中国全科医学 ›› 2022, Vol. 25 ›› Issue (17): 2173-2178.DOI: 10.12114/j.issn.1007-9572.2021.01.415
• 全科医生知识窗 • 上一篇
梁丽娟1, 蒋吴君2, 陈文雅1, 黄锐波1, 叶培韬1, 彭咏怡1, 雷薛冬1, 梁健玲1, 高怡1,*( ), 郑劲平1,*()
), 郑劲平1,*()
Lijuan LIANG1, Wujun JIANG2, Wenya CHEN1, Ruibo HUANG1, Peitao YE1, Yongyi PENG1, Xuedong LEI1, Jianling LIANG1, Yi GAO1,*(), Jinping ZHENG1,*()
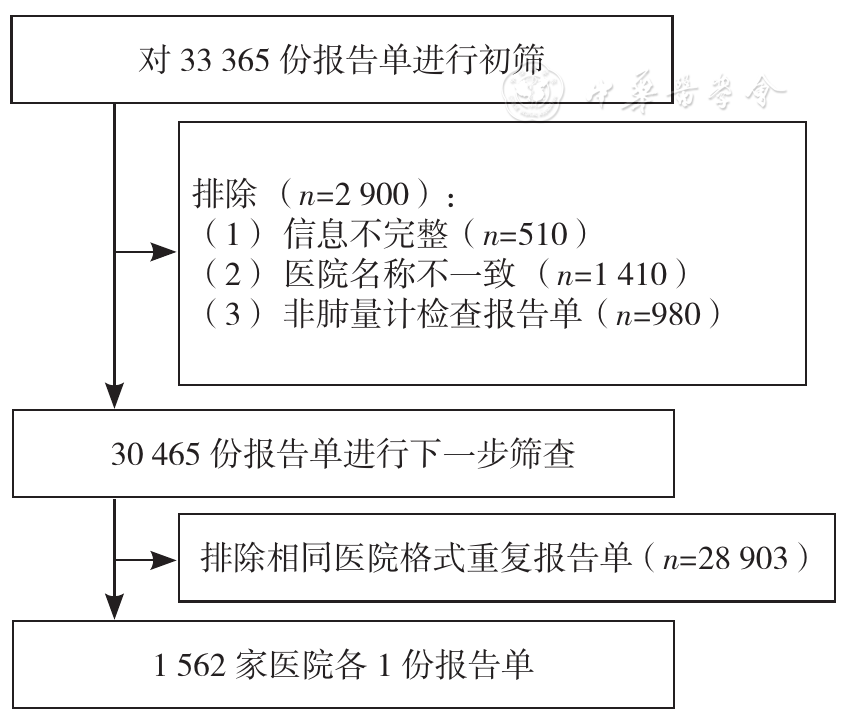
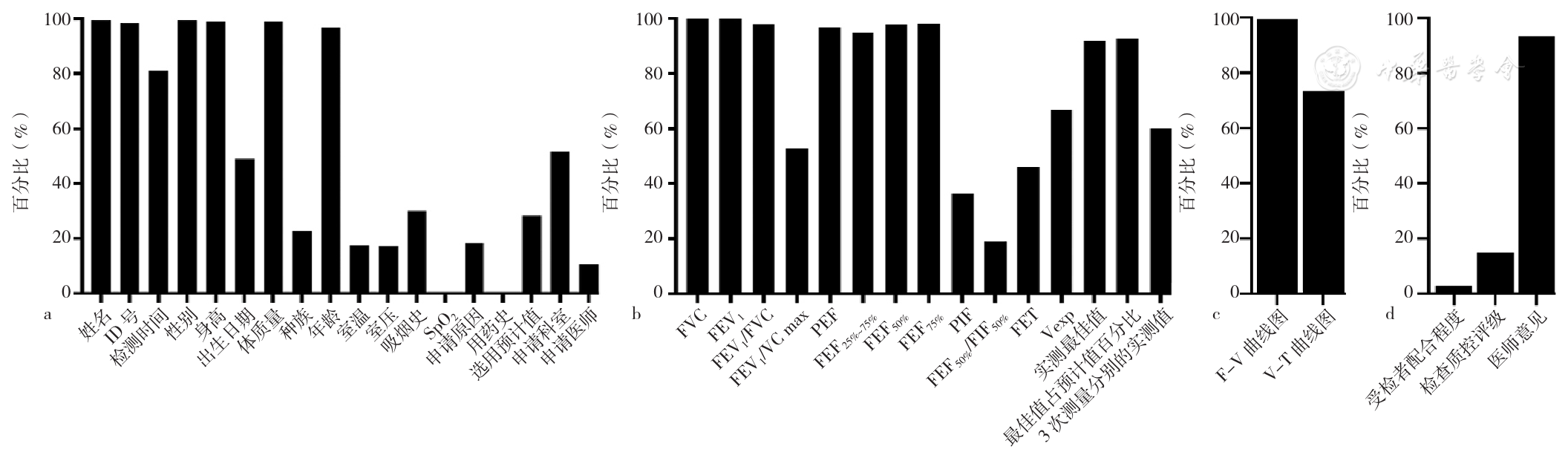
摘要: 背景 肺量计检查是最常见且应用最广泛的肺功能检查手段,其质量控制(以下简称质控)是肺功能检查推广应用的基石,报告单格式的质控是肺量计检查质控的关键一环,但我国肺量计检查报告单格式总体参差不齐,不利于肺量计检查的推广应用。 目的 探讨我国肺量计检查报告单格式的现状。 方法 收集2016年4月至2018年12月部分医院的肺量计检查报告单,分为受试者基本信息、检查指标、结果图形、结果评价4部分,每部分均以关键指标和/或重要指标进行评价。(1)受试者基本信息关键指标包括性别、身高、体质指数、年龄、预计值来源等;(2)检查指标关键指标包括用力肺活量(FVC)、第1秒用力呼气容积(FEV1)、1秒率(FEV1/FVC或FEV1/VCmax),重要指标包括最大呼气中期流量(FEF25%~75%、用力呼出50%及75%肺活量时的瞬时呼气流量(FEF50%、FEF75%)、吸气峰值流量(PIF)、用力呼气时间(FET)等;(3)结果图形关键指标包括流量-容积曲线(F-V曲线)、容积-时间曲线(V-T曲线);(4)结果评价关键指标包括受试者配合程度、检查质控评级、医师意见。比较不同地区及等级医院间报告单格式达标差异。 结果 共纳入1 562家医院各1份肺量计检查报告单,其中仅0.4%含所有关键指标。(1)受试者基本信息:27.7%的肺量计检查报告单无关键指标缺失,28.2%的肺量计检查报告单含预计值来源,不同地区及不同等级医院间肺量计检查报告单受试者基本信息关键指标比较,差异均有统计学意义(P<0.05);(2)检查指标:91.9%的肺量计检查报告单无关键指标缺失,超90.0%的肺量计检查报告单列出FEF25%~75%、FEF50%和FEF75%,仅36.4%、46.0%的报告单报告了PIF、FET;(3)结果图形:73.4%的肺量计检查报告单无关键指标缺失,26.6%的肺量计检查报告单无V-T曲线;(4)结果评价:1.6%的肺量计检查报告单无关键指标缺失,14.9%的肺量计检查报告单报告了质控评级,不同等级医院间肺量计检查报告单结果评价比较,差异有统计学意义(P<0.05)。 结论 我国部分医院肺量计检查报告单格式与规范要求差距较大,预计值来源、吸气相和质控指标及质控评级等部分的缺失严重影响了肺功能检查对临床的指导价值,建议在肺功能检查规范化相关培训中增添针对报告单格式的规范化培训,并加强肺功能相关医务工作者对报告单各项指标的理解及应用。