
Chinese General Practice ›› 2024, Vol. 27 ›› Issue (20): 2429-2436.DOI: 10.12114/j.issn.1007-9572.2024.0005
Special Issue: 指南/共识最新文章合辑
• Guidelines·Consensus • Next Articles
Received:2024-01-02
Revised:2024-01-23
Published:2024-07-15
Online:2024-04-08
CLC Number:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2024.0005
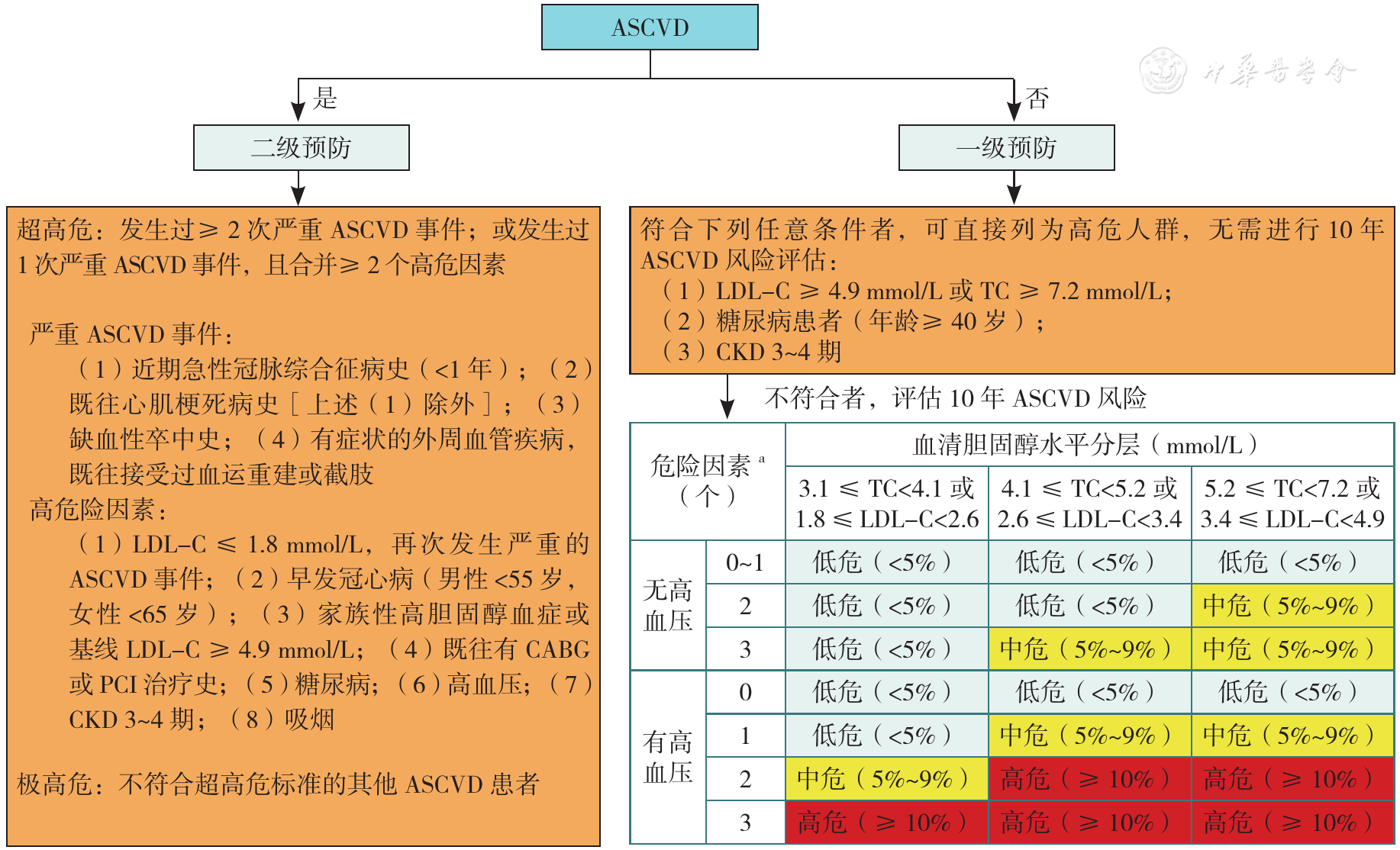
Figure 1 The risk assessment flow chart of ASCVD in Chinese adults
| 分类 | TC | LDL-C | HDL-C | TG | 非HDL-C |
|---|---|---|---|---|---|
| 理想水平 | — | <2.6 | — | — | <3.4 |
| 合适水平 | <5.2 | <3.4 | — | <1.7 | <4.1 |
| 边缘升高 | ≥5.2且<6.2 | ≥3.4且<4.1 | — | ≥1.7且<2.3 | ≥4.1且<4.9 |
| 升高 | ≥6.2 | ≥4.1 | — | ≥2.3 | ≥4.9 |
| 降低 | — | — | <1.0 | — | — |
Table 1 Reference values of blood lipids for the primary prevention of ASCVD in low-risk populations
| 分类 | TC | LDL-C | HDL-C | TG | 非HDL-C |
|---|---|---|---|---|---|
| 理想水平 | — | <2.6 | — | — | <3.4 |
| 合适水平 | <5.2 | <3.4 | — | <1.7 | <4.1 |
| 边缘升高 | ≥5.2且<6.2 | ≥3.4且<4.1 | — | ≥1.7且<2.3 | ≥4.1且<4.9 |
| 升高 | ≥6.2 | ≥4.1 | — | ≥2.3 | ≥4.9 |
| 降低 | — | — | <1.0 | — | — |
| ASCVD风险等级 | LDL-C推荐目标值(mmol/L) |
|---|---|
| 低危a | <3.4[ |
| 中、高危a | <2.6[ |
| 极高危 | <1.8且较基线降低幅度>50%[ |
| 超高危 | <1.4且较基线降低幅度>50%[ |
Table 2 The goal attainment values of LDL-C
| ASCVD风险等级 | LDL-C推荐目标值(mmol/L) |
|---|---|
| 低危a | <3.4[ |
| 中、高危a | <2.6[ |
| 极高危 | <1.8且较基线降低幅度>50%[ |
| 超高危 | <1.4且较基线降低幅度>50%[ |
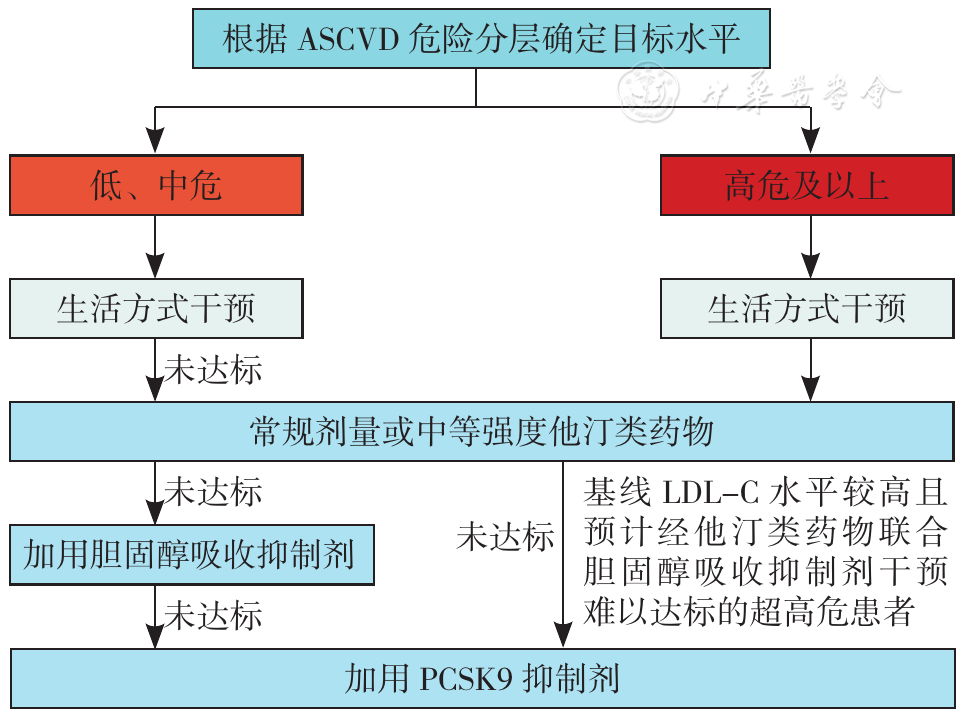
Figure 2 Flow chart of lipid-lowering strategy
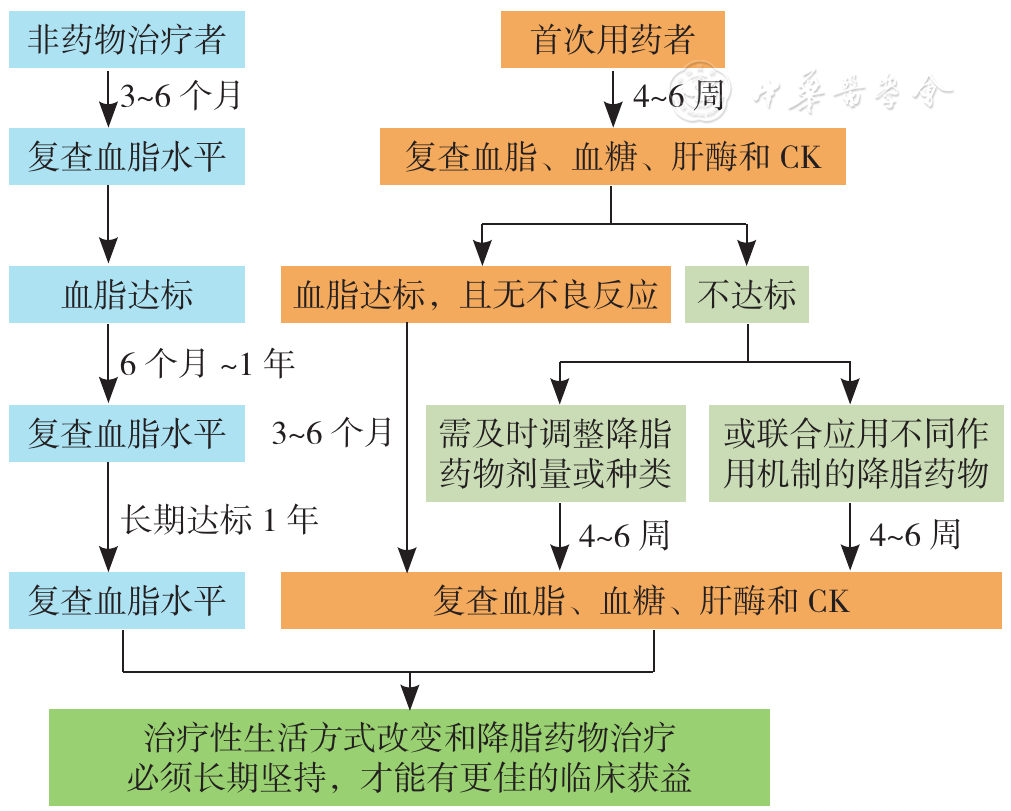
Figure 3 Monitoring flow chart of lipid-lowering treatment
| 降胆固醇强度 | 药物及其剂量 |
|---|---|
| 高强度(每日剂量可降低LDL-C≥50%) | 阿托伐他汀40~80 mg |
| 瑞舒伐他汀20 mg | |
| 中等强度(每日剂量可降低LDL-C 25%~<50%) | 阿托伐他汀10~20 mg |
| 瑞舒伐他汀5~10 mg | |
| 氟伐他汀80 mg | |
| 洛伐他汀40 mg | |
| 匹伐他汀1~4 mg | |
| 普伐他汀40 mg | |
| 辛伐他汀20~40 mg | |
| 血脂康1.2 g |
Table 3 The cholesterol reduction intensity of stains
| 降胆固醇强度 | 药物及其剂量 |
|---|---|
| 高强度(每日剂量可降低LDL-C≥50%) | 阿托伐他汀40~80 mg |
| 瑞舒伐他汀20 mg | |
| 中等强度(每日剂量可降低LDL-C 25%~<50%) | 阿托伐他汀10~20 mg |
| 瑞舒伐他汀5~10 mg | |
| 氟伐他汀80 mg | |
| 洛伐他汀40 mg | |
| 匹伐他汀1~4 mg | |
| 普伐他汀40 mg | |
| 辛伐他汀20~40 mg | |
| 血脂康1.2 g |
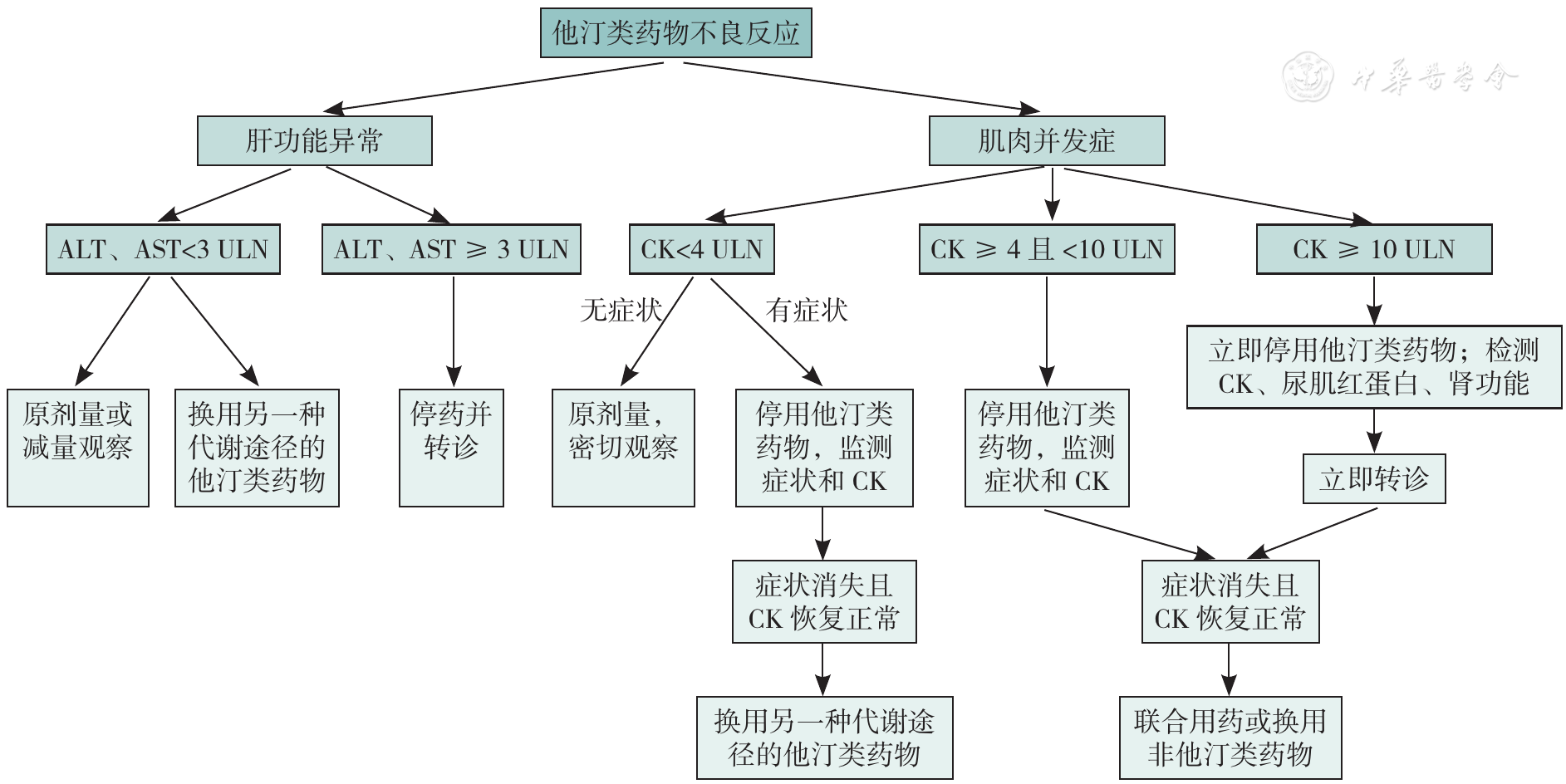
Figure 4 Management of adverse reactions to statins
| 药物分类 | 常用药物 | 剂量 | 不良反应 |
|---|---|---|---|
| 贝特类 | 非诺贝特片 | 0.1 g,3次/d | 包括肝脏、肌肉和肾毒性等 |
| 微粒化非诺贝特 | 0.2 g,1次/d | ||
| 非诺贝特缓释胶囊 | 0.25 g,1次/d | ||
| 苯扎贝特 | 0.2 g,3次/d | ||
| 苯扎贝特缓释片 | 0.4 g,1次/d | ||
| 吉非贝齐 | 0.6 g,2次/d | ||
| ω-3脂肪酸 | IPE | 1~4 g/d | 胃肠道反应,大剂量可能增加轻微出血、新发心房颤动风险 |
| EPA+DHA | |||
| 烟酸及其同类物 | 烟酸缓释片 | 0.375~1.000 g,1次/d | 颜面潮红、皮肤瘙痒、皮疹、肝脏损害、高尿酸血症、高血糖、棘皮症和消化道不适等 |
| 阿昔莫司 | 0.25~0.50 g,2次/d |
Table 4 Main TG-lowering drugs
| 药物分类 | 常用药物 | 剂量 | 不良反应 |
|---|---|---|---|
| 贝特类 | 非诺贝特片 | 0.1 g,3次/d | 包括肝脏、肌肉和肾毒性等 |
| 微粒化非诺贝特 | 0.2 g,1次/d | ||
| 非诺贝特缓释胶囊 | 0.25 g,1次/d | ||
| 苯扎贝特 | 0.2 g,3次/d | ||
| 苯扎贝特缓释片 | 0.4 g,1次/d | ||
| 吉非贝齐 | 0.6 g,2次/d | ||
| ω-3脂肪酸 | IPE | 1~4 g/d | 胃肠道反应,大剂量可能增加轻微出血、新发心房颤动风险 |
| EPA+DHA | |||
| 烟酸及其同类物 | 烟酸缓释片 | 0.375~1.000 g,1次/d | 颜面潮红、皮肤瘙痒、皮疹、肝脏损害、高尿酸血症、高血糖、棘皮症和消化道不适等 |
| 阿昔莫司 | 0.25~0.50 g,2次/d |
| 联合应用策略a | 适用情况 | 安全性关注点 |
|---|---|---|
| 他汀类药物+胆固醇吸收抑制剂 | 单药治疗后LDL-C不达标 | 常规监测 |
| 他汀类药物+PCSK9抑制剂 | 单药治疗后LDL-C不达标 | 常规监测 |
| 他汀类药物+胆固醇吸收抑制剂+PCSK9抑制剂 | 双联用药后LDL-C不达标 | 常规监测 |
| 他汀类药物+ω-3脂肪酸(IPE、EPA+DHA)或非诺贝特 | LDL-C达标、TG 2.3~5.7 mmol/L | 心房颤动、出血、肾功能 |
| 贝特类药物+ω-3脂肪酸(IPE、EPA+DHA) | 单药治疗后TG≥5.7 mmol/L | 常规监测 |
Table 5 Combination of lipid-lowering drugs
| 联合应用策略a | 适用情况 | 安全性关注点 |
|---|---|---|
| 他汀类药物+胆固醇吸收抑制剂 | 单药治疗后LDL-C不达标 | 常规监测 |
| 他汀类药物+PCSK9抑制剂 | 单药治疗后LDL-C不达标 | 常规监测 |
| 他汀类药物+胆固醇吸收抑制剂+PCSK9抑制剂 | 双联用药后LDL-C不达标 | 常规监测 |
| 他汀类药物+ω-3脂肪酸(IPE、EPA+DHA)或非诺贝特 | LDL-C达标、TG 2.3~5.7 mmol/L | 心房颤动、出血、肾功能 |
| 贝特类药物+ω-3脂肪酸(IPE、EPA+DHA) | 单药治疗后TG≥5.7 mmol/L | 常规监测 |
| [1] |
国家心血管病中心. 中国心血管健康与疾病报告2021[M]. 北京:科学出版社,2022.
|
| [2] |
|
| [3] |
国家卫生健康委员会疾病预防控制局. 中国居民营养与慢性病状况报告2015[M]. 北京:人民卫生出版社,2015.
|
| [4] |
中国血脂管理指南修订联合专家委员会. 中国血脂管理指南(2023年)[J]. 中国循环杂志,2023,38(3):237-271. DOI:10.3969/j.issn.1000-3614.2023.03.001.
|
| [5] |
Cholesterol Treatment Trialists Collaborators. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease:meta-analysis of individual data from 27 randomised trials[J]. Lancet,2012,380(9841):581-590. DOI:10.1016/S0140-6736(12)60367-5.
|
| [6] |
Cholesterol Treatment Trialists Collaboration. Efficacy and safety of LDL-lowering therapy among men and women:meta-analysis of individual data from 174 000 participants in 27 randomised trials[J]. Lancet,2015,385(9976):1397-1405. DOI:10.1016/S0140-6736(14)61368-4.
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
Accord Study Group. Effects of combination lipid therapy in type 2 diabetes mellitus[J]. N Engl J Med,2010,362(17):1563-1574. DOI:10.1056/NEJMoa1001282.
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
Cholesterol Treatment Trialists Collaborators. Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins:a meta-analysis[J]. Lancet,2008,371(9607):117-125. DOI:10.1016/S0140-6736(08)60104-X.
|
| [28] |
Cholesterol Treatment Trialists Collaboration. Impact of renal function on the effects of LDL cholesterol lowering with statin-based regimens:a meta-analysis of individual participant data from 28 randomised trials[J]. Lancet Diabetes Endocrinol,2016,4(10):829-839. DOI:10.1016/S2213-8587(16)30156-5.
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [1] | REYILAI· Maimaiti, ZHOU Yiran, WU Yun, LIU Zhencheng, LU Yaoqin, WU Haiyan. Association between Novel Obesity Indicators and Cardiovascular Disease Risk in Hypertensive Patients [J]. Chinese General Practice, 2026, 29(20): 2836-2845. |
| [2] | JIAN Yingchun, ZENG Yongqin, ZHANG Haiping, WANG Zhengdi, AN Ke, YAN Rui. Recent Advances in Mitochondrial Dysfunction in Chronic Metabolic Diseases [J]. Chinese General Practice, 2026, 29(18): 2577-2584. |
| [3] | HU Min, LYU Xiangdong. Accuracy of Artificial Intelligence in Remote Electrocardiography Diagnosis [J]. Chinese General Practice, 2026, 29(18): 2498-2503. |
| [4] | LIU Daiyue, LIU Xincan, LAN Zhenzhen. Research Progress on Postprandial Hyperlipidemia and Its Therapeutic Approaches [J]. Chinese General Practice, 2026, 29(18): 2546-2553. |
| [5] | XIANG Tong, YU Haiyan, LI Mingyue, GAO Wenjuan, ZHU Xiayuan, WU Hao. Analysis of Factors Influencing of Prediabetes Management Behaviors among Primary Care Physicians and Nurses: a Qualitative Study [J]. Chinese General Practice, 2026, 29(16): 2259-2263. |
| [6] | ZHEN Rui, GU Xufang, GAO Shengwei, ZHANG Bowen, REN Zhenjuan, YANG Ruixuan. Burden of Cardiovascular Diseases Attributable to Metabolic Risk Factors in China 1990—2021 and Projected Trends from 2022 to 2035 [J]. Chinese General Practice, 2026, 29(15): 2077-2083. |
| [7] | QIU Yanli, GAO Yongyin, BIAN Xueyan, WANG Xue, LI Yue. The Predictive Value of Estimated Pulse Wave Velocity for All-cause and Cardiovascular-related Mortality in Cancer Patients [J]. Chinese General Practice, 2026, 29(14): 1890-1897. |
| [8] | YANG Xu, FAN Jieting, SONG Hongyan, FENG Panpan, HAO Jingyu, YAO Mi. Risk Assessment and Communication Strategies for Cardiovascular Diseases in Primary Care [J]. Chinese General Practice, 2026, 29(10): 1294-1299. |
| [9] | LI Qiuchun, SU Ping, PANG Jinhong, CHEN Qiaoqiao, ZHAO Yingying, HE Ruiyan, WANG Yue, CHEN Xueyu, QIAO Junpeng, CHI Weiwei. Association of Triglyceride Glucose Index with Cardiovascular Disease in Cardiovascular-Kidney-Metabolic Syndrome Stage 0-3 Population: a Prospective Cohort Study [J]. Chinese General Practice, 2026, 29(09): 1129-1136. |
| [10] | SUN Qinyu, DENG Yifan, YANG Tianxiao, FANG Zhen, JI Jun, HE Shenghu, ZHANG Jing. Clinical Study of HbA1c/ApoA-1, TyG-BMI and Their Combination to Predict the Severity of Coronary Artery Calcification [J]. Chinese General Practice, 2026, 29(09): 1137-1145. |
| [11] | PEI Zhiyi, ZHANG Xiaoxin, LIN Jiayi, ZHANG Xiangyi, KANG Xiaofeng. Systematic Review of the Quality and Application of Patient Decision Aids in Cardiovascular Disease Based on IPDAS 4.0 Criteria [J]. Chinese General Practice, 2026, 29(07): 945-952. |
| [12] | LIU Fan, LI Jiali, KE Lixin, ZHANG Qiang, CHEN Jiahui, LU Cuncun, ZHAO Xinke. Disease Burden of Hypercholesterolemia among Individuals Aged 60 and above Globally and in China from 1990 to 2021: Trend Analysis and Model-based Projection [J]. Chinese General Practice, 2026, 29(05): 631-640. |
| [13] | XIA Ying, WU Xinri, ZHANG Caiqin, HONG Xin. Distribution and Influencing Factors of Cardiovascular Health among Community Residents Based on the "Life's Essential 8" Score [J]. Chinese General Practice, 2026, 29(05): 597-605. |
| [14] | LU Yanqiu, WU Yuntao, LIU Shaopeng, LIN Haiying, DENG Huiyou, WU Ying, HUANG Zhe, YANG Peng, WU Shouling, LI Yun. Effect of Blood Pressure Trajectory on Cardiovascular Disease in Population with High-normal Blood Pressure: a Study Based on the Kailuan Cohort [J]. Chinese General Practice, 2026, 29(03): 299-310. |
| [15] | FAN Zhuanzhuan, LI Wenting, MA Guoliang. Relationship between the Chinese Visceral Adipose Index and Cardiovascular Disease in Postmenopausal Women: a Prospective Cohort Study [J]. Chinese General Practice, 2026, 29(02): 180-187. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||