
Chinese General Practice ›› 2025, Vol. 28 ›› Issue (09): 1072-1083.DOI: 10.12114/j.issn.1007-9572.2024.0016
Special Issue: 内分泌代谢性疾病最新文章合辑
• Original Research • Previous Articles Next Articles
Received:2024-01-20
Revised:2024-06-10
Published:2025-03-20
Online:2025-01-02
Contact:
DENG Tingting
通讯作者:
邓婷婷
作者简介:作者贡献:
曾佳玲提出主要研究目标,负责研究的构思与设计,研究的实施,撰写论文;曾佳玲、蒙艳进行数据的收集与整理,统计学处理,图、表的绘制与展示;邓婷婷负责文章的质量控制与审查,对文章整体负责,监督管理;李锦华、赵萍负责论文的修订。
基金资助:CLC Number:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2024.0016
| 组别 | 例数 | 性别(男/女) | 甲状腺结节[例(%)] | 年龄(岁) | 住院天数(d) | 身高(cm) | 体质量(kg) | BMI(kg/m2) | 腰围(cm) | 臀围(cm) | 腰臀比 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| NAFLD组 | 293 | 125/168 | 183(62.46) | 57.0±12.8 | 8.14±2.46 | 161.36±8.46 | 72.37±14.84 | 27.64±4.30 | 89.51±11.48 | 101.32±8.76 | 0.88±0.06 |
| 非NAFLD组 | 285 | 122/163 | 176(61.75) | 59.3±11.6 | 8.43±3.22 | 160.12±7.94 | 63.12±13.69 | 24.46±4.12 | 80.94±11.64 | 94.30±10.49 | 0.87±0.24 |
| 检验统计量值 | 0.010a | 0.030a | -2.248 | -1.223 | 1.807 | 7.784 | 9.069 | 8.919 | 8.764 | 1.005 | |
| P值 | 0.972 | 0.862 | 0.025 | 0.222 | 0.072 | <0.001 | <0.001 | <0.001 | <0.001 | 0.315 | |
| 组别 | 收缩压(mmHg) | 舒张压(mmHg) | VFA(cm2) | SFA(cm2) | 甲状腺最大结节面积[M(P25,P75),mm2] | HbA1c(%) | FPG(mmol/L) | FINS[M(P25,P75),pmol/L] | FCP[M(P25,P75),nmol/L] | ||
| NAFLD组 | 137±21 | 79±13 | 118.25±37.81 | 234.51±158.21 | 70(20,210) | 10.27±2.61 | 7.94±2.57 | 67.5(36.8,109.2) | 0.72(0.50,1.02) | ||
| 非NAFLD组 | 141±73 | 78±12 | 84.69±37.28 | 174.79±64.42 | 65(20,230) | 9.56±2.71 | 7.96±2.46 | 47.0(25.7,90.0) | 0.59(0.36,0.96) | ||
| 检验统计量值 | -0.815 | 1.059 | 10.744 | 5.914 | -0.067b | 3.200 | -0.108 | -3.448b | -3.476b | ||
| P值 | 0.415 | 0.290 | <0.001 | <0.001 | 0.947 | 0.001 | 0.914 | 0.001 | 0.001 | ||
| 组别 | HOMA-IR | HOMA-β[M(P25,P75)] | TSH[M(P25,P75),mU/L] | TT3(nmol/L) | TT4(nmol/L) | FT3(pmol/L) | FT4(pmol/L) | 甲状腺球蛋白[M(P25,P75),mg/L] | |||
| NAFLD组 | 3.83±1.54 | 50.20(29.87,78.01) | 1.680(0.890,2.900) | 1.49±0.49 | 92.55±21.27 | 4.27±1.51 | 15.60±2.84 | 12.91(6.02,34.40) | |||
| 非NAFLD组 | 3.53±1.52 | 41.75(24.91,65.37) | 1.710(0.975,4.055) | 1.44±0.52 | 92.88±22.90 | 4.00±1.29 | 15.87±3.15 | 15.23(5.54,37.96) | |||
| 检验统计量值 | 2.384 | -3.006b | -0.959b | 1.354 | -0.181 | 2.289 | -1.074 | -0.269b | |||
| P值 | 0.017 | 0.003 | 0.337 | 0.176 | 0.856 | 0.022 | 0.283 | 0.788 | |||
| 组别 | 球蛋白抗体[M(P25,P75),mg/L] | 过氧化物酶抗体[M(P25,P75),mg/L] | SCr(μmol/L) | SUA(μmol/L) | TC(mmol/L) | TG[M(P25,P75),mmol/L] | LDL-C(mmol/L) | HDL-C(mmol/L) | 同型半胱氨酸(μmol/L) | ||
| NAFLD组 | 16.36(12.18,75.63) | 17.00(11.05,41.35) | 73.41±25.27 | 353.47±99.26 | 4.92±1.71 | 2.59(1.56,4.11) | 2.83±1.10 | 1.05±0.91 | 12.01±4.87 | ||
| 非NAFLD组 | 14.90(12.30,73.40) | 15.05(10.90,27.10) | 82.24±52.04 | 325.90±115.17 | 4.57±1.28 | 1.51(1.03,2.36) | 2.73±0.98 | 1.15±0.39 | 12.71±4.45 | ||
| 检验统计量值 | -0.558b | -0.831b | -2.572 | 3.076 | 2.773 | -8.130 | 1.142 | -1.695 | -1.711 | ||
| P值 | 0.577 | 0.406 | 0.010 | 0.002 | 0.006 | <0.001 | 0.254 | 0.091 | 0.088 | ||
| 组别 | CRP[M(P25,P75),mg/L] | 红细胞沉降率[M(P25,P75),mm/h] | ALT[M(P25,P75),U/L] | AST[M(P25,P75),U/L] | ALP(U/L) | 白细胞计数(×109/L) | 中性粒细胞计数(×109/L) | 淋巴细胞计数(×109/L) | 单核细胞计数(×109/L) | 中性粒百分比(%) | 血小板计数(×109/L) |
| NAFLD组 | 3.25(1.84,6.27) | 40(18,58) | 18(14,30) | 19(13,27) | 86.47±28.14 | 7.28±2.12 | 4.48±1.76 | 2.06±0.78 | 0.54±0.20 | 60.49±9.44 | 249.45±67.86 |
| 非NAFLD组 | 2.55(0.95,7.20) | 41(22,89) | 25(13,37) | 19(12,31) | 92.21±43.77 | 7.91±1.98 | 4.88±1.65 | 2.21±0.81 | 0.58±0.21 | 61.02±9.56 | 260.68±71.97 |
| 检验统计量值 | -2.288b | -1.563b | -0.28b | -0.020b | -0.582 | -1.263 | -0.966 | -0.776 | -0.896 | -0.232 | -0.663 |
| P值 | 0.022 | 0.118 | 0.530 | 0.984 | 0.565 | 0.210 | 0.337 | 0.440 | 0.373 | 0.817 | 0.511 |
Table 1 Comparison of clinical examination indexes between NAFLD group and non-NAFLD group
| 组别 | 例数 | 性别(男/女) | 甲状腺结节[例(%)] | 年龄(岁) | 住院天数(d) | 身高(cm) | 体质量(kg) | BMI(kg/m2) | 腰围(cm) | 臀围(cm) | 腰臀比 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| NAFLD组 | 293 | 125/168 | 183(62.46) | 57.0±12.8 | 8.14±2.46 | 161.36±8.46 | 72.37±14.84 | 27.64±4.30 | 89.51±11.48 | 101.32±8.76 | 0.88±0.06 |
| 非NAFLD组 | 285 | 122/163 | 176(61.75) | 59.3±11.6 | 8.43±3.22 | 160.12±7.94 | 63.12±13.69 | 24.46±4.12 | 80.94±11.64 | 94.30±10.49 | 0.87±0.24 |
| 检验统计量值 | 0.010a | 0.030a | -2.248 | -1.223 | 1.807 | 7.784 | 9.069 | 8.919 | 8.764 | 1.005 | |
| P值 | 0.972 | 0.862 | 0.025 | 0.222 | 0.072 | <0.001 | <0.001 | <0.001 | <0.001 | 0.315 | |
| 组别 | 收缩压(mmHg) | 舒张压(mmHg) | VFA(cm2) | SFA(cm2) | 甲状腺最大结节面积[M(P25,P75),mm2] | HbA1c(%) | FPG(mmol/L) | FINS[M(P25,P75),pmol/L] | FCP[M(P25,P75),nmol/L] | ||
| NAFLD组 | 137±21 | 79±13 | 118.25±37.81 | 234.51±158.21 | 70(20,210) | 10.27±2.61 | 7.94±2.57 | 67.5(36.8,109.2) | 0.72(0.50,1.02) | ||
| 非NAFLD组 | 141±73 | 78±12 | 84.69±37.28 | 174.79±64.42 | 65(20,230) | 9.56±2.71 | 7.96±2.46 | 47.0(25.7,90.0) | 0.59(0.36,0.96) | ||
| 检验统计量值 | -0.815 | 1.059 | 10.744 | 5.914 | -0.067b | 3.200 | -0.108 | -3.448b | -3.476b | ||
| P值 | 0.415 | 0.290 | <0.001 | <0.001 | 0.947 | 0.001 | 0.914 | 0.001 | 0.001 | ||
| 组别 | HOMA-IR | HOMA-β[M(P25,P75)] | TSH[M(P25,P75),mU/L] | TT3(nmol/L) | TT4(nmol/L) | FT3(pmol/L) | FT4(pmol/L) | 甲状腺球蛋白[M(P25,P75),mg/L] | |||
| NAFLD组 | 3.83±1.54 | 50.20(29.87,78.01) | 1.680(0.890,2.900) | 1.49±0.49 | 92.55±21.27 | 4.27±1.51 | 15.60±2.84 | 12.91(6.02,34.40) | |||
| 非NAFLD组 | 3.53±1.52 | 41.75(24.91,65.37) | 1.710(0.975,4.055) | 1.44±0.52 | 92.88±22.90 | 4.00±1.29 | 15.87±3.15 | 15.23(5.54,37.96) | |||
| 检验统计量值 | 2.384 | -3.006b | -0.959b | 1.354 | -0.181 | 2.289 | -1.074 | -0.269b | |||
| P值 | 0.017 | 0.003 | 0.337 | 0.176 | 0.856 | 0.022 | 0.283 | 0.788 | |||
| 组别 | 球蛋白抗体[M(P25,P75),mg/L] | 过氧化物酶抗体[M(P25,P75),mg/L] | SCr(μmol/L) | SUA(μmol/L) | TC(mmol/L) | TG[M(P25,P75),mmol/L] | LDL-C(mmol/L) | HDL-C(mmol/L) | 同型半胱氨酸(μmol/L) | ||
| NAFLD组 | 16.36(12.18,75.63) | 17.00(11.05,41.35) | 73.41±25.27 | 353.47±99.26 | 4.92±1.71 | 2.59(1.56,4.11) | 2.83±1.10 | 1.05±0.91 | 12.01±4.87 | ||
| 非NAFLD组 | 14.90(12.30,73.40) | 15.05(10.90,27.10) | 82.24±52.04 | 325.90±115.17 | 4.57±1.28 | 1.51(1.03,2.36) | 2.73±0.98 | 1.15±0.39 | 12.71±4.45 | ||
| 检验统计量值 | -0.558b | -0.831b | -2.572 | 3.076 | 2.773 | -8.130 | 1.142 | -1.695 | -1.711 | ||
| P值 | 0.577 | 0.406 | 0.010 | 0.002 | 0.006 | <0.001 | 0.254 | 0.091 | 0.088 | ||
| 组别 | CRP[M(P25,P75),mg/L] | 红细胞沉降率[M(P25,P75),mm/h] | ALT[M(P25,P75),U/L] | AST[M(P25,P75),U/L] | ALP(U/L) | 白细胞计数(×109/L) | 中性粒细胞计数(×109/L) | 淋巴细胞计数(×109/L) | 单核细胞计数(×109/L) | 中性粒百分比(%) | 血小板计数(×109/L) |
| NAFLD组 | 3.25(1.84,6.27) | 40(18,58) | 18(14,30) | 19(13,27) | 86.47±28.14 | 7.28±2.12 | 4.48±1.76 | 2.06±0.78 | 0.54±0.20 | 60.49±9.44 | 249.45±67.86 |
| 非NAFLD组 | 2.55(0.95,7.20) | 41(22,89) | 25(13,37) | 19(12,31) | 92.21±43.77 | 7.91±1.98 | 4.88±1.65 | 2.21±0.81 | 0.58±0.21 | 61.02±9.56 | 260.68±71.97 |
| 检验统计量值 | -2.288b | -1.563b | -0.28b | -0.020b | -0.582 | -1.263 | -0.966 | -0.776 | -0.896 | -0.232 | -0.663 |
| P值 | 0.022 | 0.118 | 0.530 | 0.984 | 0.565 | 0.210 | 0.337 | 0.440 | 0.373 | 0.817 | 0.511 |
| 组别 | 例数 | 性别(男/女) | 年龄(岁) | 甲状腺结节[例(%)] | NAFLD[例(%)] |
|---|---|---|---|---|---|
| 内脏性肥胖组 | 251 | 127/124 | 55.3±13.4 | 163(64.94) | 180(71.71) |
| 非内脏性肥胖组 | 327 | 120/207 | 60.3±10.8 | 195(59.63) | 114(34.86) |
| t(χ2)值 | 11.212a | -4.940 | 1.581a | 77.157a | |
| P值 | 0.001 | <0.001 | 0.209 | <0.001 |
Table 2 Comparison of age,sex,prevalence of thyroid nodules and NAFLD in the visceral obesity group and the non-visceral obesity group
| 组别 | 例数 | 性别(男/女) | 年龄(岁) | 甲状腺结节[例(%)] | NAFLD[例(%)] |
|---|---|---|---|---|---|
| 内脏性肥胖组 | 251 | 127/124 | 55.3±13.4 | 163(64.94) | 180(71.71) |
| 非内脏性肥胖组 | 327 | 120/207 | 60.3±10.8 | 195(59.63) | 114(34.86) |
| t(χ2)值 | 11.212a | -4.940 | 1.581a | 77.157a | |
| P值 | 0.001 | <0.001 | 0.209 | <0.001 |
| 项目 | rs值 | P值 |
|---|---|---|
| 性别 | 0.004 | 0.915 |
| 年龄 | -0.083 | 0.046 |
| 体质量 | 0.315 | <0.001 |
| BMI | 0.354 | <0.001 |
| 腰围 | 0.353 | <0.001 |
| 臀围 | 0.356 | <0.001 |
| 腰臀比 | 0.223 | <0.001 |
| VFA | 0.445 | <0.001 |
| SFA | 0.403 | <0.001 |
| 甲状腺结节 | 0.003 | 0.946 |
| 最大结节面积 | -0.004 | 0.967 |
| HbA1c | 0.144 | 0.001 |
| FINS | 0.145 | <0.001 |
| FCP | 0.134 | 0.001 |
| HOMA-IR | 0.119 | 0.004 |
| HOMA-β | 0.117 | 0.005 |
| TSH | -0.041 | 0.326 |
| TT3 | 0.103 | 0.013 |
| TT4 | -0.010 | 0.816 |
| FT3 | 0.128 | 0.002 |
| FT4 | -0.039 | 0.345 |
| CRP | 0.096 | 0.030 |
Table 3 The Spearman's correlation analysis of clinical indexes with NAFLD in T2DM patients
| 项目 | rs值 | P值 |
|---|---|---|
| 性别 | 0.004 | 0.915 |
| 年龄 | -0.083 | 0.046 |
| 体质量 | 0.315 | <0.001 |
| BMI | 0.354 | <0.001 |
| 腰围 | 0.353 | <0.001 |
| 臀围 | 0.356 | <0.001 |
| 腰臀比 | 0.223 | <0.001 |
| VFA | 0.445 | <0.001 |
| SFA | 0.403 | <0.001 |
| 甲状腺结节 | 0.003 | 0.946 |
| 最大结节面积 | -0.004 | 0.967 |
| HbA1c | 0.144 | 0.001 |
| FINS | 0.145 | <0.001 |
| FCP | 0.134 | 0.001 |
| HOMA-IR | 0.119 | 0.004 |
| HOMA-β | 0.117 | 0.005 |
| TSH | -0.041 | 0.326 |
| TT3 | 0.103 | 0.013 |
| TT4 | -0.010 | 0.816 |
| FT3 | 0.128 | 0.002 |
| FT4 | -0.039 | 0.345 |
| CRP | 0.096 | 0.030 |
| 相关因素 | rs值 | P值 |
|---|---|---|
| 性别(1=男,2=女) | -0.217 | <0.001 |
| 年龄 | -0.166 | <0.001 |
| 身高 | 0.305 | <0.001 |
| 体质量 | 0.767 | <0.001 |
| BMI | 0.778 | <0.001 |
| 腰围 | 0.781 | <0.001 |
| 臀围 | 0.687 | <0.001 |
| 腰臀比 | 0.640 | <0.001 |
| SFA | 0.715 | <0.001 |
| 舒张压 | 0.115 | 0.006 |
| FINS | 0.266 | <0.001 |
| FCP | 0.245 | <0.001 |
| HOMA-IR | 0.266 | <0.001 |
| HOMA-β | 0.248 | <0.001 |
| TSH | -0.022 | 0.592 |
| TT3 | 0.108 | 0.010 |
| TT4 | 0.004 | 0.931 |
| FT3 | 0.142 | 0.001 |
| FT4 | 0.021 | 0.617 |
| UA | 0.358 | <0.001 |
| TG | 0.345 | <0.001 |
| CRP | 0.176 | <0.001 |
| 红细胞沉降率 | -0.160 | 0.076 |
| NAFLD | 0.445 | <0.001 |
| 甲状腺结节 | 0.032 | 0.438 |
| 结节面积大小 | 0.008 | 0.892 |
| 吸烟 | 0.056 | 0.204 |
Table 4 Spearman's correlation analysis between visceral obesity and other clinical indicators in T2DM patients
| 相关因素 | rs值 | P值 |
|---|---|---|
| 性别(1=男,2=女) | -0.217 | <0.001 |
| 年龄 | -0.166 | <0.001 |
| 身高 | 0.305 | <0.001 |
| 体质量 | 0.767 | <0.001 |
| BMI | 0.778 | <0.001 |
| 腰围 | 0.781 | <0.001 |
| 臀围 | 0.687 | <0.001 |
| 腰臀比 | 0.640 | <0.001 |
| SFA | 0.715 | <0.001 |
| 舒张压 | 0.115 | 0.006 |
| FINS | 0.266 | <0.001 |
| FCP | 0.245 | <0.001 |
| HOMA-IR | 0.266 | <0.001 |
| HOMA-β | 0.248 | <0.001 |
| TSH | -0.022 | 0.592 |
| TT3 | 0.108 | 0.010 |
| TT4 | 0.004 | 0.931 |
| FT3 | 0.142 | 0.001 |
| FT4 | 0.021 | 0.617 |
| UA | 0.358 | <0.001 |
| TG | 0.345 | <0.001 |
| CRP | 0.176 | <0.001 |
| 红细胞沉降率 | -0.160 | 0.076 |
| NAFLD | 0.445 | <0.001 |
| 甲状腺结节 | 0.032 | 0.438 |
| 结节面积大小 | 0.008 | 0.892 |
| 吸烟 | 0.056 | 0.204 |
| 相关因素 | rs值 | P值 |
|---|---|---|
| 性别(1=男,2=女) | 0.212 | <0.001 |
| 年龄 | 0.187 | 0.002 |
| 身高 | -0.127 | 0.038 |
| 腰臀比 | -0.138 | 0.024 |
| TSH | -0.322 | <0.001 |
| TT3 | 0.158 | 0.010 |
| TT4 | 0.211 | <0.001 |
| 甲状腺球蛋白 | 0.260 | 0.022 |
Table 5 Spearman's correlation analysis between thyroid nodule area and clinical indicators in T2DM patients
| 相关因素 | rs值 | P值 |
|---|---|---|
| 性别(1=男,2=女) | 0.212 | <0.001 |
| 年龄 | 0.187 | 0.002 |
| 身高 | -0.127 | 0.038 |
| 腰臀比 | -0.138 | 0.024 |
| TSH | -0.322 | <0.001 |
| TT3 | 0.158 | 0.010 |
| TT4 | 0.211 | <0.001 |
| 甲状腺球蛋白 | 0.260 | 0.022 |
| 相关因素 | 回归系数 | 标准误 | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 年龄 | -0.015 | 0.007 | 5.061 | 0.024 | 0.985(0.971~0.998) |
| 体质量 | 0.046 | 0.007 | 48.235 | <0.001 | 1.047(1.034~1.061) |
| BMI | 0.182 | 0.023 | 61.917 | <0.001 | 1.200(1.146~1.255) |
| 腰围 | 0.066 | 0.009 | 59.164 | <0.001 | 1.068(1.050~1.086) |
| 臀围 | 0.081 | 0.011 | 59.463 | <0.001 | 1.085(1.063~1.108) |
| VFA | 0.019 | 0.004 | 26.666 | <0.001 | 1.019(1.012~1.026) |
| SFA | 0.005 | 0.002 | 5.691 | 0.017 | 1.005(1.001~1.009) |
| HbA1c | 0.103 | 0.032 | 10.261 | 0.001 | 1.108(1.041~1.180) |
| FCP | 0.595 | 0.204 | 8.516 | 0.004 | 1.814(1.216~2.705) |
| HOMA-IR | 0.129 | 0.056 | 5.262 | 0.022 | 1.137(1.019~1.269) |
| FT3 | 0.167 | 0.075 | 4.913 | 0.027 | 1.182(1.020~1.370) |
| SCr | -0.006 | 0.003 | 6.355 | 0.012 | 0.994(0.989~0.999) |
| SUA | 0.002 | 0.001 | 8.550 | 0.003 | 1.002(1.001~1.004) |
| TC | 0.158 | 0.060 | 6.900 | 0.009 | 1.172(1.041~1.319) |
| TG | 0.201 | 0.044 | 20.818 | <0.001 | 1.223(1.122~1.333) |
Table 6 Univariate unconditional Logistic regression analysis of influencing factors for NAFLD in T2DM patients
| 相关因素 | 回归系数 | 标准误 | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 年龄 | -0.015 | 0.007 | 5.061 | 0.024 | 0.985(0.971~0.998) |
| 体质量 | 0.046 | 0.007 | 48.235 | <0.001 | 1.047(1.034~1.061) |
| BMI | 0.182 | 0.023 | 61.917 | <0.001 | 1.200(1.146~1.255) |
| 腰围 | 0.066 | 0.009 | 59.164 | <0.001 | 1.068(1.050~1.086) |
| 臀围 | 0.081 | 0.011 | 59.463 | <0.001 | 1.085(1.063~1.108) |
| VFA | 0.019 | 0.004 | 26.666 | <0.001 | 1.019(1.012~1.026) |
| SFA | 0.005 | 0.002 | 5.691 | 0.017 | 1.005(1.001~1.009) |
| HbA1c | 0.103 | 0.032 | 10.261 | 0.001 | 1.108(1.041~1.180) |
| FCP | 0.595 | 0.204 | 8.516 | 0.004 | 1.814(1.216~2.705) |
| HOMA-IR | 0.129 | 0.056 | 5.262 | 0.022 | 1.137(1.019~1.269) |
| FT3 | 0.167 | 0.075 | 4.913 | 0.027 | 1.182(1.020~1.370) |
| SCr | -0.006 | 0.003 | 6.355 | 0.012 | 0.994(0.989~0.999) |
| SUA | 0.002 | 0.001 | 8.550 | 0.003 | 1.002(1.001~1.004) |
| TC | 0.158 | 0.060 | 6.900 | 0.009 | 1.172(1.041~1.319) |
| TG | 0.201 | 0.044 | 20.818 | <0.001 | 1.223(1.122~1.333) |
| 相关因素 | 回归系数 | 标准误 | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 体质量 | -0.039 | 0.017 | 5.015 | 0.025 | 0.962(0.929~0.995) |
| VFA | 0.025 | 0.005 | 27.862 | <0.001 | 1.025(1.016~1.035) |
| SFA | 0.006 | 0.003 | 3.942 | 0.047 | 1.006(1.000~1.011) |
| FT3 | 0.357 | 0.145 | 6.104 | 0.013 | 1.429(1.077~1.897) |
| HOMA-IR | 0.131 | 0.064 | 4.146 | 0.042 | 1.140(1.005~1.293) |
Table 7 Binary Logistic regression analysis of influencing factors for NAFLD in T2DM patients
| 相关因素 | 回归系数 | 标准误 | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 体质量 | -0.039 | 0.017 | 5.015 | 0.025 | 0.962(0.929~0.995) |
| VFA | 0.025 | 0.005 | 27.862 | <0.001 | 1.025(1.016~1.035) |
| SFA | 0.006 | 0.003 | 3.942 | 0.047 | 1.006(1.000~1.011) |
| FT3 | 0.357 | 0.145 | 6.104 | 0.013 | 1.429(1.077~1.897) |
| HOMA-IR | 0.131 | 0.064 | 4.146 | 0.042 | 1.140(1.005~1.293) |
| 相关因素 | 回归系数 | 标准误 | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 女性 | -1.074 | 0.481 | 4.996 | 0.025 | 0.342(0.133~0.876) |
| 年龄 | 0.071 | 0.017 | 16.460 | <0.001 | 1.073(1.037~1.110) |
| 身高 | 0.013 | 0.038 | 0.126 | 0.723 | 1.013(0.941~1.091) |
| 体质量 | -0.001 | 0.015 | 0.004 | 0.948 | 0.999(0.970~1.029) |
| FT4 | 0.131 | 0.055 | 5.641 | 0.018 | 1.140(1.023~1.269) |
| 甲状腺球蛋白 | 0.002 | 0.003 | 0.318 | 0.573 | 1.002(0.996~1.007) |
| HDL-C | 0.872 | 0.549 | 2.525 | 0.112 | 2.391(0.816~7.009) |
Table 8 Binary Logistic regression of risk factors for thyroid nodules in T2DM patients
| 相关因素 | 回归系数 | 标准误 | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| 女性 | -1.074 | 0.481 | 4.996 | 0.025 | 0.342(0.133~0.876) |
| 年龄 | 0.071 | 0.017 | 16.460 | <0.001 | 1.073(1.037~1.110) |
| 身高 | 0.013 | 0.038 | 0.126 | 0.723 | 1.013(0.941~1.091) |
| 体质量 | -0.001 | 0.015 | 0.004 | 0.948 | 0.999(0.970~1.029) |
| FT4 | 0.131 | 0.055 | 5.641 | 0.018 | 1.140(1.023~1.269) |
| 甲状腺球蛋白 | 0.002 | 0.003 | 0.318 | 0.573 | 1.002(0.996~1.007) |
| HDL-C | 0.872 | 0.549 | 2.525 | 0.112 | 2.391(0.816~7.009) |
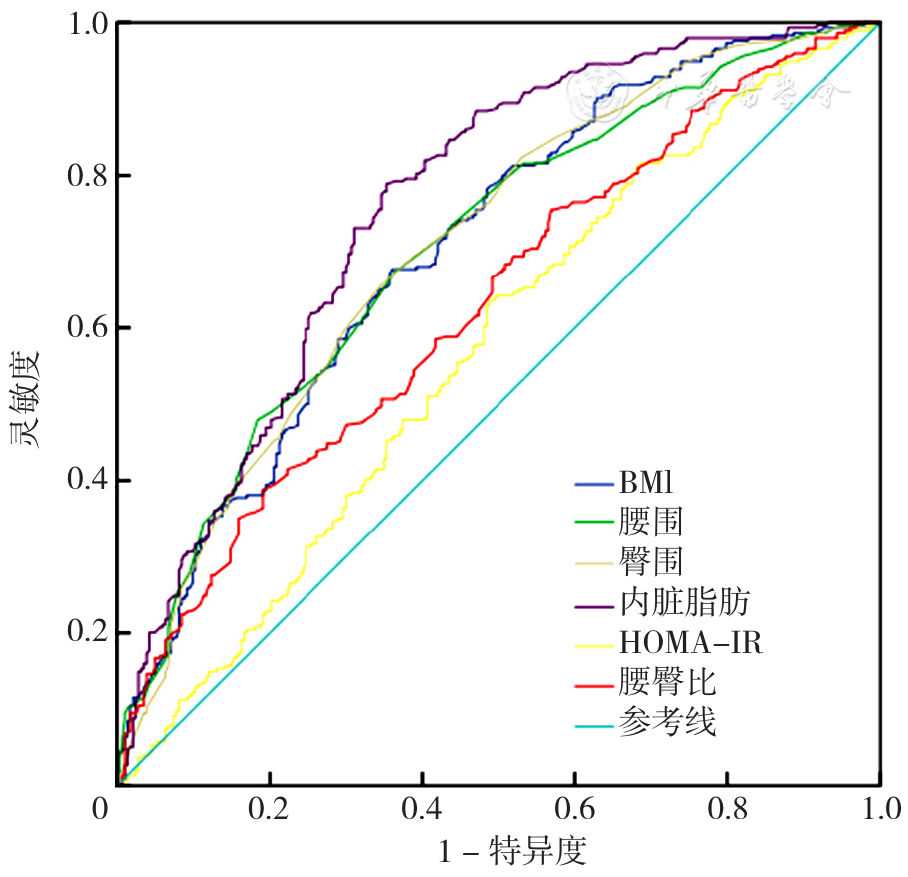
Figure 1 ROC assessed the predictive value of clinical indicators in NAFLD in T2DM patients
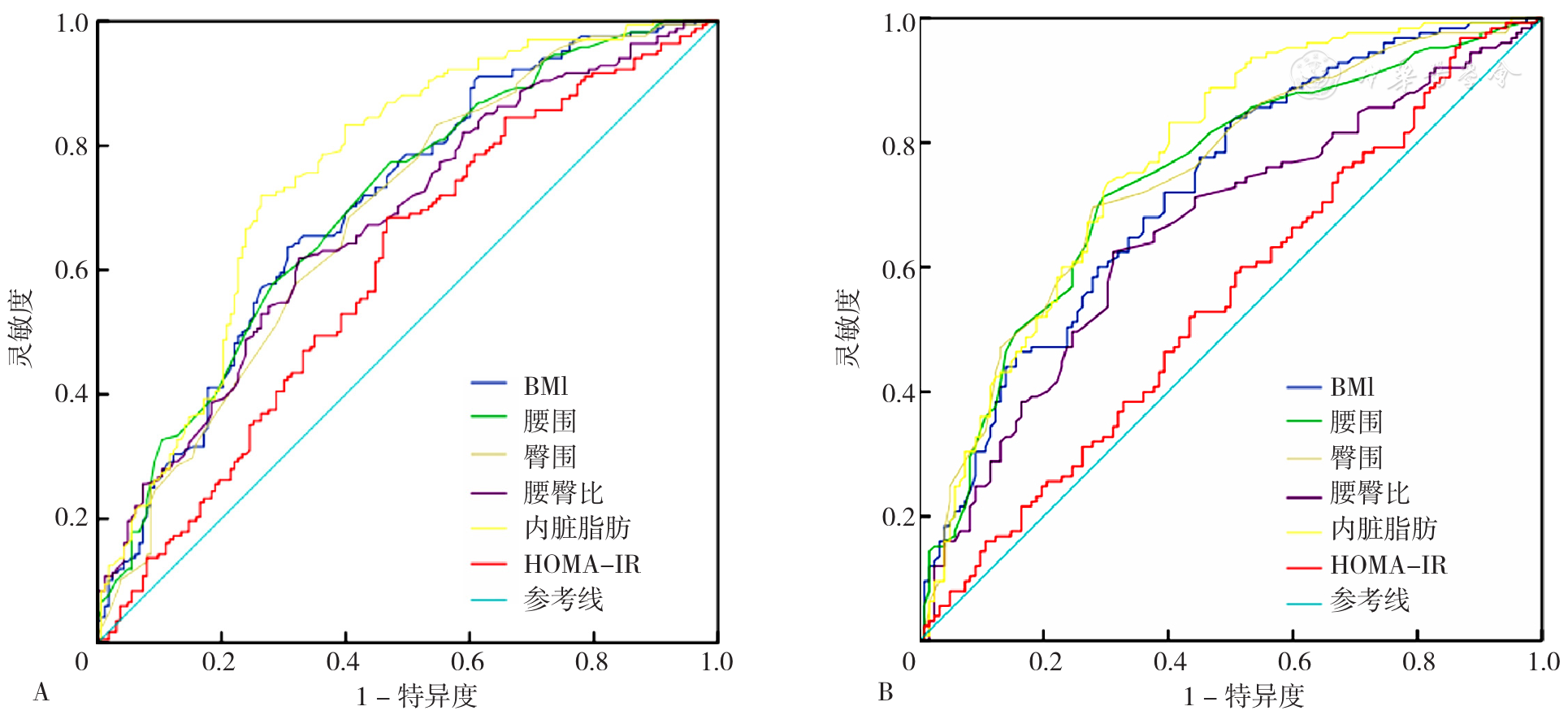
Figure 2 ROC curves of clinical indicators in predicting NAFLD in female and male T2DM patients
| 指标 | AUC(95%CI) | P值 | 灵敏度(%) | 特异度(%) | 最佳截断值 |
|---|---|---|---|---|---|
| BMI | 0.704(0.662~0.746) | <0.001 | 67.7 | 36.0 | 25.37 kg/m2 |
| 腰围 | 0.704(0.662~0.746) | <0.001 | 67.3 | 36.4 | 84.5 cm |
| 臀围 | 0.705(0.663~0.747) | <0.001 | 69.4 | 38.9 | 96.5 cm |
| 腰臀比 | 0.629(0.584~0.674) | <0.001 | 38.8 | 19.1 | 0.895 |
| VFA | 0.757(0.718~0.797) | <0.001 | 78.9 | 35.3 | 88.40 cm2 |
| HOMA-IR | 0.569(0.522~0.616) | 0.004 | 64.3 | 49.8 | 3.08 |
Table 9 Predictive values of clinical indicators in NAFLD in T2DM patients
| 指标 | AUC(95%CI) | P值 | 灵敏度(%) | 特异度(%) | 最佳截断值 |
|---|---|---|---|---|---|
| BMI | 0.704(0.662~0.746) | <0.001 | 67.7 | 36.0 | 25.37 kg/m2 |
| 腰围 | 0.704(0.662~0.746) | <0.001 | 67.3 | 36.4 | 84.5 cm |
| 臀围 | 0.705(0.663~0.747) | <0.001 | 69.4 | 38.9 | 96.5 cm |
| 腰臀比 | 0.629(0.584~0.674) | <0.001 | 38.8 | 19.1 | 0.895 |
| VFA | 0.757(0.718~0.797) | <0.001 | 78.9 | 35.3 | 88.40 cm2 |
| HOMA-IR | 0.569(0.522~0.616) | 0.004 | 64.3 | 49.8 | 3.08 |
| 指标 | AUC(95%CI) | P值 | 灵敏度(%) | 特异度(%) | 截断值 |
|---|---|---|---|---|---|
| BMI | 0.704(0.662~0.746) | <0.001 | 63.3 | 30.9 | 25.695 kg/m2 |
| 腰围 | 0.704(0.662~0.746) | <0.001 | 76.9 | 47.5 | 81.5 cm |
| 臀围 | 0.705(0.663~0.747) | <0.001 | 82.8 | 54.9 | 94.5 cm |
| 腰臀比 | 0.629(0.584~0.674) | <0.001 | 61.5 | 32.7 | 0.849 |
| VFA | 0.757(0.718~0.797) | <0.001 | 71.6 | 26.5 | 88.40 cm2 |
| HOMA-IR | 0.569(0.522~0.616) | 0.004 | 68.0 | 46.9 | 3.13 |
Table 10 Predictive values of clinical indicators in NAFLD in female T2DM patients
| 指标 | AUC(95%CI) | P值 | 灵敏度(%) | 特异度(%) | 截断值 |
|---|---|---|---|---|---|
| BMI | 0.704(0.662~0.746) | <0.001 | 63.3 | 30.9 | 25.695 kg/m2 |
| 腰围 | 0.704(0.662~0.746) | <0.001 | 76.9 | 47.5 | 81.5 cm |
| 臀围 | 0.705(0.663~0.747) | <0.001 | 82.8 | 54.9 | 94.5 cm |
| 腰臀比 | 0.629(0.584~0.674) | <0.001 | 61.5 | 32.7 | 0.849 |
| VFA | 0.757(0.718~0.797) | <0.001 | 71.6 | 26.5 | 88.40 cm2 |
| HOMA-IR | 0.569(0.522~0.616) | 0.004 | 68.0 | 46.9 | 3.13 |
| 指标 | AUC(95%CI) | P值 | 灵敏度(%) | 特异度(%) | 截断值 |
|---|---|---|---|---|---|
| BMI | 0.722(0.660~0.785) | <0.001 | 84.0 | 50.8 | 24.06 kg/m2 |
| 腰围 | 0.739(0.677~0.801) | <0.001 | 71.2 | 29.5 | 87.5 cm |
| 臀围 | 0.743(0.682~0.805) | <0.001 | 69.6 | 27.9 | 97.5 cm |
| 腰臀比 | 0.657(0.589~0.725) | <0.001 | 62.4 | 31.1 | 0.897 |
| VFA | 0.771(0.712~0.829) | <0.001 | 73.6 | 30.3 | 99.45 cm2 |
| HOMA-IR | 0.546(0.474~0.618) | 0.214 | 52.0 | 43.4 | 3.35 |
Table 11 Predictive values of clinical indicators in NAFLD in male T2DM patients
| 指标 | AUC(95%CI) | P值 | 灵敏度(%) | 特异度(%) | 截断值 |
|---|---|---|---|---|---|
| BMI | 0.722(0.660~0.785) | <0.001 | 84.0 | 50.8 | 24.06 kg/m2 |
| 腰围 | 0.739(0.677~0.801) | <0.001 | 71.2 | 29.5 | 87.5 cm |
| 臀围 | 0.743(0.682~0.805) | <0.001 | 69.6 | 27.9 | 97.5 cm |
| 腰臀比 | 0.657(0.589~0.725) | <0.001 | 62.4 | 31.1 | 0.897 |
| VFA | 0.771(0.712~0.829) | <0.001 | 73.6 | 30.3 | 99.45 cm2 |
| HOMA-IR | 0.546(0.474~0.618) | 0.214 | 52.0 | 43.4 | 3.35 |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
程梦凡,吴乃君,王雪莲. 2型糖尿病合并非酒精性脂肪肝患者内脏脂肪指数相关研究[J]. 华北理工大学学报(医学版),2020,22(3):173-177. DOI:10.19539/j.cnki.2095-2694.2020.03.002.
|
| [8] |
|
| [9] |
|
| [10] |
中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华糖尿病杂志,2021,13(4):315-409. DOI:10.3760/cma.j.cn115791-20210221-00095.
|
| [11] |
李霞,周智广,亓海英,等. 用空腹C肽代替胰岛素改良Homa公式评价胰岛素抵抗和胰岛β细胞功能[J]. 中南大学学报(医学版),2004,29(4):419-423. DOI:10.3321/j.issn:1672-7347.2004.04.012.
|
| [12] |
陆佳萍,叶晓梅,韩辰宇,等. 2型糖尿病合并非酒精性脂肪肝的危险因素及其与中国人内脏脂肪指数的相关性研究[J]. 中国实用内科杂志,2022,42(11):925-929,935. DOI:10.19538/j.nk2022110111.
|
| [13] |
|
| [14] |
赵新,陈延延,李晓通,等. 2型糖尿病合并非酒精性脂肪肝与糖尿病慢性并发症的相关性[J]. 中国慢性病预防与控制,2014,22(1):26-28,32. DOI:10.16386/j.cjpccd.issn.1004-6194.2014.01.034.
|
| [15] |
文槟. 非酒精性脂肪肝患者病情的严重程度与其内脏脂肪指数、体重指数的关系[J]. 当代医药论丛,2021,19(22):77-79. DOI:10.3969/j.issn.2095-7629.2021.22.037.
|
| [16] |
|
| [17] |
郑海兰,丁维,李凡,等. 2型糖尿病患者合并非酒精性脂肪性肝病与甲状腺功能的相关性研究[J]. 中国糖尿病杂志,2019,27(11):820-824. DOI:10.3969/j.issn.1006-6187.2019.11.005.
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
张玄娥,王博,顾蕾,等. 上海市杨浦区50岁以上居民甲状腺结节与中心性肥胖及内脏脂肪指数的相关性[J]. 同济大学学报(医学版),2018,39(4):86-91. DOI:10.16118/j.1008-0392.2018.04.017.
|
| [41] |
|
| [42] |
钱巧慧,方琦,郭建,等. 非酒精性脂肪肝患者胰岛素抵抗程度与甲状腺结节的相关性研究[J]. 实用预防医学,2018,25(6):717-719. DOI:10.3969/j.issn.1006-3110.2018.06.021.
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
|
| [54] |
|
| [55] |
|
| [56] |
|
| [57] |
|
| [1] | ZHAO Yuqing, WANG Wei, CHEN Liyuan, YOU Huijuan, WEI Ying, WANG Qinglu, YANG Fengying. Liver Macrophage Polarisation: a New Target for Exercise Prevention and Treatment of Non-alcoholic Fatty Liver Disease [J]. Chinese General Practice, 2025, 28(27): 3456-3465. |
| [2] | LIU Yueying, WANG Xueli, LIU Yuqiu, WEI Limin. Correlation of Fasting C-peptide to Diabetes Duration Ration and Type 2 Diabetes Mellitus Combined with Metabolism-related Fatty Liver Disease [J]. Chinese General Practice, 2025, 28(23): 2852-2860. |
| [3] | LIANG Hengmiao, HUANG Sizhe, CHEN Yuting, LIU Ce, WANG Huijun, DU Qingfeng. A Retrospective Analysis of the Association between Serum Uric Acid Levels and Insulin Resistance Degrees in Individuals Undergoing Health Examination [J]. Chinese General Practice, 2025, 28(21): 2635-2642. |
| [4] | HAN Zheng, SUN Meng, FU Fanglin, PAN Yaojia, WANG Weiqiang. A Study on the Relationship between the Triglyceride-Glucose Index and Cardiometabolic Multimorbidity in Individuals Aged 50 and Above [J]. Chinese General Practice, 2025, 28(18): 2278-2284. |
| [5] | NI Xuetong, AHEYEERKE Halengbieke, TANG Jianmin, CAO Tengrui, TAO Lixin, ZHENG Deqiang, LI Qiang, HAN Yumei, YANG Xinghua. The Bidirectional Temporal Causal Association Study between Dysglycaemia and Non-alcoholic Fatty Liver Disease: Based on the Beijing Health Management Cohort [J]. Chinese General Practice, 2025, 28(13): 1607-1613. |
| [6] | BAI Lu, ZHANG Qiang, LIU Fangfang, SUN Caihong, FEI Sijie, XIN Caifeng. Correlation between Triglyceride Glucose Index and Atrial Fibrillation in Patients with Chronic Heart Failure [J]. Chinese General Practice, 2025, 28(06): 720-728. |
| [7] | XU Yaolong, ZHAO Jiaxin, YANG Ligang. Epidemic Status and Risk Factors of Non-alcoholic Fatty Liver Disease [J]. Chinese General Practice, 2024, 27(30): 3825-3834. |
| [8] | XU Lili, ZHENG Wei, YUAN Xianxian, MA Kaiwen, ZHANG Puyang, LI Guanghui. The Relationship between Body Composition in Early Pregnancy and Gestational Diabetes Mellitus in a Population of Normal BMI Pregnant Women [J]. Chinese General Practice, 2024, 27(29): 3602-3607. |
| [9] | FU Wei, CHENG Guobin, LYU Linya, DING Yao, WANG Yao, ZHAO Junlong. Association of Monounsaturated Fatty Acid Intake with Nonalcoholic Fatty Liver Disease Risk in Chinese Han Adults: a Retrospective Case-control Study [J]. Chinese General Practice, 2024, 27(29): 3623-3628. |
| [10] | LI Mengyuan, GAO Zheng, LIANG Jingqiao, ZHANG Yadong, LI Bo, XU Xin. The Efficacy of Yishen Quzhuo Formula Compared with Metformin in the Treatment of Polycystic Ovary Syndrome with Insulin Resistance: a Randomized Controlled Trial [J]. Chinese General Practice, 2024, 27(27): 3411-3417. |
| [11] | HOU Qinchuan, ZHANG Rui, LI Binghong, ZHANG Huiwang, ZHANG Beibei, YONG Tao, LIU Yuping, SHUAI Ping. A Retrospective Cohort Study on the Relationship between Triglyceride-Glucose Index and Its Combination with Obesity Indices and Chronic Kidney Disease in Adults [J]. Chinese General Practice, 2024, 27(22): 2731-2738. |
| [12] | HOU Nana, FENG Jinzhang, LIU Suohong, FENG Junfang, XUE Xiaoyan, YIN Na, CHI Gefu. Correlation between Serum Uric Acid/Creatinine Ratio and Metabolism-associated Fatty Liver Disease [J]. Chinese General Practice, 2024, 27(20): 2476-2482. |
| [13] | HUANG Shuwei, ZHOU Zhiheng, FENG Tianyuan, LIU Li, DENG Guangpu, LI Yaotian, ZHU Hong. Study on the Predictive Value of Different Insulin Resistance Replacement Indices for Hyperuricemia in Middle-aged and Elderly Patients with Type 2 Diabetes [J]. Chinese General Practice, 2024, 27(19): 2364-2374. |
| [14] | YIN Qiuguo, QIN Xintong, ZHANG Yidan, JIANG Peng, GUO Ping, JIA Xingtai, JIAN Liguo. Correlation between Insulin Resistance Metabolic Score and Poor Prognosis in Patients with Chronic Heart Failure [J]. Chinese General Practice, 2024, 27(18): 2179-2185. |
| [15] | NI Xuetong, WANG Ruoxi, ZHANG Jing, YANG Xinghua. Research Progress in the Correlation of Non-alcoholic Fatty Liver Disease and Metabolic-associated Fatty Liver Disease with Cardiovascular Diseases in China and Abroad [J]. Chinese General Practice, 2024, 27(16): 2033-2038. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||