
Chinese General Practice ›› 2026, Vol. 29 ›› Issue (21): 2950-2958.DOI: 10.12114/j.issn.1007-9572.2025.0339
Special Issue: 肥胖/减重最新文章合辑
• Article • Previous Articles Next Articles
Received:2025-09-03
Revised:2025-10-21
Published:2026-07-20
Online:2026-06-03
Contact:
ZHAO Qian
通讯作者:
赵倩
作者简介:作者贡献:
韩聪聪负责研究设计、数据整理,完成论文初稿撰写;邱欣雨协助研究设计与方案制订、完成部分数据分析,并对论文内容提出修改建议;单春方、宋宁、陈清杰负责数据收集并参与数据整理;穆拉迪力·阿卜杜热合曼参与统计分析与讨论部分撰写;李晓梅负责研究指导,协助方法与讨论部分内容完善;杨毅宁、赵倩负责全面指导研究实施与论文写作,监督文章的整体质量,审定最终版本。
基金资助:CLC Number:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2025.0339
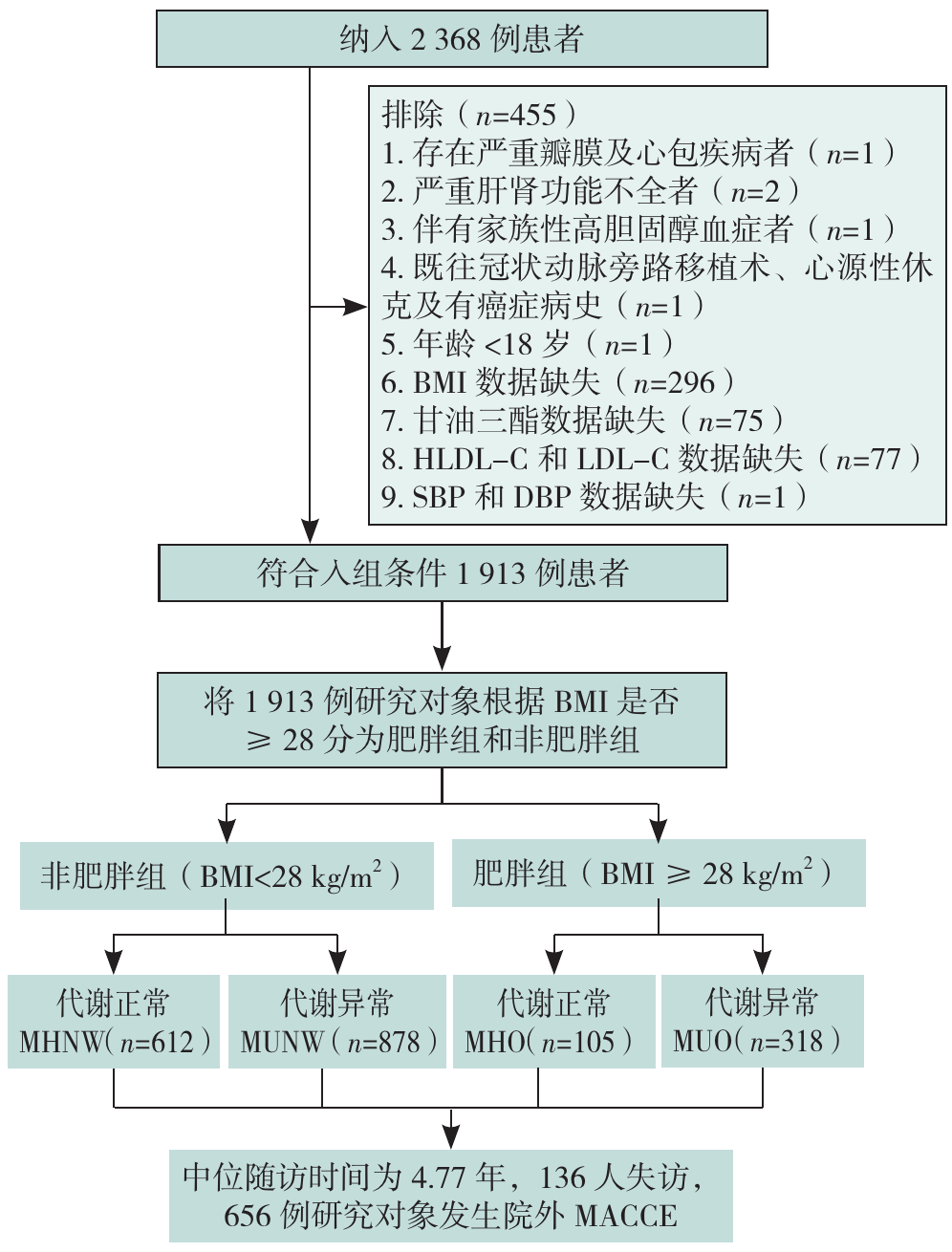
Figure 1 Research flowchart
| 项目 | MHNW(n=612) | MHO(n=105) | MUNW(n=878) | MUO(n=318) | 检验统计量值 | P值 |
|---|---|---|---|---|---|---|
| 年龄( | 59.6±12.1 | 54.9±12.0 | 60.4±11.9 | 54.3±11.5 | 24.69 | <0.001 |
| 性别[例(%)] | 25.88a | <0.001 | ||||
| 男 | 537(87.7) | 92(87.6) | 688(78.4) | 271(85.2) | ||
| 女 | 75(12.3) | 13(12.4) | 190(21.6) | 47(14.8) | ||
| BMI( | 23.9±2.4 | 30.7±3.1 | 24.6±2.1 | 30.7±3.0 | 759.96 | <0.001 |
| 高血压[例(%)] | 128(20.9) | 20(19.0) | 599(68.2) | 215(67.6) | 403.35a | <0.001 |
| 糖尿病[例(%)] | 33(5.4) | 2(1.9) | 389(44.3) | 125(39.3) | 321.30a | <0.001 |
| 吸烟[例(%)] | 334(54.6) | 60(57.1) | 406(46.2) | 179(56.3) | 16.21a | 0.001 |
| 饮酒[例(%)] | 209(34.2) | 38(36.2) | 272(31.0) | 109(34.3) | 2.69a | 0.442 |
| 入院心率( | 82.2±38.7 | 84.3±16.2 | 83.2±24.8 | 87.2±56.9 | 1.41 | 0.238 |
| 入院SBP( | 122±19 | 128±20 | 126±21 | 128±21 | 10.22 | <0.001 |
| 入院DBP( | 76±13 | 81±13 | 77±13 | 80±14 | 7.58 | <0.001 |
| 血糖( | 6.6±2.8 | 6.6±2.2 | 8.1±3.8 | 8.0±4.0 | 28.03 | <0.001 |
| 白细胞计数( | 10.2±3.5 | 10.5±3.5 | 10.1±3.4 | 10.4±3.5 | 0.77 | 0.511 |
| 血红蛋白浓度( | 146.8±16.3 | 152.8±15.6 | 145.2±18.8 | 151.9±15.8 | 15.51 | <0.001 |
| TC( | 4.6±1.1 | 4.6±1.0 | 4.5±1.2 | 4.7±1.2 | 1.46 | 0.223 |
| TG[M(P25,P75),mmol/L] | 1.2(0.9,1.7) | 1.4(1.0,1.7) | 2.0(1.3,2.9) | 2.4(1.6,3.4) | 345.31b | <0.001 |
| HDL-C( | 1.1±0.3 | 1.0±0.3 | 0.9±0.2 | 0.9±0.2 | 126.00 | <0.001 |
| LDL-C( | 3.0±1.0 | 3.1±0.8 | 2.8±1.0 | 2.9±1.0 | 8.61 | <0.001 |
| 肌酐( | 75.0±22.2 | 73.9±20.7 | 83.4±62.0 | 79.2±38.9 | 4.38 | 0.004 |
| 尿素( | 5.7±2.0 | 5.2±1.4 | 6.1±2.7 | 5.8±2.2 | 6.74 | <0.001 |
| 尿酸( | 333.7±92.3 | 371.1±100.0 | 343.1±97.1 | 367.5±102.6 | 11.14 | <0.001 |
| 总胆红素( | 14.6±6.6 | 15.4±7.1 | 14.3±7.0 | 14.9±7.8 | 1.30 | 0.272 |
| 直接胆红素( | 1.9±1.9 | 2.3±2.3 | 1.7±2.1 | 1.6±2.2 | 3.87 | 0.009 |
| 左心室射血分数( | 57.7±6.8 | 57.3±6.8 | 57.9±7.0 | 57.2±6.6 | 3.80 | 0.284 |
Table 1 Comparison of baseline characteristics among different obesity metabolic phenotype groups
| 项目 | MHNW(n=612) | MHO(n=105) | MUNW(n=878) | MUO(n=318) | 检验统计量值 | P值 |
|---|---|---|---|---|---|---|
| 年龄( | 59.6±12.1 | 54.9±12.0 | 60.4±11.9 | 54.3±11.5 | 24.69 | <0.001 |
| 性别[例(%)] | 25.88a | <0.001 | ||||
| 男 | 537(87.7) | 92(87.6) | 688(78.4) | 271(85.2) | ||
| 女 | 75(12.3) | 13(12.4) | 190(21.6) | 47(14.8) | ||
| BMI( | 23.9±2.4 | 30.7±3.1 | 24.6±2.1 | 30.7±3.0 | 759.96 | <0.001 |
| 高血压[例(%)] | 128(20.9) | 20(19.0) | 599(68.2) | 215(67.6) | 403.35a | <0.001 |
| 糖尿病[例(%)] | 33(5.4) | 2(1.9) | 389(44.3) | 125(39.3) | 321.30a | <0.001 |
| 吸烟[例(%)] | 334(54.6) | 60(57.1) | 406(46.2) | 179(56.3) | 16.21a | 0.001 |
| 饮酒[例(%)] | 209(34.2) | 38(36.2) | 272(31.0) | 109(34.3) | 2.69a | 0.442 |
| 入院心率( | 82.2±38.7 | 84.3±16.2 | 83.2±24.8 | 87.2±56.9 | 1.41 | 0.238 |
| 入院SBP( | 122±19 | 128±20 | 126±21 | 128±21 | 10.22 | <0.001 |
| 入院DBP( | 76±13 | 81±13 | 77±13 | 80±14 | 7.58 | <0.001 |
| 血糖( | 6.6±2.8 | 6.6±2.2 | 8.1±3.8 | 8.0±4.0 | 28.03 | <0.001 |
| 白细胞计数( | 10.2±3.5 | 10.5±3.5 | 10.1±3.4 | 10.4±3.5 | 0.77 | 0.511 |
| 血红蛋白浓度( | 146.8±16.3 | 152.8±15.6 | 145.2±18.8 | 151.9±15.8 | 15.51 | <0.001 |
| TC( | 4.6±1.1 | 4.6±1.0 | 4.5±1.2 | 4.7±1.2 | 1.46 | 0.223 |
| TG[M(P25,P75),mmol/L] | 1.2(0.9,1.7) | 1.4(1.0,1.7) | 2.0(1.3,2.9) | 2.4(1.6,3.4) | 345.31b | <0.001 |
| HDL-C( | 1.1±0.3 | 1.0±0.3 | 0.9±0.2 | 0.9±0.2 | 126.00 | <0.001 |
| LDL-C( | 3.0±1.0 | 3.1±0.8 | 2.8±1.0 | 2.9±1.0 | 8.61 | <0.001 |
| 肌酐( | 75.0±22.2 | 73.9±20.7 | 83.4±62.0 | 79.2±38.9 | 4.38 | 0.004 |
| 尿素( | 5.7±2.0 | 5.2±1.4 | 6.1±2.7 | 5.8±2.2 | 6.74 | <0.001 |
| 尿酸( | 333.7±92.3 | 371.1±100.0 | 343.1±97.1 | 367.5±102.6 | 11.14 | <0.001 |
| 总胆红素( | 14.6±6.6 | 15.4±7.1 | 14.3±7.0 | 14.9±7.8 | 1.30 | 0.272 |
| 直接胆红素( | 1.9±1.9 | 2.3±2.3 | 1.7±2.1 | 1.6±2.2 | 3.87 | 0.009 |
| 左心室射血分数( | 57.7±6.8 | 57.3±6.8 | 57.9±7.0 | 57.2±6.6 | 3.80 | 0.284 |
| MACCE类型 | MHNW(n=612) | MHO(n=105) | MUNW(n=878) | MUO(n=318) | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 不稳定型心绞痛再入院 | 91(14.9) | 19(18.1) | 164(18.7) | 71(22.3)a | 8.36 | 0.039 |
| 心力衰竭再入院 | 30(4.9) | 9(8.6) | 45(5.1) | 25(7.9) | 5.64 | 0.130 |
| 全因死亡 | 29(4.7) | 3(2.9) | 47(5.4) | 11(3.5) | 2.72 | 0.436 |
| 脑卒中 | 11(1.8) | 5(4.8) | 30(3.4) | 12(3.8) | 5.28 | 0.152 |
| 非致死性心肌梗死 | 13(2.1) | 4(3.8) | 23(2.6) | 14(4.4) | 4.49 | 0.213 |
| 合计 | 174(28.4) | 40(38.1)a | 309(35.2)a | 133(41.8)ab | 18.33 | <0.001 |
Table 2 Comparison of the incidence of MACCE among people with different metabolic phenotypes of obesity
| MACCE类型 | MHNW(n=612) | MHO(n=105) | MUNW(n=878) | MUO(n=318) | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 不稳定型心绞痛再入院 | 91(14.9) | 19(18.1) | 164(18.7) | 71(22.3)a | 8.36 | 0.039 |
| 心力衰竭再入院 | 30(4.9) | 9(8.6) | 45(5.1) | 25(7.9) | 5.64 | 0.130 |
| 全因死亡 | 29(4.7) | 3(2.9) | 47(5.4) | 11(3.5) | 2.72 | 0.436 |
| 脑卒中 | 11(1.8) | 5(4.8) | 30(3.4) | 12(3.8) | 5.28 | 0.152 |
| 非致死性心肌梗死 | 13(2.1) | 4(3.8) | 23(2.6) | 14(4.4) | 4.49 | 0.213 |
| 合计 | 174(28.4) | 40(38.1)a | 309(35.2)a | 133(41.8)ab | 18.33 | <0.001 |
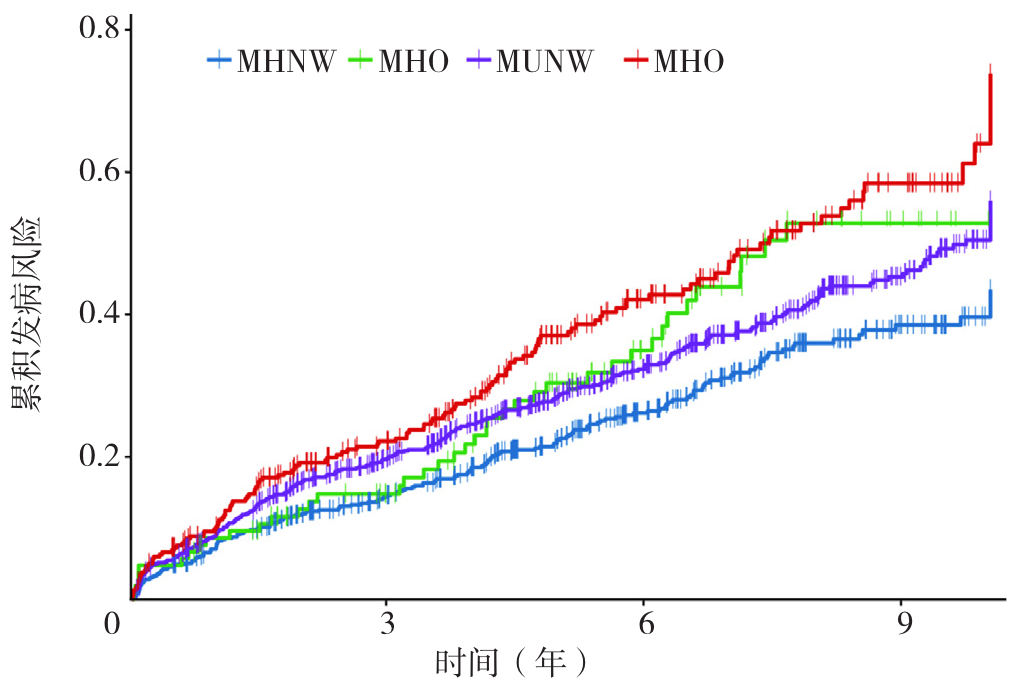
Figure 2 Kaplan-Meier survival curves of MACCE cumulative events across different obesity metabolic phenotypes groups
| 变量 | 模型1 | 模型2 | 模型3 | |||
|---|---|---|---|---|---|---|
| HR(95%CI) | P值 | HR(95%CI) | P值 | HR(95%CI) | P值 | |
| MHNW组(参照组) | 1.00 | 1.00 | 1.00 | |||
| MHO组 | 1.43(1.01~2.02) | 0.042 | 1.56(1.10~2.20) | 0.012 | 1.56(1.10~2.21) | 0.013 |
| MUNW组 | 1.33(1.10~1.60) | 0.003 | 1.32(1.10~1.59) | 0.003 | 1.28(1.04~1.58) | 0.020 |
| MUO组 | 1.79(1.42~2.24) | <0.001 | 2.00(1.59~2.52) | <0.001 | 1.94(1.51~2.50) | <0.001 |
Table 3 Relationship between metabolic phenotype grouping of obesity and MACCE under different modes
| 变量 | 模型1 | 模型2 | 模型3 | |||
|---|---|---|---|---|---|---|
| HR(95%CI) | P值 | HR(95%CI) | P值 | HR(95%CI) | P值 | |
| MHNW组(参照组) | 1.00 | 1.00 | 1.00 | |||
| MHO组 | 1.43(1.01~2.02) | 0.042 | 1.56(1.10~2.20) | 0.012 | 1.56(1.10~2.21) | 0.013 |
| MUNW组 | 1.33(1.10~1.60) | 0.003 | 1.32(1.10~1.59) | 0.003 | 1.28(1.04~1.58) | 0.020 |
| MUO组 | 1.79(1.42~2.24) | <0.001 | 2.00(1.59~2.52) | <0.001 | 1.94(1.51~2.50) | <0.001 |
| 变量 | 敏感性分析1 | 敏感性分析2 | 敏感性分析3 | |||
|---|---|---|---|---|---|---|
| HR(95% CI) | P值 | HR(95% CI) | P值 | HR(95% CI) | P值 | |
| MHNW组(参照组) | 1.00 | 1.00 | 1.00 | |||
| MHO组 | 1.13(0.86~1.48) | 0.397 | 1.50(1.20~1.86) | <0.001 | 1.47(1.08~2.02) | 0.016 |
| MUNW组 | 1.44(1.09~1.91) | 0.011 | 1.33(1.10~1.61) | 0.004 | 1.29(1.09~1.54) | 0.004 |
| MUO组 | 1.46(1.15~1.85) | 0.002 | 1.62(1.25~2.12) | <0.001 | 1.80(1.46~2.23) | <0.001 |
Table 4 Sensitivity analysis of metabolic obesity phenotypes and their association with the risk of MACCE
| 变量 | 敏感性分析1 | 敏感性分析2 | 敏感性分析3 | |||
|---|---|---|---|---|---|---|
| HR(95% CI) | P值 | HR(95% CI) | P值 | HR(95% CI) | P值 | |
| MHNW组(参照组) | 1.00 | 1.00 | 1.00 | |||
| MHO组 | 1.13(0.86~1.48) | 0.397 | 1.50(1.20~1.86) | <0.001 | 1.47(1.08~2.02) | 0.016 |
| MUNW组 | 1.44(1.09~1.91) | 0.011 | 1.33(1.10~1.61) | 0.004 | 1.29(1.09~1.54) | 0.004 |
| MUO组 | 1.46(1.15~1.85) | 0.002 | 1.62(1.25~2.12) | <0.001 | 1.80(1.46~2.23) | <0.001 |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
肥胖症诊疗指南(2024年版)[J]. 中国循环杂志, 2025, 40(1): 6-30.
|
| [19] |
Third report of the national cholesterol education program (NCEP) Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panelⅲ) final report [J]. Circulation, 2002, 106(25): 3143-421.
|
| [20] |
何权瀛, 高莹慧. 关于吸烟问题若干名词定义[J]. 中华结核和呼吸杂志, 2009, 32(1): 26. DOI: 10.3760/cma.j.issn.1001-0939.2009.01.008.
|
| [21] |
|
| [22] |
中国高血压防治指南修订委员会, 高血压联盟, 中国医疗保健国际交流促进会高血压病学分会, 等. 中国高血压防治指南(2024年修订版)[J]. 中华高血压杂志(中英文), 2024, 32(07): 603-700. DOI: 10.16439/j.issn.1673-7245.2024.07.002.
|
| [23] |
中华医学会糖尿病学分会代谢综合征研究协作组. 中华医学会糖尿病学分会关于代谢综合征的建议[J]. 中华糖尿病杂志, 2004, (3): 5-10.
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
冯嘉, 吕垚, 周伊恒, 等. 脂肪组织与肥胖相关高血压发病机制研究进展[J/OL]. 中国全科医学, 1-8. [2025-09-01].
|
| [36] |
|
| [37] |
张泽宇, 李春晖. 1990—2021年中国归因于二手烟的缺血性心脏病疾病负担分析[J/OL]. 中国全科医学, 1-11. [2025-09-01].
|
| [38] |
|
| [39] |
|
| [40] |
|
| [1] | LI Wenzhe, YANG Yuqing, YANG Tingjie, GUO Yiming, CHEN Lulin, CAO Yudong, YUAN Jiangshu, YANG Honghui, WANG Che. Correlation Analysis between Triglyceride-glucose Index, Triglyceride-glucose-BMI and Vulnerable Plaques in Patients with Acute Coronary Syndrome [J]. Chinese General Practice, 2026, 29(23): 3287-3293. |
| [2] | ZHANG Wenzheng, ZHANG Hongling. Association between Cardiometabolic Index and Hypertension in Elderly Patients with Metabolic Associated Fatty Liver Disease in the Community Population: a Prospective Cohort Study [J]. Chinese General Practice, 2026, 29(23): 3261-3267. |
| [3] | Expert Group on Guidelines for the Assessment, Treatment, and Prevention of Childhood Obesity in China, Professional Committee on Obesity Control in Women and Children, China Maternal and Child Health Research Association. Guidelines for the Assessment, Treatment, and Prevention of Childhood Obesity in China (Second Edition) [J]. Chinese General Practice, 2026, 29(23): 3233-3252. |
| [4] | LIN Yanping, HUANG Jiachun, GUO Haiwei, ZHAO Rui, YANG Haolin, WAN Lei, ZHU Genfu, HUANG Hongxing. Study on the Distribution of TCM Syndrome Types and the Relationship between Muscle-bone-lipid in Patients with Primary Osteoporosis [J]. Chinese General Practice, 2026, 29(21): 3040-3045. |
| [5] | CHAI Zhihao, ZHANG Weisen, LUO Jiaoling, ZHU Feng, ZHU Tong, JIN Yali, PAN Jing, LU Yingjun, JIANG Chaoqiang. The Mediation Effect of Socioeconomic Status in Childhood Parental Literacy and Cognitive Function in Middle-aged and Older People: Based on Guangzhou Biobank Cohort Study [J]. Chinese General Practice, 2026, 29(21): 2959-2966. |
| [6] | LIU Shuai, YUAN Shizhao, LIU Yan, JIA Shuoxian, ZHAO Yan, WANG Ziyi, ZHOU Chunhua, YU Jing. Evaluation of the Efficacy, Safetyand Economy of Different Amphotericin B Formulationsin Invasive Fungal Disease: a Retrospective Cohort Study [J]. Chinese General Practice, 2026, 29(21): 2967-2974. |
| [7] | ZHANG Ke, ZENG Xianchang, ZOLZAYA Enkhzaya, ZHU Yelin, HUANG Yiwen, LIU Zhenxiu, TAO Feng. Effect of Xiere Xingpi Yin on Eating Behaviors and Weight-related Outcomes in Patients with Obesity: a Randomized Controlled Trial [J]. Chinese General Practice, 2026, 29(20): 2759-2765. |
| [8] | REYILAI· Maimaiti, ZHOU Yiran, WU Yun, LIU Zhencheng, LU Yaoqin, WU Haiyan. Association between Novel Obesity Indicators and Cardiovascular Disease Risk in Hypertensive Patients [J]. Chinese General Practice, 2026, 29(20): 2836-2845. |
| [9] | WU Zhen, XI Yaqi, HU Linlin. Characteristics of Policy Instrument Selection and Combination for Weight Management in China: a Content Analysis of National Policy Documents (2016-2025) [J]. Chinese General Practice, 2026, 29(20): 2766-2774. |
| [10] | CHEN Xiangyang, HUANG Hongmei, LI Sheyu. Prevention and Management of Adult Obesity: Progress and Trends from Six Keywords in 2025 [J]. Chinese General Practice, 2026, 29(20): 2753-2758. |
| [11] | TANG Lijuan, QI Qi, ZHANG Fan, GAO Yifu, CAO Yajing, YUE Fujuan, GAO Jinchai, LIU Xiaoli. Characterisation of the Prevalence of Overweight/Obesity among Residents Aged 18-44 Years in Hebei Province in 2013 and 2020 [J]. Chinese General Practice, 2026, 29(19): 2695-2704. |
| [12] | LI Yachan, YANG Yang, XU Qianting, KE Tingyu. Association between the Chinese Visceral Adiposity Index and Left Ventricular Diastolic Dysfunction in Type 2 Diabetes Mellitus [J]. Chinese General Practice, 2026, 29(18): 2482-2488. |
| [13] | LI Simin, ZHANG Tingting, WANG Kunbo, YANG Jianzhou, PING Weiwei. Effects of Exercise Dosage on Elderly Patients with Sarcopenia: a Meta-analysis [J]. Chinese General Practice, 2026, 29(17): 2400-2409. |
| [14] | Chinese Nutrition Society Obesity Prevention and Control Branch. Chinese Guidelines for Behavioral and Lifestyle Interventions for Obesity [J]. Chinese General Practice, 2026, 29(16): 2113-2139. |
| [15] | LI Jiali, LIU Fan, KE Lixin, LI Huijuan, WANG Haibo, ZHAO Xiaoxiao, ZHAO Xinke, LU Cuncun. Disease Burden of Obesity among Individuals Aged 60 and above Globally and in China from 1990 to 2021: Trend Analysis and Model-based Projection [J]. Chinese General Practice, 2026, 29(15): 2067-2076. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||