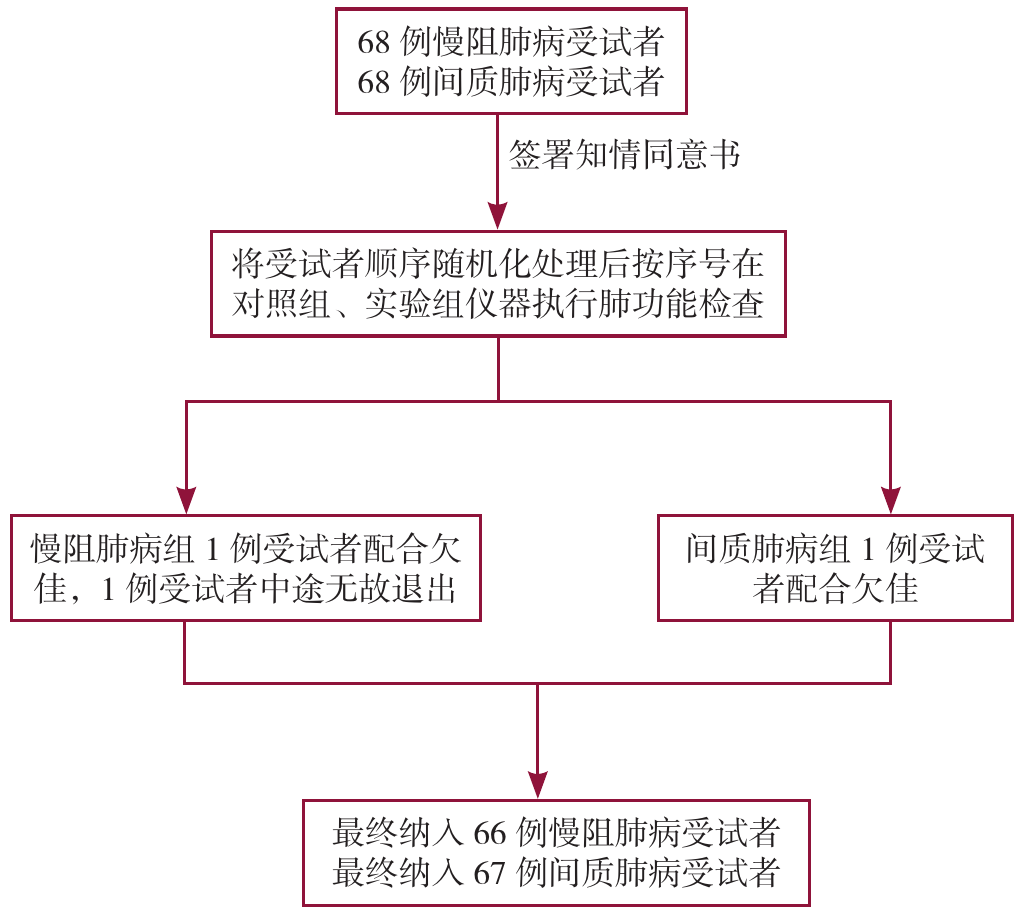
Methods From June 15 to September 1, 2023, among patients who underwent examinations in the Pulmonary Function Laboratory of the First Affiliated Hospital of Guangzhou Medical University, 68 subjects with clinically diagnosed chronic obstructive pulmonary disease (COPD) and 68 with interstitial lung disease (ILD) were randomly selected, and divided into the ILD group and the COPD group. A cross-over design was adopted, where the subjects were randomly assigned to use two types of pulmonary diffusing capacity testing instruments in sequence: the experimental group (MeHow MeAir 9000) and the control group (Jaeger MasterScreen Diffusion). Professional pulmonary function examiners performed pulmonary diffusing capacity and vital capacity tests on the subjects in accordance with the procedural and quality control standards specified in the standards for single-breath carbon monoxide uptake in the lung guideline issued by the European Respiratory Society/American Thoracic Society (ERS/ATS). The collected indicators included: diffusing capacity of the lung for carbon monoxide (DLCO), inspiratory vital capacity (IVC), alveolar ventilation (VA), ratio of diffusing capacity of the lung for carbon monoxide to alveolar ventilation (DLCO/VA), forced vital capacity (FVC), forced expired volume in one second (FEV1), and percentage of predicted diffusing capacity of the lung for carbon monoxide (DLCO%pred). Consistency analysis was conducted on the measurement results obtained by the two groups of instruments and the results of the grading of pulmonary diffusing capacity impairment severity.
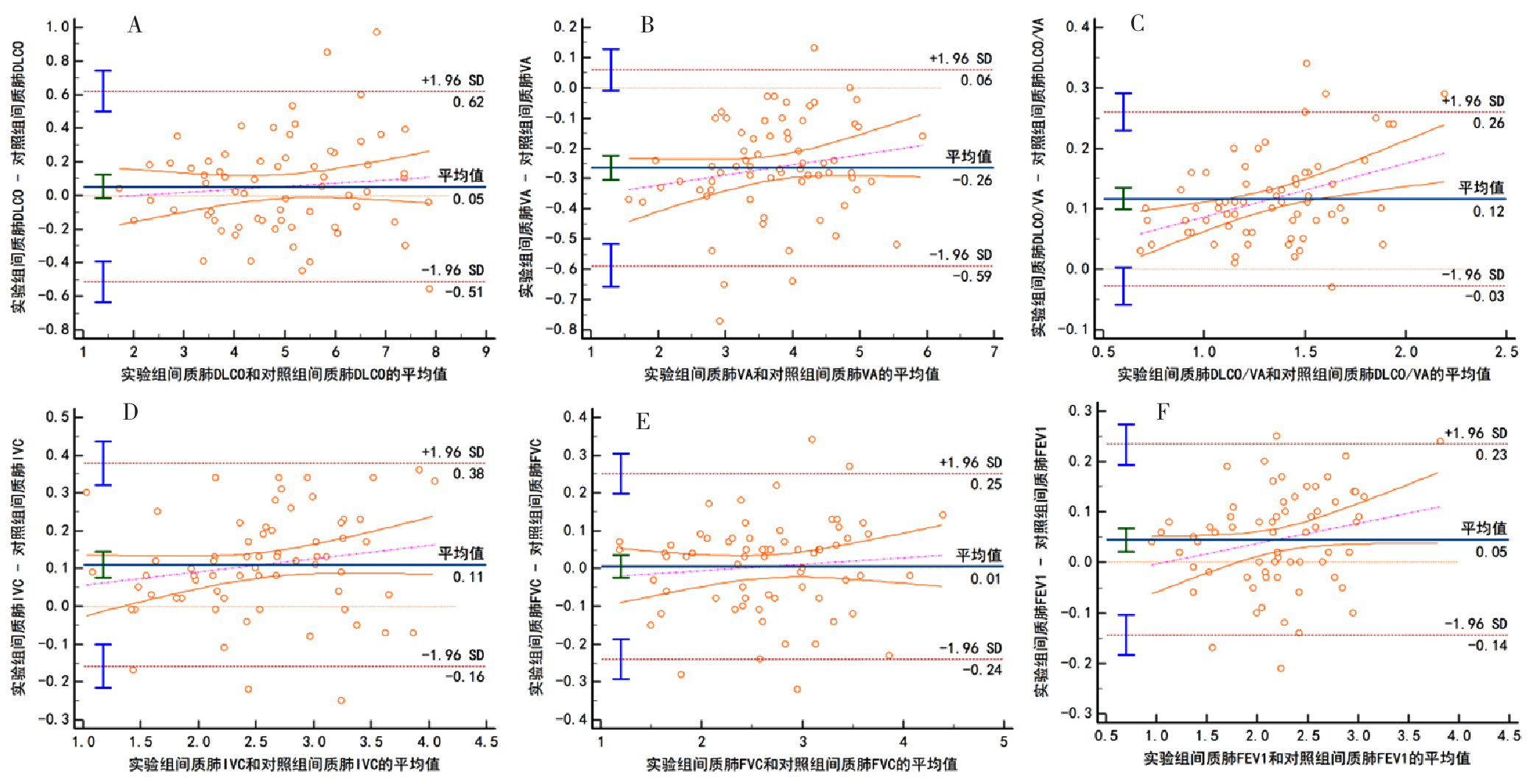
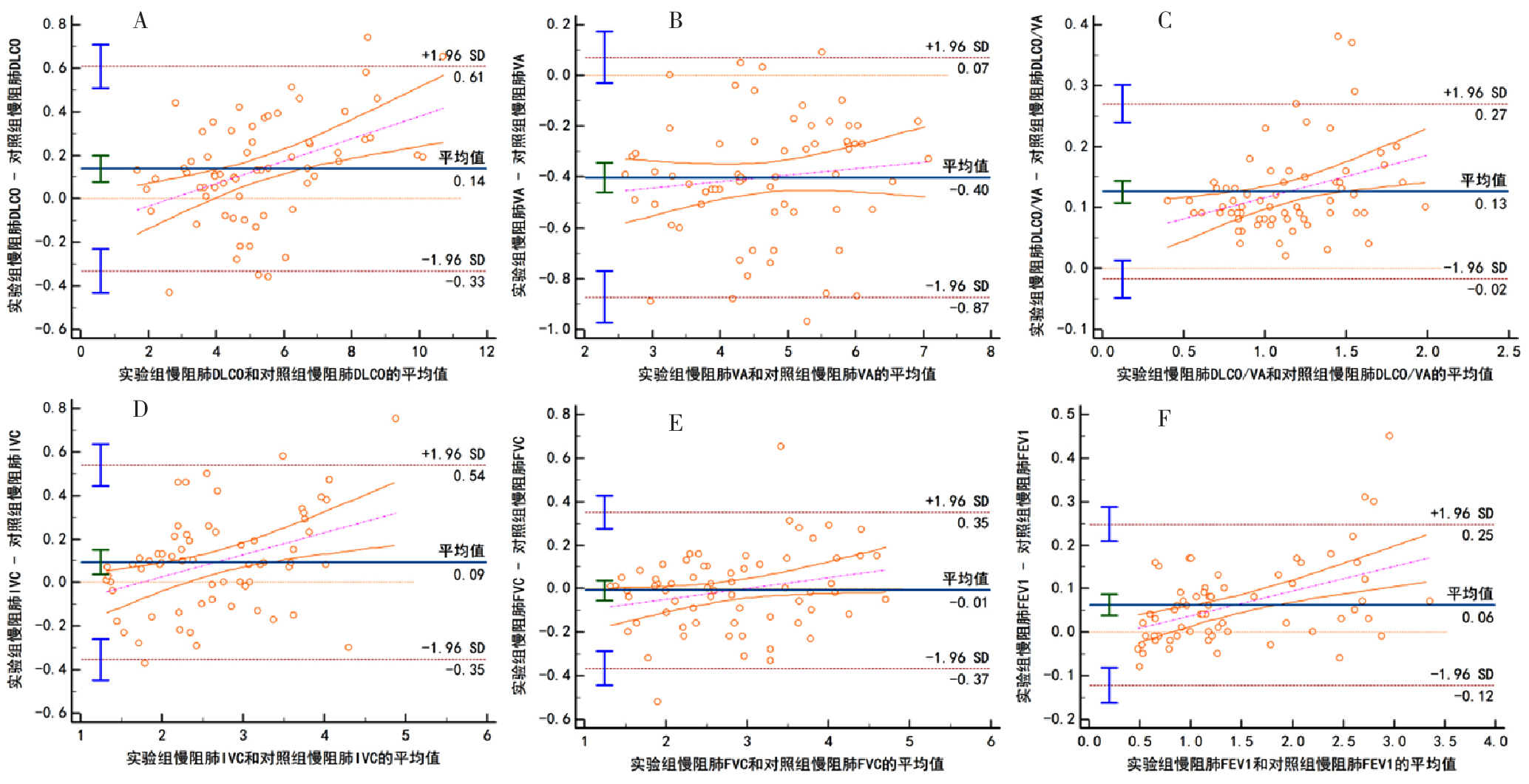
Results Statistical analysis and comparison of the consistency of measurement values of DLCO, IVC, VA, DLCO/VA, FVC, and FEV1 between the two instruments: in the interstitial lung disease group, the ICCs were 0.981 6, 0.944 9, 0.916 8, 0.969 8, 0.984 4, and 0.982 4 respectively; in the COPD group, the ICCs were 0.990 7, 0.917 9, 0.920 9, 0.960 2, 0.979 8, and 0.989 7 respectively. The analysis results of both disease groups showed high consistency, and the results were statistically significant (P< 0.05). In the Bland-Altman scatter plots of the measurement values of DLCO, IVC, VA, DLCO/VA, FVC, and FEV1 from the two instruments, the proportions of data points falling within the 95% confidence interval (95%CI) in the interstitial lung disease group were 95.5%, 94.0%, 94.0%, 95.5%, 92.5% and 94.0% respectively; in the COPD group, the proportions were 92.4%, 93.9%, 93.9%, 95.5%, 97.0% and 95.5% respectively. These results indicated that the consistency of diffusing capacity measurement values between the experimental group instrument and the control group instrument was good. In terms of the comparison of the two instruments regarding the grading of diffusing capacity impairment (classified into 4 grades: normal, mild, moderate, and severe based on DLCO%pred) in both disease groups, the ICCs in the interstitial lung disease group and the COPD group were 0.939 7 and 0.975 0 respectively, with statistically significant results (P< 0.05). The weighted kappa values from Cohen's weighted kappa test for consistency strength were 0.896 9 and 0.837 2 respectively, and the analysis results were statistically significant (P< 0.05), suggesting that the experimental group instrument and the control group instrument have good consistency in evaluating the grading of pulmonary diffusing capacity impairment.
Conclusion The pulmonary diffusing capacity testing of the new domestic MeHow MeAir 9000 shows high measurement accuracy in chronic respiratory diseases and good reliability in evaluating the severity of pulmonary diffusing capacity impairment, making it suitable for clinical promotion and application.

 )
)