中国全科医学 ›› 2024, Vol. 27 ›› Issue (21): 2592-2599.DOI: 10.12114/j.issn.1007-9572.2023.0839
谭璐1, 陈涛1, 高洪蛟2, 陈彦希1, 任艳1,*( )
)
TAN Lu1, CHEN Tao1, GAO Hongjiao2, CHEN Yanxi1, REN Yan1,*()
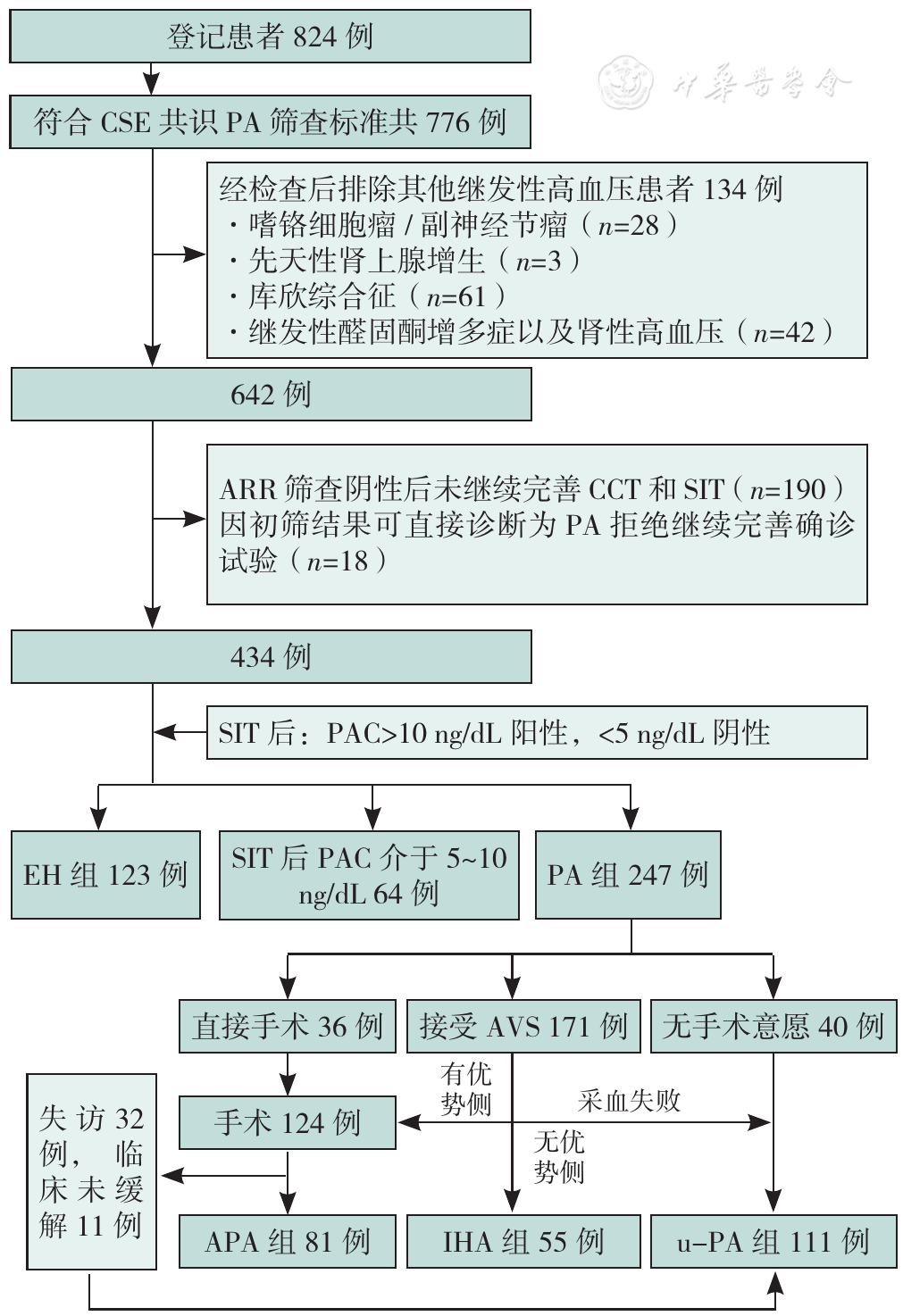
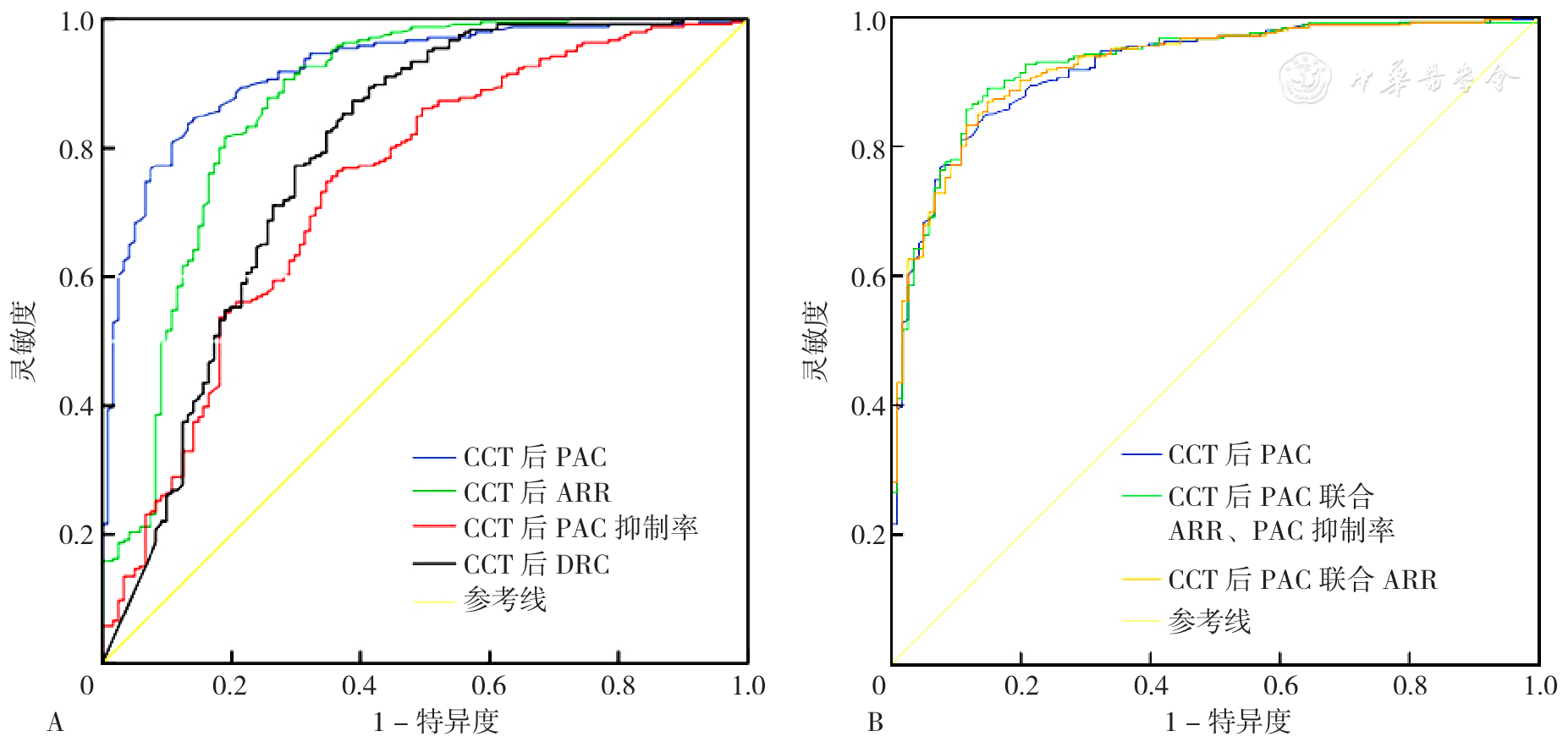
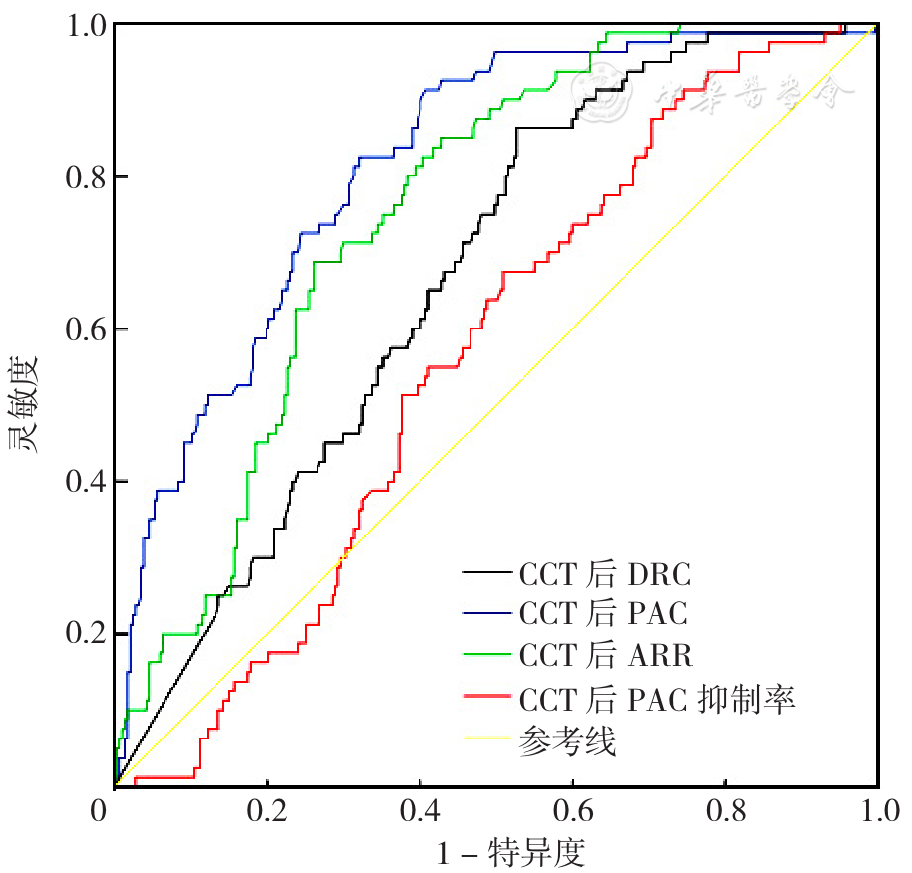
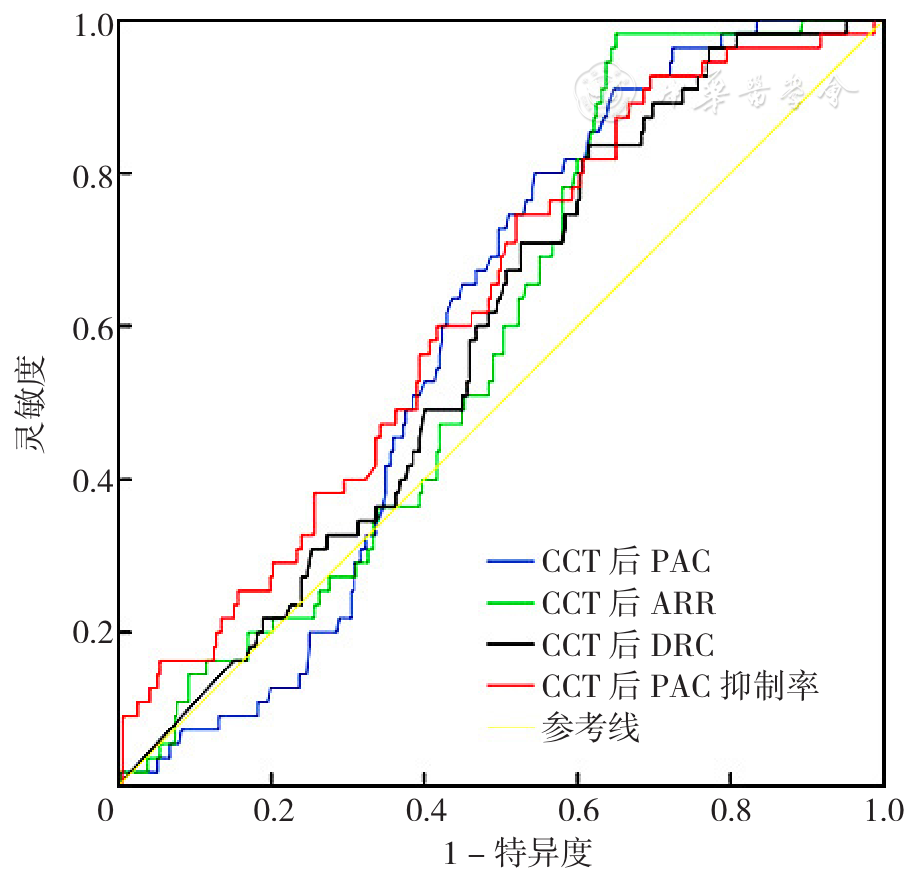
摘要: 背景 原发性醛固酮增多症(PA)作为继发性高血压中发病率最高、心脑血管危害大但手术后治愈率高的疾病,已被各大高血压指南推荐扩大筛查、早期诊断和治疗。但该类患者的确诊、分型和治疗后临床转归判定方式繁多且存在较多争议。卡托普利抑制试验(CCT)因其便捷、安全可直接用于社区、门诊,期望CCT能对PA患者进行全程管理以改善预后。 目的 探究CCT对PA的诊断、分型以及临床转归的判断能力。 方法 选取2020-10-01—2022-12-30在四川大学华西医院内分泌代谢科接受内分泌性高血压病因筛查并登记的824例患者为研究对象。经筛选后最终370例患者纳入研究,其中123例原发性高血压(EH)患者纳入EH组,247例PA患者分别纳入单侧醛固酮瘤(APA)组81例、特发性醛固酮增多症(IHA)组55例和未分型PA(u-PA)组111例。比较4组间差异并绘制CCT后各指标及联合诊断PA的受试者工作特征(ROC)曲线,确定最佳截断值。其次绘制CCT后各指标诊断APA和IHA亚型的ROC曲线,计算ROC曲线下面积(AUC)评估CCT对APA和IHA的分型判断能力。最后根据术后临床结局将单侧肾上腺切除患者分为3组:未缓解组11例、临床改善组27例和临床缓解组54例,比较3组间差异并判断CCT对APA患者术后临床转归的判断能力。 结果 CCT后血浆醛固酮浓度(PAC)对PA的诊断效能最高(AUC=0.921,95%CI=0.893~0.950),最佳截断值为11.7 ng/dL,灵敏度、特异度分别为84.6%和86.0%;CCT后醛固酮/肾素比值(ARR)对PA也有较好的诊断效能(AUC=0.868,95%CI=0.823~0.923),最佳截断值为2.8(ng/dL)/(mU/L),灵敏度、特异度分别为82.2%和81.0%。CCT后PAC>17.0 ng/dL可协助诊断APA亚型,CCT后PAC<11.7 ng/dL同时ARR<2.8(ng/dL)/(mU/L)的患者可排除APA亚型。在接受手术治疗的患者中,有87.2%患者经CCT后PAC<11.7 ng/dL,89.7%患者CCT后ARR<2.8(ng/dL)/(mU/L)均接近术后临床缓解水平(88.0%)。 结论 CCT可全程用于PA患者的诊断、分型和临床转归评价,CCT后PAC及CCT后ARR诊断PA的最佳截断值分别为11.7 ng/dL和2.8(ng/dL)/(mU/L),也可用于APA的分型判断以及术后生化缓解的判断。CCT前采血检验临床意义小,可适当简化流程。