中国全科医学 ›› 2023, Vol. 26 ›› Issue (14): 1703-1708.DOI: 10.12114/j.issn.1007-9572.2022.0658
所属专题: 心血管最新文章合辑
马万瑞1, 马乾凤2, 吴竞捷3, 王立群4, 王志忠1,5,*( )
)
MA Wanrui1, MA Qianfeng2, WU Jingjie3, WANG Liqun4, WANG Zhizhong1,5,*()
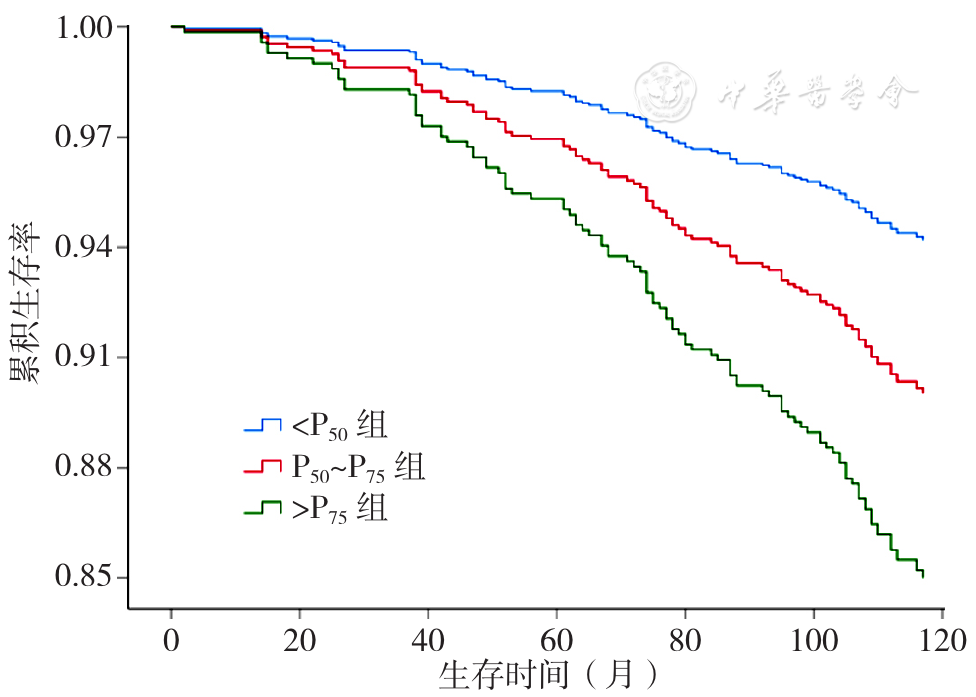
摘要: 背景 心血管代谢性危险因素聚集(CRFC)是老年人常见的健康问题,目前相关研究主要集中在流行病学分布特征的描述,有关CRFC与人群全因死亡风险的研究鲜有报道。目的 探讨CRFC与社区≥55岁人群全因死亡风险的关系,为开展≥55岁人群社区保健提供参考。方法 于2011年9—11月采用典型抽样法选取宁夏回族自治区吴忠市和银川市5个社区的1 046名≥55岁人群作为研究对象,对其开展一般情况问卷调查、体格检查、超声检查、实验室检查和CRFC评价〔纳入中心性肥胖、高胆固醇血症、高三酰甘油血症、高低密度脂蛋白血症、低高密度脂蛋白血症、高血压、糖尿病、高尿酸血症、非酒精性脂肪性肝病(NAFLD)共计9项心血管代谢性危险因素后,控制一般情况变量,通过构建多因素Cox比例风险回归模型,估计各个心血管代谢性危险因素的回归系数β,以回归系数β为权重将所有心血管代谢性危险因素的评分相加得出心血管代谢危险因素危险总评分〕,将心血管代谢危险因素危险总评分按照四分位数分为三组:<P50组,P50~P75组,>P75组;分别于2017年,2019年和2021年通过面访和死因监测系统搜索的方式完成随访。采用Kaplan-Meier法绘制<P50组,P50~P75组,>P75组社区老年人全因死亡的生存曲线,生存曲线比较采用Log-rank检验;采用多因素Cox比例风险回归分析一般情况、各心血管代谢性危险因素、心血管代谢危险因素危险总评分、心血管代谢危险因素危险总评分分组、年龄组分层与社区≥55岁人群全因死亡风险的关系。结果 研究对象年龄55~88岁,平均年龄(66.4±6.6)岁。共观察到106例死亡案例,10年累计死亡率为10.13%。随着危险评分的增加,个体预期中位生存时间显著缩短,>P75组累积生存率低于P50~P75组和<P50组;多因素Cox比例风险回归分析结果显示,年龄、性别、独居、文化程度可能是社区老年人全因死亡风险的影响因素(P<0.05);控制一般情况后,多因素Cox比例风险回归分析结果显示,心血管代谢危险因素危险总评分是社区≥55岁人群全因死亡风险的影响因素〔HR=3.04,95%CI(1.55,5.97),P=0.001〕,且心血管代谢危险因素总评分越高死亡风险亦越高,>P75组全因死亡风险高于<P50组〔HR=2.02,95%CI(1.16,3.50),P=0.013〕;以年龄组分层多因素Cox比例风险回归分析结果显示,≥65岁年龄组心血管代谢危险因素总评分与社区≥55岁人群全因死亡风险显著关联〔HR=2.79,95%CI(1.36,5.74),P=0.005〕;>P75组全因死亡风险高于<P50组〔HR=1.83,95%CI(1.02,3.28),P=0.042〕。结论 CRFC与社区≥55岁人群全因死亡风险显著关联,其聚集程度越高全因死亡风险越高,提示早期评价CRFC并给予干预可能对提高社区≥55岁人群保健效果、降低死亡风险具有一定意义。