
Chinese General Practice ›› 2026, Vol. 29 ›› Issue (18): 2489-2497.DOI: 10.12114/j.issn.1007-9572.2024.0481
Special Issue: 心肌梗死最新文章合辑
• Article • Previous Articles
Received:2024-10-10
Revised:2025-08-24
Published:2026-06-20
Online:2026-05-21
Contact:
YANG Yining
通讯作者:
杨毅宁
作者简介:作者贡献:
袁玉娟提出主要研究目标,负责研究的构思与设计,研究的实施,统计学处理以及图、表的绘制与展示,撰写论文;袁玉娟、陶静、王颖进行数据的收集与整理;彭辉进行论文的修订;杨毅宁负责文章的质量控制与审查,对文章整体负责,监督管理。
基金资助:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2024.0481
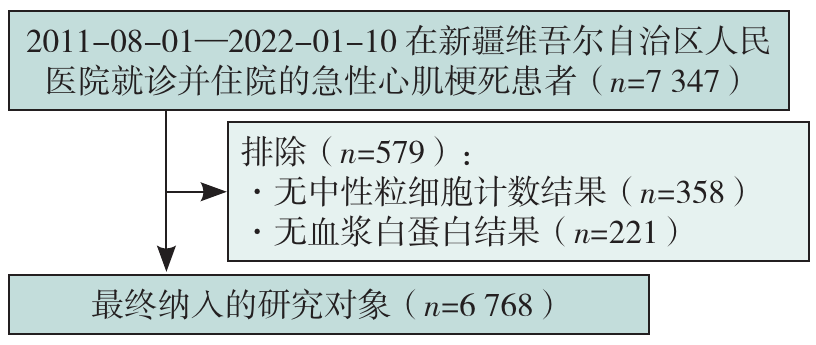
Figure 1 Flow chart of the inclusion of research objects
| 变量 | Q1组(n=1 753) | Q2组(n=1 694) | Q3组(n=1 624) | Q4组(n=1 697) | 检验统计量值 | P值 |
|---|---|---|---|---|---|---|
| 年龄( | 58.5±12.2 | 60.3±12.9 | 62.9±12.9 | 67.9±12.2 | 179.724a | <0.001 |
| 性别[例(%)] | 19.426b | <0.001 | ||||
| 男 | 1 362(77.7) | 1 329(78.5) | 1 211(74.6) | 1 236(72.8) | ||
| 女 | 391(22.3) | 365(21.5) | 413(25.4) | 461(27.2) | ||
| BMI( | 26.5±3.7 | 26.3±3.7 | 25.9±3.9 | 24.9±3.9 | 56.589a | <0.001 |
| 吸烟[例(%)] | 881(50.3) | 822(48.5) | 713(43.9) | 633(37.3) | 69.481b | <0.001 |
| 饮酒[例(%)] | 574(32.7) | 547(32.3) | 439(27.0) | 389(22.9) | 54.426b | <0.001 |
| DBP( | 79±14 | 79±15 | 77±15 | 74±16 | 34.995a | <0.001 |
| SBP( | 129±22 | 130±24 | 126±24 | 124±26 | 20.385a | <0.001 |
| 心率( | 79.9±13.7 | 82.2±16.6 | 85.8±18.9 | 90.9±21.1 | 34.865a | <0.001 |
| 脑卒中[例(%)] | 113(6.4) | 139(8.2) | 139(8.6) | 220(13.0) | 48.071b | <0.001 |
| 高血压[例(%)] | 945(53.9) | 985(58.1) | 923(56.8) | 1 019(60.0) | 14.090b | 0.003 |
| 2型糖尿病[例(%)] | 539(30.7) | 529(31.2) | 576(35.5) | 721(42.5) | 65.538b | <0.001 |
| 丙氨酸氨基转移酶[M(P25,P75),U/L] | 29.00(19.00,47.00) | 31.00(20.00,49.00) | 36.00(22.00,57.50) | 34.00(21.00,63.00) | 72.210 | <0.001 |
| 天冬氨酸氨基转移酶[M(P25,P75),U/L] | 27.00(19.00,46.00) | 37.55(23.00,80.00) | 60.00(28.00,167.00) | 56.00(26.00,146.12) | 564.938 | <0.001 |
| 血肌酐[M(P25,P75),μmol/L] | 71.90(62.20,84.50) | 72.00(61.40,86.70) | 72.05(60.80,92.60) | 86.80(65.80,142.40) | 270.619 | <0.001 |
| 血尿素氮[M(P25,P75),mmol/L] | 0.17(0.07,5.43) | 1.03(0.08,5.61) | 0.25(0.08,5.94) | 3.17(0.09,8.30) | 113.725 | <0.001 |
| 血尿酸( | 341.91±104.00 | 349.02±116.95 | 359.27±129.57 | 392.12±165.76 | 49.161a | <0.001 |
| 血钙[M(P25,P75),mmol/L] | 2.26±0.16 | 2.23±0.16 | 2.19±0.16 | 2.07±0.18 | 441.452a | <0.001 |
| 血钾( | 4.01±0.46 | 4.01±0.51 | 4.07±0.56 | 4.19±0.75 | 38.418a | <0.001 |
| 超敏C反应蛋白[M(P25,P75),mg/dL] | 4.06(1.46,11.58) | 6.17(2.08,18.92) | 7.37(2.51,26.12) | 23.00(5.01,75.49) | 671.300 | <0.001 |
| TG( | 1.82±1.33 | 1.69±1.39 | 1.48±0.98 | 1.41±0.94 | 43.682a | <0.001 |
| TC( | 4.21±1.15 | 4.30±1.16 | 4.27±1.17 | 3.94±1.22 | 33.263a | <0.001 |
| 低密度脂蛋白胆固醇( | 2.53±0.95 | 2.63±0.96 | 2.62±0.98 | 2.37±0.99 | 25.135a | <0.001 |
| 高密度脂蛋白胆固醇( | 0.95±0.26 | 0.96±0.27 | 1.01±0.29 | 0.93±0.32 | 22.412a | <0.001 |
| 肌钙蛋白T[M(P25,P75),ng/mL] | 0.24(0.06,0.87) | 0.50(0.15,1.43) | 1.04(0.26,3.32) | 1.14(0.28,3.75) | 629.855 | <0.001 |
| 肌钙蛋白I[M(P25,P75),ng/mL] | 1.01(0.12,5.36) | 2.70(0.39,11.20) | 6.46(0.83,27.54) | 5.21(0.78,23.40) | 482.805 | <0.001 |
| 肌酸激酶[M(P25,P75),U/L] | 115.00(63.00,298.00) | 220.00(91.00,715.00) | 506.00(141.00,1 523.00) | 414.00(135.00,1 240.00) | 684.886 | <0.001 |
| 肌酸激酶同工酶[M(P25,P75),ng/mL] | 14.10(2.75,29.90) | 19.16(4.85,56.30) | 30.63(7.61,103.00) | 23.20(6.24,76.00) | 289.419 | <0.001 |
| D-二聚体[M(P25,P75),mg/L] | 0.36(0.22,0.68) | 0.40(0.24,0.86) | 0.60(0.30,1.41) | 1.42(0.58,3.35) | 1 057.994 | <0.001 |
| 白蛋白( | 45.13±8.78 | 39.53±3.98 | 37.75±3.72 | 31.78±4.75 | 1 586.650a | <0.001 |
| 白细胞计数[M(P25,P75),×109/L] | 7.54(6.19,9.30) | 8.84(6.94,11.16) | 10.49(8.11,13.38) | 11.04(8.40,14.57) | 954.139 | <0.001 |
| 中性粒细胞计数( | 5.17±2.64 | 7.02±3.05 | 9.30±4.09 | 10.58±5.26 | 657.625a | <0.001 |
| 中性粒细胞计数百分比( | 61.90±10.60 | 73.16±7.96 | 82.05±8.07 | 85.97±7.39 | 2 643.841a | <0.001 |
| 淋巴细胞计数[M(P25,P75),×109/L] | 2.05(1.63,2.56) | 1.62(1.25,2.03) | 1.15(0.84,1.52) | 0.84(0.57,1.20) | 2 577.833 | <0.001 |
| 单核细胞计数[M(P25,P75),×109/L] | 0.49(0.37,0.64) | 0.51(0.37,0.69) | 0.45(0.28,0.69) | 0.46(0.27,0.69) | 63.891 | <0.001 |
| 血小板计数( | 245.17±78.80 | 240.93±78.31 | 238.38±83.91 | 229.95±105.74 | 9.244a | <0.001 |
| ACEI/ARB[例(%)] | 384(21.9) | 295(17.4) | 281(17.3) | 287(16.9) | 19.222b | <0.001 |
| β受体阻滞剂[例(%)] | 161(9.2) | 134(7.9) | 99(6.1) | 113(6.7) | 13.938b | 0.003 |
| 钙通道阻滞剂[例(%)] | 330(18.8) | 368(21.7) | 345(21.2) | 372(21.9) | 6.446b | 0.092 |
| 利尿剂[例(%)] | 65(3.7) | 59(3.5) | 80(4.9) | 107(6.3) | 19.654b | <0.001 |
| 抗血小板药物[例(%)] | 444(25.3) | 346(20.4) | 313(19.3) | 322(19.0) | 27.180b | <0.001 |
| 他汀类药物[例(%)] | 313(17.9) | 239(14.1) | 190(11.7) | 193(11.4) | 38.758b | <0.001 |
| 急性心肌梗死分型[例(%)] | 33.510b | <0.001 | ||||
| STEMI | 1 031(58.8) | 934(55.1) | 1 054(64.9) | 1 017(59.9) | ||
| NSTEMI | 722(41.2) | 760(44.9) | 570(35.1) | 680(40.1) | ||
| 冠状动脉血管再灌注治疗[例(%)] | 840(47.9) | 851(50.2) | 749(46.1) | 530(31.2) | 152.955b | <0.001 |
| 全因死亡[例(%)] | 96(5.5) | 126(7.4) | 184(11.3) | 359(21.2) | 248.698b | <0.001 |
| 心源性休克[例(%)] | 66(3.8) | 105(6.2) | 194(11.9) | 344(20.3) | 294.586b | <0.001 |
| VT或VF[例(%)] | 58(3.3) | 70(4.1) | 106(6.5) | 146(8.6) | 55.772b | <0.001 |
| 房室传导阻滞[例(%)] | 25(1.4) | 23(1.4) | 49(3.0) | 61(3.6) | 28.571b | <0.001 |
| 新发脑卒中[例(%)] | 15(0.9) | 23(1.4) | 29(1.8) | 52(3.1) | 26.604b | <0.001 |
Table 1 Comparison of baseline data of patients among 4 groups
| 变量 | Q1组(n=1 753) | Q2组(n=1 694) | Q3组(n=1 624) | Q4组(n=1 697) | 检验统计量值 | P值 |
|---|---|---|---|---|---|---|
| 年龄( | 58.5±12.2 | 60.3±12.9 | 62.9±12.9 | 67.9±12.2 | 179.724a | <0.001 |
| 性别[例(%)] | 19.426b | <0.001 | ||||
| 男 | 1 362(77.7) | 1 329(78.5) | 1 211(74.6) | 1 236(72.8) | ||
| 女 | 391(22.3) | 365(21.5) | 413(25.4) | 461(27.2) | ||
| BMI( | 26.5±3.7 | 26.3±3.7 | 25.9±3.9 | 24.9±3.9 | 56.589a | <0.001 |
| 吸烟[例(%)] | 881(50.3) | 822(48.5) | 713(43.9) | 633(37.3) | 69.481b | <0.001 |
| 饮酒[例(%)] | 574(32.7) | 547(32.3) | 439(27.0) | 389(22.9) | 54.426b | <0.001 |
| DBP( | 79±14 | 79±15 | 77±15 | 74±16 | 34.995a | <0.001 |
| SBP( | 129±22 | 130±24 | 126±24 | 124±26 | 20.385a | <0.001 |
| 心率( | 79.9±13.7 | 82.2±16.6 | 85.8±18.9 | 90.9±21.1 | 34.865a | <0.001 |
| 脑卒中[例(%)] | 113(6.4) | 139(8.2) | 139(8.6) | 220(13.0) | 48.071b | <0.001 |
| 高血压[例(%)] | 945(53.9) | 985(58.1) | 923(56.8) | 1 019(60.0) | 14.090b | 0.003 |
| 2型糖尿病[例(%)] | 539(30.7) | 529(31.2) | 576(35.5) | 721(42.5) | 65.538b | <0.001 |
| 丙氨酸氨基转移酶[M(P25,P75),U/L] | 29.00(19.00,47.00) | 31.00(20.00,49.00) | 36.00(22.00,57.50) | 34.00(21.00,63.00) | 72.210 | <0.001 |
| 天冬氨酸氨基转移酶[M(P25,P75),U/L] | 27.00(19.00,46.00) | 37.55(23.00,80.00) | 60.00(28.00,167.00) | 56.00(26.00,146.12) | 564.938 | <0.001 |
| 血肌酐[M(P25,P75),μmol/L] | 71.90(62.20,84.50) | 72.00(61.40,86.70) | 72.05(60.80,92.60) | 86.80(65.80,142.40) | 270.619 | <0.001 |
| 血尿素氮[M(P25,P75),mmol/L] | 0.17(0.07,5.43) | 1.03(0.08,5.61) | 0.25(0.08,5.94) | 3.17(0.09,8.30) | 113.725 | <0.001 |
| 血尿酸( | 341.91±104.00 | 349.02±116.95 | 359.27±129.57 | 392.12±165.76 | 49.161a | <0.001 |
| 血钙[M(P25,P75),mmol/L] | 2.26±0.16 | 2.23±0.16 | 2.19±0.16 | 2.07±0.18 | 441.452a | <0.001 |
| 血钾( | 4.01±0.46 | 4.01±0.51 | 4.07±0.56 | 4.19±0.75 | 38.418a | <0.001 |
| 超敏C反应蛋白[M(P25,P75),mg/dL] | 4.06(1.46,11.58) | 6.17(2.08,18.92) | 7.37(2.51,26.12) | 23.00(5.01,75.49) | 671.300 | <0.001 |
| TG( | 1.82±1.33 | 1.69±1.39 | 1.48±0.98 | 1.41±0.94 | 43.682a | <0.001 |
| TC( | 4.21±1.15 | 4.30±1.16 | 4.27±1.17 | 3.94±1.22 | 33.263a | <0.001 |
| 低密度脂蛋白胆固醇( | 2.53±0.95 | 2.63±0.96 | 2.62±0.98 | 2.37±0.99 | 25.135a | <0.001 |
| 高密度脂蛋白胆固醇( | 0.95±0.26 | 0.96±0.27 | 1.01±0.29 | 0.93±0.32 | 22.412a | <0.001 |
| 肌钙蛋白T[M(P25,P75),ng/mL] | 0.24(0.06,0.87) | 0.50(0.15,1.43) | 1.04(0.26,3.32) | 1.14(0.28,3.75) | 629.855 | <0.001 |
| 肌钙蛋白I[M(P25,P75),ng/mL] | 1.01(0.12,5.36) | 2.70(0.39,11.20) | 6.46(0.83,27.54) | 5.21(0.78,23.40) | 482.805 | <0.001 |
| 肌酸激酶[M(P25,P75),U/L] | 115.00(63.00,298.00) | 220.00(91.00,715.00) | 506.00(141.00,1 523.00) | 414.00(135.00,1 240.00) | 684.886 | <0.001 |
| 肌酸激酶同工酶[M(P25,P75),ng/mL] | 14.10(2.75,29.90) | 19.16(4.85,56.30) | 30.63(7.61,103.00) | 23.20(6.24,76.00) | 289.419 | <0.001 |
| D-二聚体[M(P25,P75),mg/L] | 0.36(0.22,0.68) | 0.40(0.24,0.86) | 0.60(0.30,1.41) | 1.42(0.58,3.35) | 1 057.994 | <0.001 |
| 白蛋白( | 45.13±8.78 | 39.53±3.98 | 37.75±3.72 | 31.78±4.75 | 1 586.650a | <0.001 |
| 白细胞计数[M(P25,P75),×109/L] | 7.54(6.19,9.30) | 8.84(6.94,11.16) | 10.49(8.11,13.38) | 11.04(8.40,14.57) | 954.139 | <0.001 |
| 中性粒细胞计数( | 5.17±2.64 | 7.02±3.05 | 9.30±4.09 | 10.58±5.26 | 657.625a | <0.001 |
| 中性粒细胞计数百分比( | 61.90±10.60 | 73.16±7.96 | 82.05±8.07 | 85.97±7.39 | 2 643.841a | <0.001 |
| 淋巴细胞计数[M(P25,P75),×109/L] | 2.05(1.63,2.56) | 1.62(1.25,2.03) | 1.15(0.84,1.52) | 0.84(0.57,1.20) | 2 577.833 | <0.001 |
| 单核细胞计数[M(P25,P75),×109/L] | 0.49(0.37,0.64) | 0.51(0.37,0.69) | 0.45(0.28,0.69) | 0.46(0.27,0.69) | 63.891 | <0.001 |
| 血小板计数( | 245.17±78.80 | 240.93±78.31 | 238.38±83.91 | 229.95±105.74 | 9.244a | <0.001 |
| ACEI/ARB[例(%)] | 384(21.9) | 295(17.4) | 281(17.3) | 287(16.9) | 19.222b | <0.001 |
| β受体阻滞剂[例(%)] | 161(9.2) | 134(7.9) | 99(6.1) | 113(6.7) | 13.938b | 0.003 |
| 钙通道阻滞剂[例(%)] | 330(18.8) | 368(21.7) | 345(21.2) | 372(21.9) | 6.446b | 0.092 |
| 利尿剂[例(%)] | 65(3.7) | 59(3.5) | 80(4.9) | 107(6.3) | 19.654b | <0.001 |
| 抗血小板药物[例(%)] | 444(25.3) | 346(20.4) | 313(19.3) | 322(19.0) | 27.180b | <0.001 |
| 他汀类药物[例(%)] | 313(17.9) | 239(14.1) | 190(11.7) | 193(11.4) | 38.758b | <0.001 |
| 急性心肌梗死分型[例(%)] | 33.510b | <0.001 | ||||
| STEMI | 1 031(58.8) | 934(55.1) | 1 054(64.9) | 1 017(59.9) | ||
| NSTEMI | 722(41.2) | 760(44.9) | 570(35.1) | 680(40.1) | ||
| 冠状动脉血管再灌注治疗[例(%)] | 840(47.9) | 851(50.2) | 749(46.1) | 530(31.2) | 152.955b | <0.001 |
| 全因死亡[例(%)] | 96(5.5) | 126(7.4) | 184(11.3) | 359(21.2) | 248.698b | <0.001 |
| 心源性休克[例(%)] | 66(3.8) | 105(6.2) | 194(11.9) | 344(20.3) | 294.586b | <0.001 |
| VT或VF[例(%)] | 58(3.3) | 70(4.1) | 106(6.5) | 146(8.6) | 55.772b | <0.001 |
| 房室传导阻滞[例(%)] | 25(1.4) | 23(1.4) | 49(3.0) | 61(3.6) | 28.571b | <0.001 |
| 新发脑卒中[例(%)] | 15(0.9) | 23(1.4) | 29(1.8) | 52(3.1) | 26.604b | <0.001 |
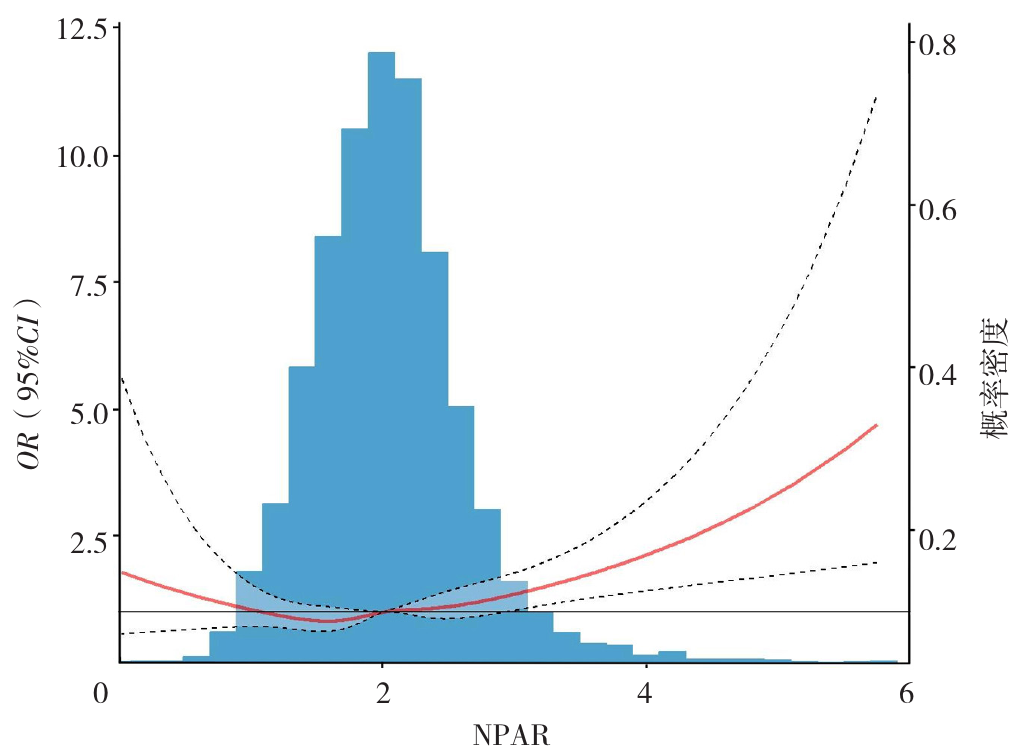
Figure 2 Dose-response relationship between NPAR and in-hospital all-cause mortality risk
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.79(1.67~1.93) | <0.001 | 1.60(1.48~1.72) | <0.001 | 1.18(1.08~1.29) | <0.001 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.007 | |||
| Q2组 | 1.39(1.06~1.83) | 0.019 | 1.27(0.96~1.68) | 0.091 | 1.19(0.89~1.60) | 0.246 |
| Q3组 | 2.21(1.71~2.86) | <0.001 | 1.81(1.39~2.35) | <0.001 | 1.27(0.96~1.69) | 0.102 |
| Q4组 | 4.63(3.67~5.89) | <0.001 | 3.14(2.47~4.03) | <0.001 | 1.48(1.11~1.97) | 0.008 |
Table 2 Multivariate Logistic regression analysis of NPAR on in-hospital all-cause mortality in AMI patients
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.79(1.67~1.93) | <0.001 | 1.60(1.48~1.72) | <0.001 | 1.18(1.08~1.29) | <0.001 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.007 | |||
| Q2组 | 1.39(1.06~1.83) | 0.019 | 1.27(0.96~1.68) | 0.091 | 1.19(0.89~1.60) | 0.246 |
| Q3组 | 2.21(1.71~2.86) | <0.001 | 1.81(1.39~2.35) | <0.001 | 1.27(0.96~1.69) | 0.102 |
| Q4组 | 4.63(3.67~5.89) | <0.001 | 3.14(2.47~4.03) | <0.001 | 1.48(1.11~1.97) | 0.008 |
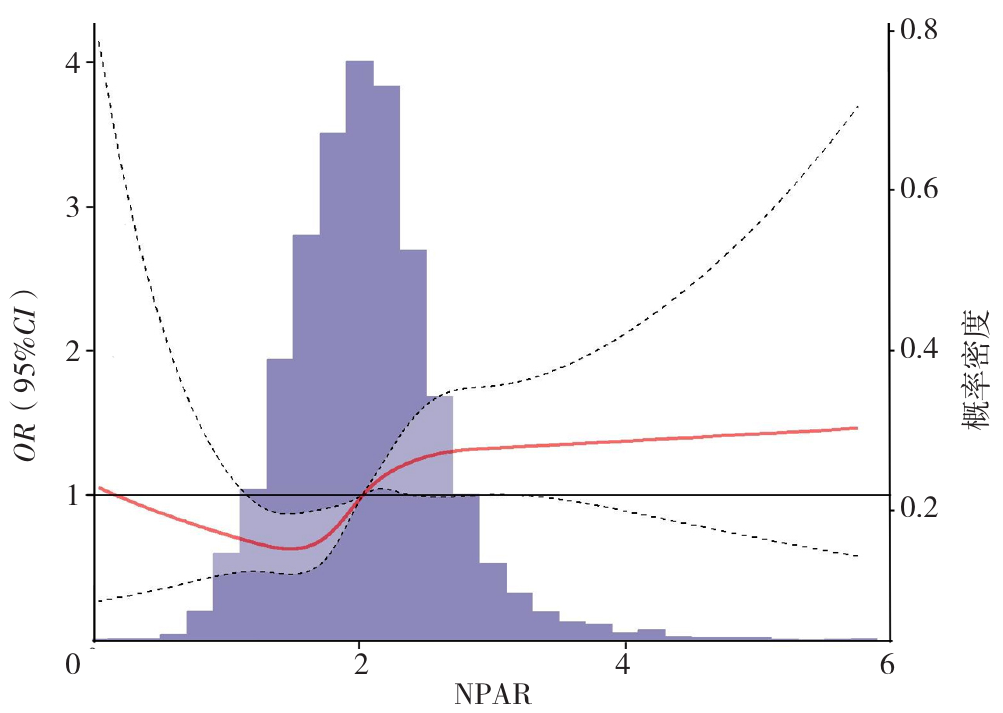
Figure 3 Dose-response relationship between NPAR and in-hospital cardiogenic shock risk
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.81(1.68~1.95) | <0.001 | 1.68(1.56~1.81) | <0.001 | 1.20(1.09~1.32) | <0.001 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | <0.001 | |||
| Q2组 | 1.69(1.24~2.32) | 0.001 | 1.62(1.18~2.23) | 0.003 | 1.41(1.01~1.97) | 0.044 |
| Q3组 | 3.47(2.61~4.66) | <0.001 | 3.11(2.34~4.18) | <0.001 | 1.85(1.36~2.54) | <0.001 |
| Q4组 | 6.50(4.98~8.60) | <0.001 | 5.20(3.96~6.93) | <0.001 | 2.09(1.53~2.89) | <0.001 |
Table 3 Multivariate Logistic regression analysis of NPAR on cardiogenic shock in AMI patients
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.81(1.68~1.95) | <0.001 | 1.68(1.56~1.81) | <0.001 | 1.20(1.09~1.32) | <0.001 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | <0.001 | |||
| Q2组 | 1.69(1.24~2.32) | 0.001 | 1.62(1.18~2.23) | 0.003 | 1.41(1.01~1.97) | 0.044 |
| Q3组 | 3.47(2.61~4.66) | <0.001 | 3.11(2.34~4.18) | <0.001 | 1.85(1.36~2.54) | <0.001 |
| Q4组 | 6.50(4.98~8.60) | <0.001 | 5.20(3.96~6.93) | <0.001 | 2.09(1.53~2.89) | <0.001 |
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.34(1.22~1.47) | <0.001 | 1.31(1.19~1.44) | <0.001 | 1.07(0.95~1.21) | 0.251 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.009 | |||
| Q2组 | 1.26(0.88~1.80) | 0.202 | 1.24(0.87~1.77) | 0.233 | 1.15(0.80~1.65) | 0.454 |
| Q3组 | 2.04(1.48~2.85) | <0.001 | 1.97(1.42~2.76) | <0.001 | 1.43(1.01~2.03) | 0.045 |
| Q4组 | 2.75(2.03~3.78) | <0.001 | 2.56(1.87~3.55) | <0.001 | 1.56(1.09~2.26) | 0.017 |
Table 4 Multivariate Logistic regression analysis of NPAR on ventricular tachycardia or ventricular fibrillation in AMI patients
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.34(1.22~1.47) | <0.001 | 1.31(1.19~1.44) | <0.001 | 1.07(0.95~1.21) | 0.251 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.009 | |||
| Q2组 | 1.26(0.88~1.80) | 0.202 | 1.24(0.87~1.77) | 0.233 | 1.15(0.80~1.65) | 0.454 |
| Q3组 | 2.04(1.48~2.85) | <0.001 | 1.97(1.42~2.76) | <0.001 | 1.43(1.01~2.03) | 0.045 |
| Q4组 | 2.75(2.03~3.78) | <0.001 | 2.56(1.87~3.55) | <0.001 | 1.56(1.09~2.26) | 0.017 |
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.34(1.16~1.53) | <0.001 | 1.23(1.06~1.42) | 0.005 | 1.20(0.99~1.45) | 0.058 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.005 | |||
| Q2组 | 0.95(0.53~1.69) | 0.864 | 0.90(0.50~1.59) | 0.708 | 0.92(0.51~1.65) | 0.774 |
| Q3组 | 2.15(1.34~3.55) | 0.002 | 1.90(1.18~3.15) | 0.010 | 1.85(1.11~3.15) | 0.020 |
| Q4组 | 2.58(1.63~4.20) | <0.001 | 2.00(1.24~3.30) | 0.005 | 1.87(1.08~3.31) | 0.028 |
Table 5 Multivariate Logistic regression analysis of NPAR on atrioventricular block in AMI patients
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.34(1.16~1.53) | <0.001 | 1.23(1.06~1.42) | 0.005 | 1.20(0.99~1.45) | 0.058 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.005 | |||
| Q2组 | 0.95(0.53~1.69) | 0.864 | 0.90(0.50~1.59) | 0.708 | 0.92(0.51~1.65) | 0.774 |
| Q3组 | 2.15(1.34~3.55) | 0.002 | 1.90(1.18~3.15) | 0.010 | 1.85(1.11~3.15) | 0.020 |
| Q4组 | 2.58(1.63~4.20) | <0.001 | 2.00(1.24~3.30) | 0.005 | 1.87(1.08~3.31) | 0.028 |
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.49(1.28~1.72) | <0.001 | 1.45(1.24~1.68) | <0.001 | 1.23(1.00~1.50) | 0.046 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.017 | |||
| Q2组 | 1.59(0.84~3.13) | 0.162 | 1.58(0.83~3.10) | 0.172 | 1.50(0.77~2.98) | 0.237 |
| Q3组 | 2.11(1.14~4.05) | 0.020 | 2.02(1.09~3.89) | 0.029 | 1.90(0.99~3.77) | 0.059 |
| Q4组 | 3.66(2.11~6.76) | <0.001 | 3.38(1.91~6.33) | <0.001 | 2.26(1.16~4.58) | 0.019 |
Table 6 Multivariate Logistic regression analysis of NPAR on new-onset stroke in AMI patients
| 变量 | 未校正模型 | 模型1 | 模型2 | |||
|---|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| NPAR | 1.49(1.28~1.72) | <0.001 | 1.45(1.24~1.68) | <0.001 | 1.23(1.00~1.50) | 0.046 |
| NPAR分组(以Q1组为参照) | <0.001 | <0.001 | 0.017 | |||
| Q2组 | 1.59(0.84~3.13) | 0.162 | 1.58(0.83~3.10) | 0.172 | 1.50(0.77~2.98) | 0.237 |
| Q3组 | 2.11(1.14~4.05) | 0.020 | 2.02(1.09~3.89) | 0.029 | 1.90(0.99~3.77) | 0.059 |
| Q4组 | 3.66(2.11~6.76) | <0.001 | 3.38(1.91~6.33) | <0.001 | 2.26(1.16~4.58) | 0.019 |
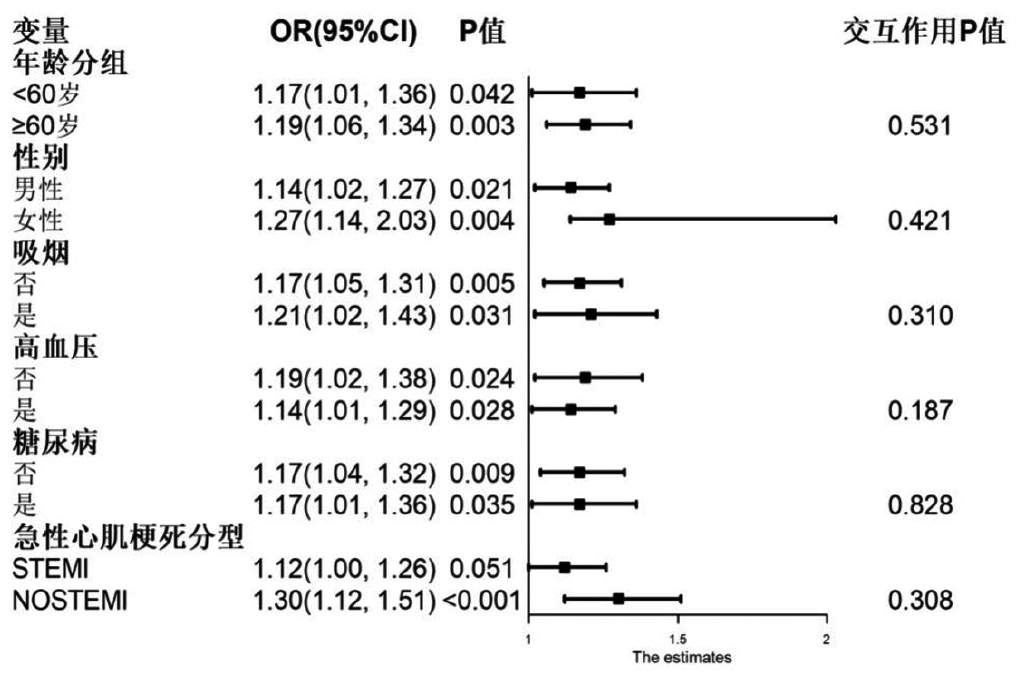
Figure 4 Stratified analysis and interaction analysis results of NPAR with in-hospital all-cause mortality risk
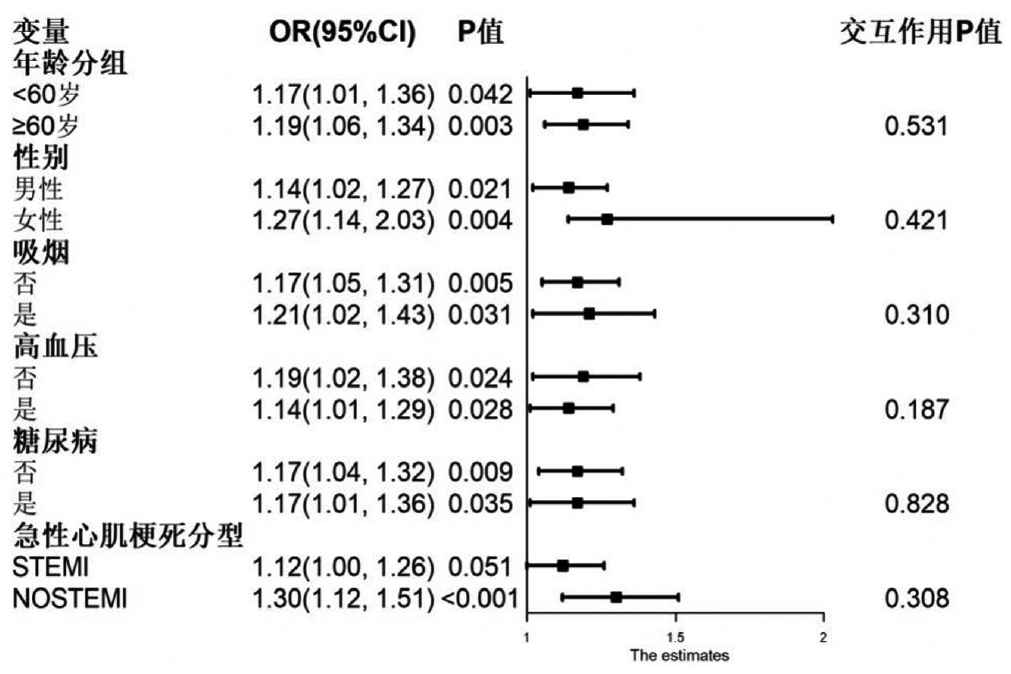
Figure 5 Stratified analysis and interaction analysis results of NPAR with in-hospital cardiogenic shock
| [1] |
2019 Diseases and Injuries Collaborators GBD. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-1222. DOI: 10.1016/S0140-6736(20)30925-9.
|
| [2] |
|
| [3] |
中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2022概要[J]. 中国循环杂志, 2023, 38(6): 583-612. DOI: 10.3969/j.issn.1000-3614.2023.06.001.
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
急性ST段抬高型心肌梗死诊断和治疗指南(2019)[J]. 中华心血管病杂志, 2019, 47(10): 766-783. DOI: 10.3760/cma.j.issn.0253?3758.2019.10.003.
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [1] | ZHEN Rui, GU Xufang, GAO Shengwei, ZHANG Bowen, REN Zhenjuan, YANG Ruixuan. Burden of Cardiovascular Diseases Attributable to Metabolic Risk Factors in China 1990—2021 and Projected Trends from 2022 to 2035 [J]. Chinese General Practice, 2026, 29(15): 2077-2083. |
| [2] | HU Jiaqi, LI Duan, FANG Hao, FAN Xingying, DU Wei, ZHOU Hanni. Study on Predictive Model of Non-genetic Risk Factors for Hyperuricemia in a Physical Examination Cohort [J]. Chinese General Practice, 2026, 29(10): 1324-1333. |
| [3] | WANG Lina, LEI Jingshu, LI Kuibao, WANG Ruiying, LI Xinmiao, WANG Fangfang, GUO Xiaorong, NIU Ruihao, ZHAO Wei, ZHOU Fangfang, ZHAO Jingjing, LEE CHONGYOU. Review on Inflammatory Response in Patients with Acute Myocardial Infarction [J]. Chinese General Practice, 2026, 29(06): 790-801. |
| [4] | LEI Yingying, ZHENG Siying, WANG Wenxin, JIANG Hong. Prevalence Trend and Prediction of Hypertensive Heart Disease in the World and China from 1990 to 2021 [J]. Chinese General Practice, 2026, 29(05): 641-648. |
| [5] | ZHANG Shu, CHENG Yu, WU Shouling, CHEN Shuohua, WU Yuntao. The Impact of Cumulative Plasma Atherogenic Index Exposure on Incident Cardiovascular Disease in Non-Diabetic Individuals: a Cohort Study [J]. Chinese General Practice, 2025, 28(36): 4558-4565. |
| [6] | CEN Kaiyuan, FATIMAH Ahmedy, CHEN Hong, SHAO Mingchen, MEXMOLLEN Marcus, MOHD Fadzli Shukor. Exercise-based Cardiac Rehabilitation in Acute Myocardial Infarction Management: Global Perspectives, Multimodal Interventions, and Personalized Strategies [J]. Chinese General Practice, 2025, 28(36): 4627-4639. |
| [7] | MI Lingyu, CHEN Lianxin, GAO Hengbo, WANG Bincheng. Predictive Value of Triglyceride-glucose Index for Prognosis in Patients with Pulmonary Embolism [J]. Chinese General Practice, 2025, 28(35): 4421-4429. |
| [8] | WANG Biyou, GAO Ying, YOU Junfang, LIU Li, ZHANG Qing, SU Haiyan. Canonical Correlation Analysis of Lipid Ratios and Inflammatory Markers in Individuals at Risk of Cardiovascular Disease [J]. Chinese General Practice, 2025, 28(33): 4132-4139. |
| [9] | SHANG Luxiang, ZHU Mingqi, ZHOU Xianhui, GAO Mei, TANG Baopeng, HOU Yinglong. Prevalence and Risk Factors of Atrial Fibrillation among Adults in China: a Meta-analysis [J]. Chinese General Practice, 2025, 28(33): 4192-4198. |
| [10] | LIU Mingbo, HE Xinye, YANG Xiaohong, WANG Zengwu. Interpretation of Report on Cardiovascular Health and Diseases in China 2024 [J]. Chinese General Practice, 2025, 28(32): 3989-4008. |
| [11] | ZHANG Ji, ZHOU Jie, LI Ling, WU Yanli, JI Wei, LIU Tao. Associations of Fasting Blood Glucose with All-cause Mortality and Specific-cause Mortality in a Prospective Cohort Study [J]. Chinese General Practice, 2025, 28(31): 3924-3931. |
| [12] | XU Baichuan, WANG Yan, ZHANG Peng, LI Yiting, LIU Feilai, XIE Yang. Research and Analysis of Screening Tools for Chronic Obstructive Pulmonary Disease Comorbidity Lung Cancer [J]. Chinese General Practice, 2025, 28(30): 3847-3852. |
| [13] | SU Qing, XU Yao, LI Yihang, WANG Liyan, CAI Yefeng, NI Xiaojia. Quality Evaluation of Methodology on the Changes in Traditional Chinese Medicine Syndromes of Stroke and Risk Population [J]. Chinese General Practice, 2025, 28(29): 3694-3702. |
| [14] | DENG Jie, QI Qi, WU Xinyu, HAN Quanle, LI Lei, JIANG Yue, YU Jing, WU Ruojie, WU Shouling, LI Kangbo. Cohort Study on the Association between the Atherogenic Index of Plasma and the Risk of Incident Heart Failure in a Physical Examination Population [J]. Chinese General Practice, 2025, 28(29): 3645-3652. |
| [15] | SHAO Xiaoying, SHAO Jie, ZHU Yan, SHAO Jinling, SHANG Ling, WU Zhenlian, ZHAO Yu, ZHANG Jiacai. Analysis of the Current Status of Iron Deficiency and Factors Affecting Iron Deficiency Anemia among Children Aged 6-36 Months in Guizhou Province [J]. Chinese General Practice, 2025, 28(27): 3368-3374. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||