
Chinese General Practice ›› 2025, Vol. 28 ›› Issue (35): 4385-4396.DOI: 10.12114/j.issn.1007-9572.2025.0227
Special Issue: 睡眠问题专题研究
• Guidelines·Consensus • Previous Articles Next Articles
Received:2025-07-10
Revised:2025-08-30
Published:2025-12-15
Online:2025-10-15
基金资助:CLC Number:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2025.0227
| 序号 | 核心问题 | 推荐意见 | 证据质量 | 推荐强度 |
|---|---|---|---|---|
| 1 | 虚拟现实(VR)技术在改善肿瘤相关性失眠(CRI)中的主要干预机制有哪些? | 【推荐意见1】 VR技术通过注意力分散、沉浸式多模态放松诱导、认知重构以及实时生物反馈与自我调节等多重核心机制协同作用,有效干预CRI。这些机制从心理和生理层面缓解患者的过度唤醒状态和非适应性认知,从而改善睡眠质量,构成一个有机整合的干预框架 | B | 强推荐 |
| 2 | 针对CRI,VR技术居家康复的推荐干预方案(包括内容、时长、频率、疗程)是什么? | 【推荐意见2】 针对CRI,VR技术居家康复可根据患者具体需求和情况,选择以下干预方案:VR自然场景模拟干预,推荐为1次/d,15~20 min/次,持续3~4周;VR引导的身心实践(如正念冥想与呼吸训练),推荐1次/d,30 min/次,持续6周;VR辅助的失眠认知行为疗法(CBT-I),推荐1~2次/d,15~30 min/次,持续3~6周;VR结合生物反馈(VR-BF),推荐1次/d,15~30 min/次,持续7~10 d或更长。这些方案各有侧重,共同为CRI患者提供了多样化的居家康复选择 | C | 弱推荐 |
| 3 | VR技术在CRI居家康复中的实施流程包括哪些步骤? | 【推荐意见3】 VR技术在CRI居家康复中的实施流程应包括干预前筛查评估、设备调试及干预、安全管理与监督、定期评估与调整4个核心阶段 | D | 强推荐 |
| 4 | 如何客观有效地评估VR技术居家康复对CRI的疗效?推荐使用哪些评价指标? | 【推荐意见4】 应采用主观与客观指标相结合、全面覆盖睡眠核心问题、共病症状及生活质量的多维度评价体系评估VR技术居家康复对CRI的疗效。推荐首选睡眠量表匹兹堡睡眠质量指数(PSQI)和失眠严重指数量表(ISI)进行初筛,警惕主观认知偏差;对于肿瘤的脆弱人群,推荐居家监测核心方案为"体动记录仪连续佩戴≥7 d+同步睡眠日记",前者客观追踪睡眠效率(SE)、觉醒时间(WASO)等参数,后者通过记录上床/起床时间及夜间症状等校准设备静卧误判;此组合可动态评估治疗反应,替代重复多导睡眠监测(PSG)。PSG作为睡眠医学诊断的金标准,建议对疑似器质性共病的CRI患者采用,但无法实现长期居家监测。此外,为全面了解VR干预的综合效果,还应结合共病症状量表[如患者健康问卷抑郁症状群量表(PHQ-9)、广泛性焦虑量表(GAD-7)、数字疼痛评分量表(NRS)、简明疲乏量表中文版(BFI-C)]和生活质量量表[如欧洲癌症研究与治疗组织生活质量核心问卷(EORTC QLQ-C30)]进行评估,以明确VR干预对患者整体身心健康和生活质量的改善 | A | 强推荐 |
| 5 | VR技术应用于CRI居家康复的安全性问题有哪些,应如何评估和管理? | 【推荐意见5】 VR技术应用于CRI居家康复时,需全面关注并管理其生理、心理社会及技术3方面的安全性风险。生理方面,应警惕晕动病、视觉系统负荷和心血管影响;针对晕动病,推荐通过虚拟现实晕动病问卷(CSQ-VR)及心率(HR)、心率变异性(HRV)等客观指标评估;针对视觉系统负荷,建议限制VR技术干预单次时长≤30 min,首次使用建议10 min,增加休息和眨眼并定期进行眼科检查;针对心血管系统影响,建议筛查基线血压、避免高频动态场景。心理社会方面,需警惕沉浸式环境可能加剧焦虑/抑郁或诱发创伤闪回,推荐VR技术干预前后使用医院焦虑抑郁量表(HADS)、PHQ-9、GAD-7等量表进行评估监测;建议照护者对患者进行密切监测,防范现实感混淆与社交回避问题。技术方面,应确保硬件符合安全规范,建议设备具备高分辨率(每只眼睛≥2 K)、高刷新率(90~120 Hz)、最小延迟(<45 ms)和宽视场角(中央≥60°,整体理想≥100°);并严格保护患者数据隐私,进行匿名化、加密、访问控制 | B | 强推荐 |
Table 1 Recommendations summary of Expert Consensus on the Application of Virtual Reality Technology in Home-based Rehabilitation for Cancer-related Insomnia(2025 Edition)
| 序号 | 核心问题 | 推荐意见 | 证据质量 | 推荐强度 |
|---|---|---|---|---|
| 1 | 虚拟现实(VR)技术在改善肿瘤相关性失眠(CRI)中的主要干预机制有哪些? | 【推荐意见1】 VR技术通过注意力分散、沉浸式多模态放松诱导、认知重构以及实时生物反馈与自我调节等多重核心机制协同作用,有效干预CRI。这些机制从心理和生理层面缓解患者的过度唤醒状态和非适应性认知,从而改善睡眠质量,构成一个有机整合的干预框架 | B | 强推荐 |
| 2 | 针对CRI,VR技术居家康复的推荐干预方案(包括内容、时长、频率、疗程)是什么? | 【推荐意见2】 针对CRI,VR技术居家康复可根据患者具体需求和情况,选择以下干预方案:VR自然场景模拟干预,推荐为1次/d,15~20 min/次,持续3~4周;VR引导的身心实践(如正念冥想与呼吸训练),推荐1次/d,30 min/次,持续6周;VR辅助的失眠认知行为疗法(CBT-I),推荐1~2次/d,15~30 min/次,持续3~6周;VR结合生物反馈(VR-BF),推荐1次/d,15~30 min/次,持续7~10 d或更长。这些方案各有侧重,共同为CRI患者提供了多样化的居家康复选择 | C | 弱推荐 |
| 3 | VR技术在CRI居家康复中的实施流程包括哪些步骤? | 【推荐意见3】 VR技术在CRI居家康复中的实施流程应包括干预前筛查评估、设备调试及干预、安全管理与监督、定期评估与调整4个核心阶段 | D | 强推荐 |
| 4 | 如何客观有效地评估VR技术居家康复对CRI的疗效?推荐使用哪些评价指标? | 【推荐意见4】 应采用主观与客观指标相结合、全面覆盖睡眠核心问题、共病症状及生活质量的多维度评价体系评估VR技术居家康复对CRI的疗效。推荐首选睡眠量表匹兹堡睡眠质量指数(PSQI)和失眠严重指数量表(ISI)进行初筛,警惕主观认知偏差;对于肿瘤的脆弱人群,推荐居家监测核心方案为"体动记录仪连续佩戴≥7 d+同步睡眠日记",前者客观追踪睡眠效率(SE)、觉醒时间(WASO)等参数,后者通过记录上床/起床时间及夜间症状等校准设备静卧误判;此组合可动态评估治疗反应,替代重复多导睡眠监测(PSG)。PSG作为睡眠医学诊断的金标准,建议对疑似器质性共病的CRI患者采用,但无法实现长期居家监测。此外,为全面了解VR干预的综合效果,还应结合共病症状量表[如患者健康问卷抑郁症状群量表(PHQ-9)、广泛性焦虑量表(GAD-7)、数字疼痛评分量表(NRS)、简明疲乏量表中文版(BFI-C)]和生活质量量表[如欧洲癌症研究与治疗组织生活质量核心问卷(EORTC QLQ-C30)]进行评估,以明确VR干预对患者整体身心健康和生活质量的改善 | A | 强推荐 |
| 5 | VR技术应用于CRI居家康复的安全性问题有哪些,应如何评估和管理? | 【推荐意见5】 VR技术应用于CRI居家康复时,需全面关注并管理其生理、心理社会及技术3方面的安全性风险。生理方面,应警惕晕动病、视觉系统负荷和心血管影响;针对晕动病,推荐通过虚拟现实晕动病问卷(CSQ-VR)及心率(HR)、心率变异性(HRV)等客观指标评估;针对视觉系统负荷,建议限制VR技术干预单次时长≤30 min,首次使用建议10 min,增加休息和眨眼并定期进行眼科检查;针对心血管系统影响,建议筛查基线血压、避免高频动态场景。心理社会方面,需警惕沉浸式环境可能加剧焦虑/抑郁或诱发创伤闪回,推荐VR技术干预前后使用医院焦虑抑郁量表(HADS)、PHQ-9、GAD-7等量表进行评估监测;建议照护者对患者进行密切监测,防范现实感混淆与社交回避问题。技术方面,应确保硬件符合安全规范,建议设备具备高分辨率(每只眼睛≥2 K)、高刷新率(90~120 Hz)、最小延迟(<45 ms)和宽视场角(中央≥60°,整体理想≥100°);并严格保护患者数据隐私,进行匿名化、加密、访问控制 | B | 强推荐 |
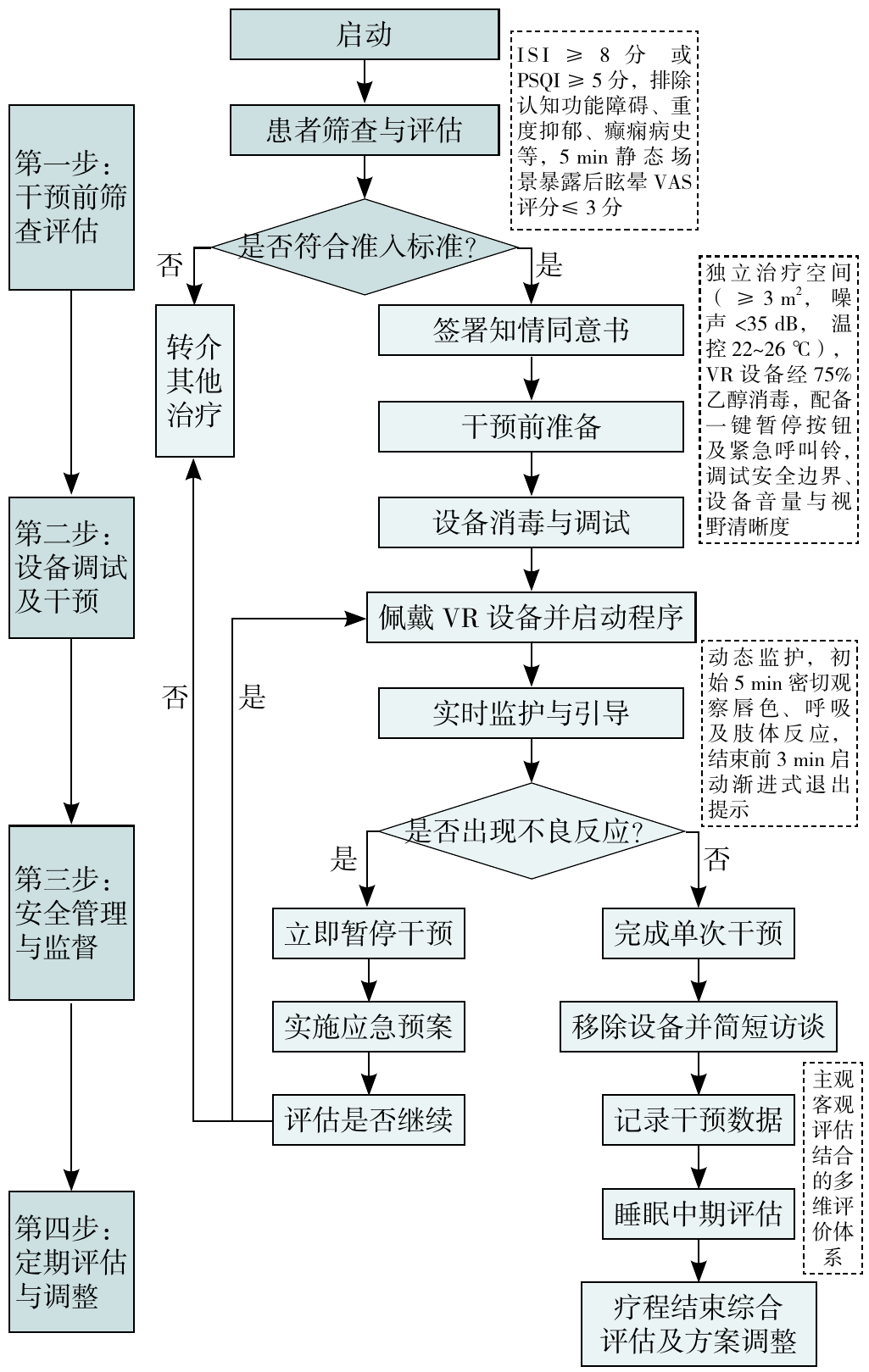
Figure 1 Flowchart of the implementation of virtual reality technology in home-based rehabilitation for cancer-related insomnia
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
贾杰. 积极推进全周期、多功能肿瘤康复[J]. 康复学报,2025,35(2):105-111.
|
| [9] | |
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] | |
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] | |
| [51] |
|
| [52] |
|
| [53] |
牟云平,王月莹,袁金金,等. 2018《AASM临床实践指南:使用体动记录仪评估睡眠障碍与昼夜节律睡眠-觉醒障碍》要点解读[J]. 上海护理,2022,22(6):1-5.
|
| [54] |
|
| [55] |
|
| [56] |
|
| [57] |
|
| [58] |
|
| [59] |
|
| [60] |
|
| [61] |
|
| [62] |
|
| [63] |
|
| [64] |
|
| [65] |
|
| [66] |
|
| [67] |
|
| [68] |
|
| [69] |
|
| [70] |
|
| [71] |
|
| [72] |
|
| [73] |
|
| [74] |
|
| [75] |
中国医学装备协会眼科专业委员会眼科检验检测学组联合中国医学装备协会眼科专业委员会眼科创新诊疗技术及装备学组. 虚拟现实与增强现实设备基于视觉健康使用的专家共识(2022)[J]. 中华眼科医学杂志(电子版),2022,(2):125-128. DOI:10.3877/cma.j.issn.2095-2007.2022.02.012.
|
| [76] |
|
| [77] |
|
| [78] |
|
| [79] |
|
| [80] |
|
| [81] |
|
| [82] |
|
| [83] |
|
| [1] | China Pharmacological Society Committee on Drug-induced Diseases. Expert Consensus on Medication Therapy for Acid-related Diseases [J]. Chinese General Practice, 2026, 29(19): 2593-2607. |
| [2] | General Practice Branch of Cross-straits Medicine Exchange Association, General Practice Branch of Zhejiang Medical Association, General Undifferentiated Disease Professional Committee of Zhejiang Society of Mathematical Medicine, Chinese Geriatrics Society. Expert Consensus on the Diagnosis, Treatment, and Management of Numbness (2025) [J]. Chinese General Practice, 2026, 29(18): 2433-2449. |
| [3] | Community Rehabilitation Working Committee of Chinese Rehabilitation Medicine Association. Chinese Expert Consensus on the Management of Home-based Rehabilitation for Cognitive Impairment (2026 Edition) [J]. Chinese General Practice, 2026, 29(14): 1793-1802. |
| [4] | YU Xuefang, ZHU Min, MA Qinglin, TAN Shenlang, WU Zixing, JIANG Wei. Clinical Efficacy of Chaihu Longgu Muli Decoction Combined with Cognitive Behavioral Therapy in the Treatment of Acute Insomnia of Liver Qi Stagnation with Fire Transformation Type [J]. Chinese General Practice, 2026, 29(13): 1666-1672. |
| [5] | WANG Gaoming, WANG Minghang, YANG Jiang, MENG Yuanyuan, ZHAO Di, DONG Xiaosheng. Systematic Evaluation and Reflection on the Quality of Bronchial Asthma Guidelines in China [J]. Chinese General Practice, 2026, 29(10): 1239-1245. |
| [6] | Chinese Geriatrics Society, National Clinical Research Center for Geriatric Diseases (Xuanwu Hospital). Chinese Expert Consensus on Screening and Comprehensive Assessment of Intrinsic Capacity in Older Adults [J]. Chinese General Practice, 2026, 29(10): 1225-1238. |
| [7] | Expert Panel of the Consensus on Artificial Intelligence Empowering Healthcare Services. Artificial Intelligence Empowering Healthcare Services: Expert Consensus from the Mangrove Health Conference in 2025 [J]. Chinese General Practice, 2026, 29(07): 817-822. |
| [8] | Institute for Healthy China, Tsinghua University, School of Public Health, Peking University, College of General Practice, Southern University of Science and Technology, Public Health Security and Health Professional Committee, Public Safety Science and Technology Society. Expert Consensus on Health Promotion Strategies for Adult Vaccination in China [J]. Chinese General Practice, 2026, 29(06): 681-687. |
| [9] | Psychosomatic Endocrinology Coordination Group of the Psychosomatic Medicine Society of the Chinese Medical Association, Diabetes Prevention and Control Committee of Chinese Preventive Medicine Association. Chinese Expert Consensus on the Diagnosis and Treatment of Diabetes Comorbid with Depression [J]. Chinese General Practice, 2026, 29(03): 273-292. |
| [10] | WU Hui, WANG Luya, LI Jialu, ZHANG Jun. Key Points Interpretation of Chinese Expert Consensus on Early Screening and Management of Homozygous Familial Hypercholesterolemia (2024) [J]. Chinese General Practice, 2025, 28(36): 4535-4540. |
| [11] | China Rehabilitation Science Institute, Community-Based Rehabilitation Committee of the China Association of Rehabilitation of Disabled Persons, Geriatric Rehabilitation Committee of Chinese Association of Geriatric Research, Guangdong Provincial People's Hospital (Guangdong Academy of Medical Sciences) /Southern Medical University, Guangzhou Association of Rehabilitation Medicine. Expert Consensus on Sarcopenia Screening in Community-dwelling Older Adults [J]. Chinese General Practice, 2025, 28(36): 4517-4534. |
| [12] | Community Rehabilitation Working Committee of Chinese Rehabilitation Medicine Association. Chinese Expert Consensus on Constipation Screening and Assessment for Community Cancer Patients (2025 Edition) [J]. Chinese General Practice, 2025, 28(34): 4249-4257. |
| [13] | Community Rehabilitation Working Committee of Chinese Rehabilitation Medicine Association. Chinese Expert Consensus on Community-based Cancer-related Fatigue Management (2025 Edition) [J]. Chinese General Practice, 2025, 28(33): 4117-4124. |
| [14] | General Practice Branch of Cross-Straits Medicine Exchange Association, General Practice Branch of Zhejiang Medical Association, General Undifferentiated Disease Professional Committee of Zhejiang Society of Mathematical Medicine, the Expert Collaboration Group on Medically Unspecified Disease in General Practice, Chinese Geriatrics Society. Expert Consensus on the Diagnosis, Treatment, and Management of Edema (2025) [J]. Chinese General Practice, 2025, 28(31): 3861-3878. |
| [15] | Community Rehabilitation Working Committee of Chinese Rehabilitation Medical Association. Chinese Expert Consensus on Sleep Health and Rehabilitation Management for Community-dwelling Older Adults (2025 Edition) [J]. Chinese General Practice, 2025, 28(29): 3608-3618. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||