
Chinese General Practice ›› 2026, Vol. 29 ›› Issue (18): 2498-2503.DOI: 10.12114/j.issn.1007-9572.2025.0021
• Article • Previous Articles Next Articles
Received:2025-01-13
Revised:2025-06-02
Published:2026-06-20
Online:2026-05-21
Contact:
HU Min
通讯作者:
胡敏
作者简介:作者贡献:
胡敏进行研究方案设计、数据收集整理、统计分析、论文撰写,对文章整体负责;吕向东提出研究思路,审校论文,监督管理。
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2025.0021
| AI诊断 | 医师诊断 | 合计 | |||
|---|---|---|---|---|---|
| 正常 | 采集不良 | 阳性 | 危急 | ||
| 正常 | 80(14.4) | 0 | 8(1.5) | 0 | 88(15.9) |
| 采集不良 | 0 | 5(0.9) | 0 | 0 | 5(0.9) |
| 阳性 | 32(5.8) | 0 | 374(67.6) | 1(0.2) | 407(73.6) |
| 危急 | 0 | 0 | 0 | 53(9.6) | 53(9.6) |
| 合计 | 112(20.2) | 5(0.9) | 382(69.1) | 54(9.8) | 553(100.0) |
Table 1 Diagnosis differences between AI-based and physician-based interpretation results of ECGs of inpatients transferred to tertiary hospital
| AI诊断 | 医师诊断 | 合计 | |||
|---|---|---|---|---|---|
| 正常 | 采集不良 | 阳性 | 危急 | ||
| 正常 | 80(14.4) | 0 | 8(1.5) | 0 | 88(15.9) |
| 采集不良 | 0 | 5(0.9) | 0 | 0 | 5(0.9) |
| 阳性 | 32(5.8) | 0 | 374(67.6) | 1(0.2) | 407(73.6) |
| 危急 | 0 | 0 | 0 | 53(9.6) | 53(9.6) |
| 合计 | 112(20.2) | 5(0.9) | 382(69.1) | 54(9.8) | 553(100.0) |
| AI诊断 | 医师诊断 | 合计 | |||
|---|---|---|---|---|---|
| 正常 | 采集不良 | 阳性 | 危急 | ||
| 正常 | 4 247(23.4) | 7(0.0) | 469(2.6) | 0 | 4 723(26.0) |
| 采集不良 | 0 | 190(1.0) | 0 | 0 | 190(1.0) |
| 阳性 | 1 624(8.9) | 11(0.1) | 11 207(61.7) | 19(0.1) | 12 861(70.8) |
| 危急 | 2(0.0) | 12(0.1) | 2(0.0) | 374(2.1) | 390(2.1) |
| 合计 | 5 873(32.3) | 220(1.2) | 11 678(64.3) | 393(2.2) | 18 164(100.0) |
Table 2 Diagnosis differences between AI-based and physician-based interpretation results of all consultation ECGs
| AI诊断 | 医师诊断 | 合计 | |||
|---|---|---|---|---|---|
| 正常 | 采集不良 | 阳性 | 危急 | ||
| 正常 | 4 247(23.4) | 7(0.0) | 469(2.6) | 0 | 4 723(26.0) |
| 采集不良 | 0 | 190(1.0) | 0 | 0 | 190(1.0) |
| 阳性 | 1 624(8.9) | 11(0.1) | 11 207(61.7) | 19(0.1) | 12 861(70.8) |
| 危急 | 2(0.0) | 12(0.1) | 2(0.0) | 374(2.1) | 390(2.1) |
| 合计 | 5 873(32.3) | 220(1.2) | 11 678(64.3) | 393(2.2) | 18 164(100.0) |
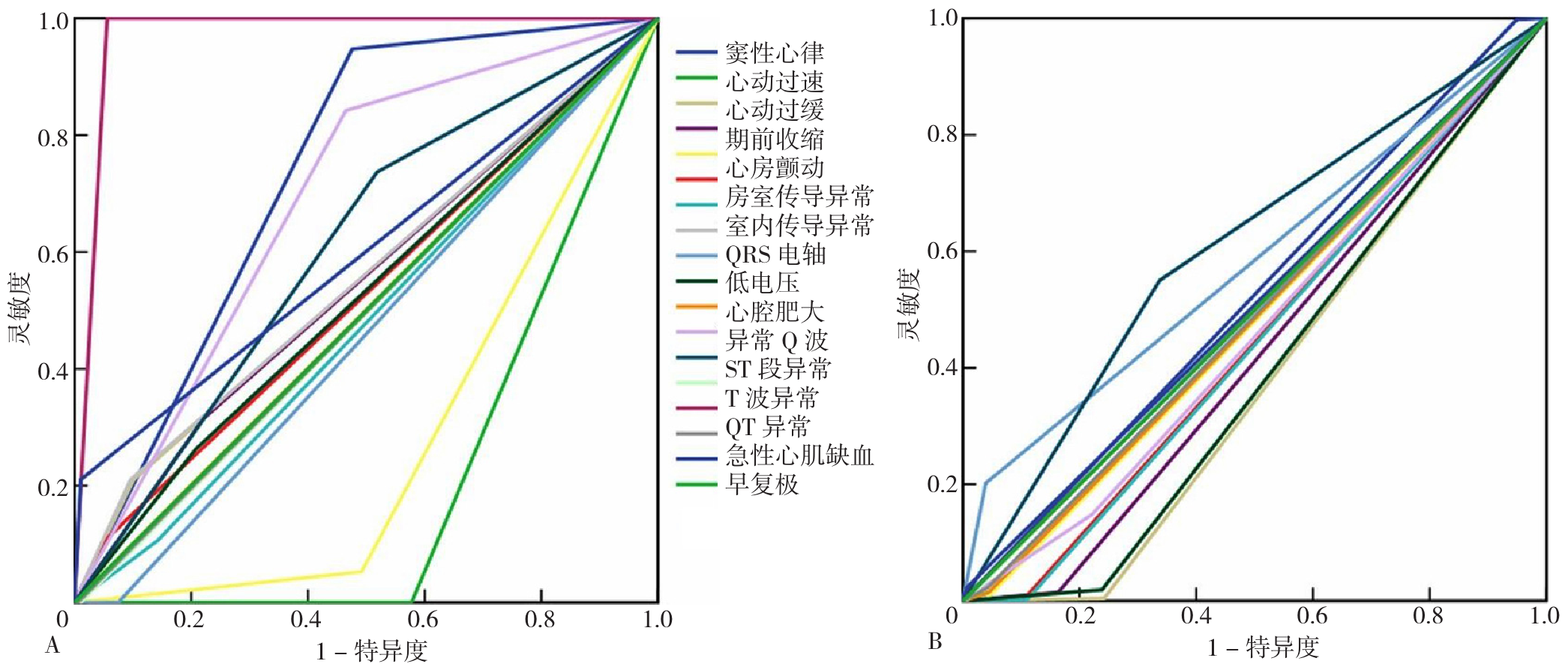
Figure 1 ROC curves of each ECG indicator in the critical and positive class ECG of the physician group for AI inconsistent with the physician classification
| 心电图指标 | 危急类AUC(95%CI) | 阳性类AUC(95%CI) |
|---|---|---|
| 窦性心律 | 0.74(0.65~0.82)a | 0.52(0.50~0.55) |
| 心动过速 | 0.21(0.15~0.27)a | 0.48(0.46~0.51) |
| 心动过缓 | 0.55(0.41~0.70) | 0.38(0.36~0.40)a |
| 期前收缩 | 0.55(0.41~0.68) | 0.43(0.40~0.45)a |
| 心房颤动 | 0.28(0.19~0.37)a | 0.48(0.46~0.51) |
| 房室传导异常 | 0.53(0.39~0.67) | 0.45(0.42~0.47)a |
| 室内传导异常 | 0.48(0.35~0.61) | 0.45(0.42~0.47)a |
| QRS电轴 | 0.56(0.42~0.70) | 0.49(0.46~0.51) |
| 低电压 | 0.46(0.34~0.59) | 0.58(0.55~0.61)a |
| 心腔肥大 | 0.53(0.39~0.66) | 0.39(0.37~0.41)a |
| 异常Q波 | 0.50(0.37~0.63) | 0.49(0.46~0.51) |
| ST段异常 | 0.69(0.58~0.80)a | 0.46(0.44~0.49)a |
| T波异常 | 0.61(0.49~0.73) | 0.61(0.58~0.63)a |
| QT异常 | 0.49(0.36~0.63) | 0.50(0.47~0.52) |
| 急性心肌缺血 | 0.97(0.96~0.99)a | 0.50(0.47~0.53) |
| 早复极 | 0.50(0.36~0.63) | 0.49(0.46~0.52) |
| 其他 | 0.60(0.45~0.75) | 0.51(0.48~0.54) |
Table 3 The impact of ECG entities on inconsistent diagnosis between the two groups with stratified by physician group classification results
| 心电图指标 | 危急类AUC(95%CI) | 阳性类AUC(95%CI) |
|---|---|---|
| 窦性心律 | 0.74(0.65~0.82)a | 0.52(0.50~0.55) |
| 心动过速 | 0.21(0.15~0.27)a | 0.48(0.46~0.51) |
| 心动过缓 | 0.55(0.41~0.70) | 0.38(0.36~0.40)a |
| 期前收缩 | 0.55(0.41~0.68) | 0.43(0.40~0.45)a |
| 心房颤动 | 0.28(0.19~0.37)a | 0.48(0.46~0.51) |
| 房室传导异常 | 0.53(0.39~0.67) | 0.45(0.42~0.47)a |
| 室内传导异常 | 0.48(0.35~0.61) | 0.45(0.42~0.47)a |
| QRS电轴 | 0.56(0.42~0.70) | 0.49(0.46~0.51) |
| 低电压 | 0.46(0.34~0.59) | 0.58(0.55~0.61)a |
| 心腔肥大 | 0.53(0.39~0.66) | 0.39(0.37~0.41)a |
| 异常Q波 | 0.50(0.37~0.63) | 0.49(0.46~0.51) |
| ST段异常 | 0.69(0.58~0.80)a | 0.46(0.44~0.49)a |
| T波异常 | 0.61(0.49~0.73) | 0.61(0.58~0.63)a |
| QT异常 | 0.49(0.36~0.63) | 0.50(0.47~0.52) |
| 急性心肌缺血 | 0.97(0.96~0.99)a | 0.50(0.47~0.53) |
| 早复极 | 0.50(0.36~0.63) | 0.49(0.46~0.52) |
| 其他 | 0.60(0.45~0.75) | 0.51(0.48~0.54) |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
张海澄, 余新艳, 王红宇, 等. 远程心电筛查助力分级诊疗的管理难点及瓶颈[J]. 中国全科医学, 2023, 26(5): 525-531, 540. DOI: 10.12114/j.issn.1007-9572.2022.L0002.
|
| [6] |
余新艳, 顾志乐, 张晓娟, 等. 人工智能在远程心电云平台辅助决策基层危急值心电图中的应用价值研究[J]. 中国全科医学, 2022, 25(11): 1363-1367, 1372. DOI: 10.12114/j.issn.1007-9572.2021.01.411.
|
| [7] |
心电图危急值2017中国专家共识——中国心电学会危急值专家工作组[J]. 临床心电学杂志, 2017, 26(6): 401-402.
|
| [8] |
全军心血管专业委员会心脏无创检测学组《心电图诊断术语规范化中国专家共识》编写专家组, 郭继鸿, 王思让, 等. 心电图诊断术语规范化中国专家共识(2019)[J]. 实用心电学杂志, 2019, 28(3): 161-165. DOI: 10.13308/j.issn.2095-9354.2019.03.002.
|
| [9] |
《远程心电图诊断危险分级中国专家共识》编写专家组, 郭继鸿, 陈韵岱, 等. 远程心电图危险分级诊断的中国专家共识[J]. 临床心电学杂志, 2022, 31(6): 401-405.
|
| [10] |
国家心血管病中心. 中国心血管健康与疾病报告-2023, 2023[M]. 北京: 中国协和医科大学出版社, 2024: 1-12.
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
周伊恒, 杨梓钰, 吕垚, 等. 美国心脏协会指南解读系列——《人工智能在心血管疾病中的应用科学声明》解读[J]. 中国全科医学, 2024, 27(35): 4353-4357. DOI: 10.12114/j.issn.1007-9572.2024.0192.
|
| [16] |
|
| [17] |
|
| [18] |
|
| [1] | REYILAI· Maimaiti, ZHOU Yiran, WU Yun, LIU Zhencheng, LU Yaoqin, WU Haiyan. Association between Novel Obesity Indicators and Cardiovascular Disease Risk in Hypertensive Patients [J]. Chinese General Practice, 2026, 29(20): 2836-2845. |
| [2] | ZHEN Rui, GU Xufang, GAO Shengwei, ZHANG Bowen, REN Zhenjuan, YANG Ruixuan. Burden of Cardiovascular Diseases Attributable to Metabolic Risk Factors in China 1990—2021 and Projected Trends from 2022 to 2035 [J]. Chinese General Practice, 2026, 29(15): 2077-2083. |
| [3] | QIU Yanli, GAO Yongyin, BIAN Xueyan, WANG Xue, LI Yue. The Predictive Value of Estimated Pulse Wave Velocity for All-cause and Cardiovascular-related Mortality in Cancer Patients [J]. Chinese General Practice, 2026, 29(14): 1890-1897. |
| [4] | XU Qinghong, WANG Jing, HUANG Yuan, ZHU Ci, CAO Wenbing, LI Ying. A Validation Study on Measuring Colorectal Polyp Size Using a Deep Learning-based Real-time Colorectal Polyp Measurement System [J]. Chinese General Practice, 2026, 29(14): 1873-1877. |
| [5] | ZHANG Hanyu, GU Jie, LIN Yingnan, HUANG Yanyan. Discussion on the Application of AI-based Simulated-scenario Standardized Patients in the Standardized Training Teaching of General Practice Resident Physicians [J]. Chinese General Practice, 2026, 29(13): 1726-1731. |
| [6] | YANG Lei, GUAN Hua. Application Progress of Generative Artificial Intelligence in Weight Management [J]. Chinese General Practice, 2026, 29(12): 1533-1540. |
| [7] | YANG Xu, FAN Jieting, SONG Hongyan, FENG Panpan, HAO Jingyu, YAO Mi. Risk Assessment and Communication Strategies for Cardiovascular Diseases in Primary Care [J]. Chinese General Practice, 2026, 29(10): 1294-1299. |
| [8] | LI Qiuchun, SU Ping, PANG Jinhong, CHEN Qiaoqiao, ZHAO Yingying, HE Ruiyan, WANG Yue, CHEN Xueyu, QIAO Junpeng, CHI Weiwei. Association of Triglyceride Glucose Index with Cardiovascular Disease in Cardiovascular-Kidney-Metabolic Syndrome Stage 0-3 Population: a Prospective Cohort Study [J]. Chinese General Practice, 2026, 29(09): 1129-1136. |
| [9] | PEI Zhiyi, ZHANG Xiaoxin, LIN Jiayi, ZHANG Xiangyi, KANG Xiaofeng. Systematic Review of the Quality and Application of Patient Decision Aids in Cardiovascular Disease Based on IPDAS 4.0 Criteria [J]. Chinese General Practice, 2026, 29(07): 945-952. |
| [10] | Expert Panel of the Consensus on Artificial Intelligence Empowering Healthcare Services. Artificial Intelligence Empowering Healthcare Services: Expert Consensus from the Mangrove Health Conference in 2025 [J]. Chinese General Practice, 2026, 29(07): 817-822. |
| [11] | WANG Lina, LEI Jingshu, LI Kuibao, WANG Ruiying, LI Xinmiao, WANG Fangfang, GUO Xiaorong, NIU Ruihao, ZHAO Wei, ZHOU Fangfang, ZHAO Jingjing, LEE CHONGYOU. Review on Inflammatory Response in Patients with Acute Myocardial Infarction [J]. Chinese General Practice, 2026, 29(06): 790-801. |
| [12] | XIA Ying, WU Xinri, ZHANG Caiqin, HONG Xin. Distribution and Influencing Factors of Cardiovascular Health among Community Residents Based on the "Life's Essential 8" Score [J]. Chinese General Practice, 2026, 29(05): 597-605. |
| [13] | LI Xi, LIU Jue. Artificial Intelligence Empowers Primary Healthcare Services: Progress and Challenges [J]. Chinese General Practice, 2026, 29(04): 436-443. |
| [14] | LU Yanqiu, WU Yuntao, LIU Shaopeng, LIN Haiying, DENG Huiyou, WU Ying, HUANG Zhe, YANG Peng, WU Shouling, LI Yun. Effect of Blood Pressure Trajectory on Cardiovascular Disease in Population with High-normal Blood Pressure: a Study Based on the Kailuan Cohort [J]. Chinese General Practice, 2026, 29(03): 299-310. |
| [15] | FAN Zhuanzhuan, LI Wenting, MA Guoliang. Relationship between the Chinese Visceral Adipose Index and Cardiovascular Disease in Postmenopausal Women: a Prospective Cohort Study [J]. Chinese General Practice, 2026, 29(02): 180-187. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||