中国全科医学 ›› 2024, Vol. 27 ›› Issue (06): 692-698.DOI: 10.12114/j.issn.1007-9572.2023.0263
所属专题: 泌尿系统疾病最新文章合辑
高歌, 张鑫越, 冯玉华, 窦婧予, 吴雪莹, 程根阳*( )
)
GAO Ge, ZHANG Xinyue, FENG Yuhua, DOU Jingyu, WU Xueying, CHENG Genyang*()
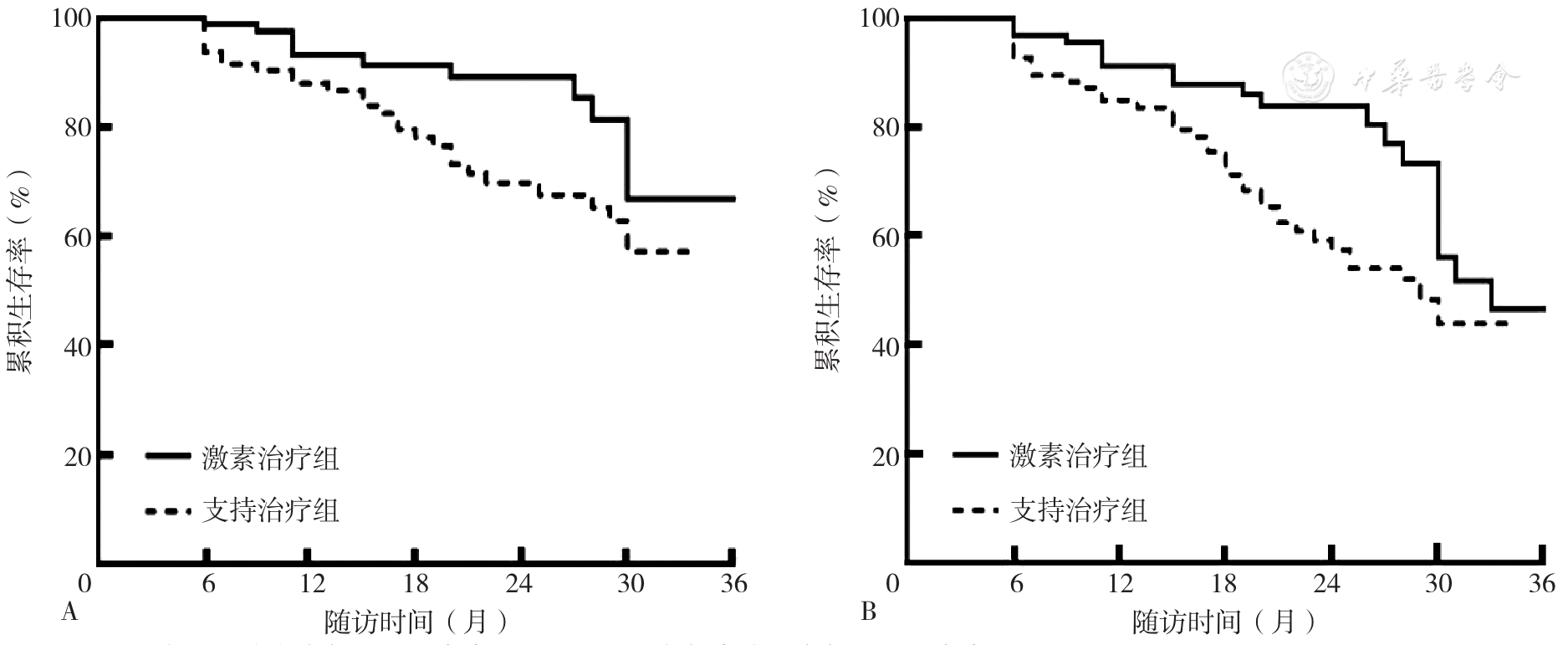
摘要: 背景 IgA肾病(IgAN)是世界范围内常见的原发性肾小球肾炎之一,目前糖皮质激素是否能改善慢性肾脏病(CKD)进展高风险IgAN患者肾脏预后尚无明确结论。 目的 本研究旨在探讨激素治疗对CKD进展高风险IgAN患者的治疗反应及肾脏预后的影响。 方法 回顾性纳入2017年1月—2021年10月于郑州大学第一附属医院就诊的CKD进展高风险IgAN患者。根据是否进行激素治疗将患者分为激素治疗组和支持治疗组,采用倾向匹配法按照性别、年龄、24 h尿蛋白定量、估算肾小球滤过率(eGFR)对患者进行1∶1匹配筛选病例,收集患者的临床及病理资料,记录患者治疗1年内疾病缓解情况及不良反应发生情况。以开始支持治疗的日期作为随访起点,随访至2022-10-31,主要终点事件定义为:进展为终末期肾脏病(ESRD)或接受透析治疗。复合终点事件定义为:eGFR较基线持续下降超过30%或进入ESRD或接受透析或患者死亡;运用Kaplan-Meier法绘制生存曲线,并采用Log-rank检验比较两组患者主要/复合终点事件累积发生率的差异。运用Cox比例风险回归分析探究影响CKD进展高风险IgAN患者预后的可能因素。 结果 共有236例原发性IgAN患者符合纳入标准,经过1∶1匹配,激素治疗组97例与支持治疗组97患者匹配成功,两组基线数据匹配均衡。激素治疗组患者完全缓解率、部分缓解率均高于支持治疗组(χ2=6.171,P=0.013;χ2=3.973,P=0.046)。中位随访时间为18.00(9.75,28.00)个月。Kaplan-Meier生存分析结果显示,激素治疗组的主要终点事件累积发生率低于支持治疗组(χ2=4.495,P=0.034);激素治疗组的复合终点事件累积发生率低于支持治疗组(χ2=4.419,P=0.036)。符合纳入标准的236例患者中有177例中等量蛋白尿患者,采用倾向匹配法按照性别、年龄、24 h尿蛋白定量、eGFR对激素治疗和支持治疗的177例患者进行1∶1匹配后,激素治疗中等量蛋白尿者和支持治疗中等量蛋白尿者各有76例患者匹配成功。Kaplan-Meier生存曲线结果显示,激素治疗中等量蛋白尿者的主要终点事件累积发生率低于支持治疗中等量蛋白尿者(χ2=4.127,P=0.042);激素治疗中等量蛋白尿者的复合终点事件累积发生率低于支持治疗中等量蛋白尿者(χ2=4.934,P=0.026)。多因素Cox比例风险回归分析结果显示血红蛋白(HR=0.982)、血肌酐(HR=1.019)、eGFR(HR=1.020)、24 h尿蛋白定量(HR=1.205)是影响CKD进展高风险IgAN患者发生主要终点事件的影响因素(P<0.05)。激素治疗组感染发生率高于支持治疗组(P<0.05)。 结论 在CKD进展高风险IgAN肾病患者中,与单纯支持治疗相比,激素治疗可以显著提升肾脏缓解率,降低肾功能下降、肾衰竭风;但仍需警惕其不良反应的发生。