
Chinese General Practice ›› 2023, Vol. 26 ›› Issue (16): 2047-2054.DOI: 10.12114/j.issn.1007-9572.2022.0388
• Original Research·Focus on Research Tools • Previous Articles
Received:2022-05-31
Revised:2023-03-11
Published:2023-06-05
Online:2023-03-23
Contact:
NI Ziling
通讯作者:
倪紫菱
作者简介:基金资助:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2022.0388
| 项目 | 人数 | 构成比(%) |
|---|---|---|
| 性别 | ||
| 男 | 70 | 22.7 |
| 女 | 239 | 77.3 |
| 年龄(岁) | ||
| 20~30 | 63 | 20.4 |
| 31~40 | 126 | 40.8 |
| 41~50 | 91 | 29.4 |
| ≥51 | 29 | 9.4 |
| 工作岗位a | ||
| 家庭医生团队长 | 74 | 23.9 |
| 家庭医生助理 | 18 | 5.8 |
| 护士 | 109 | 35.3 |
| 医师 | 69 | 22.3 |
| 其他 | 39 | 12.6 |
| 工作年限(年) | ||
| 1~5 | 49 | 15.9 |
| 6~10 | 69 | 22.3 |
| 11~15 | 85 | 27.5 |
| 16~20 | 23 | 7.4 |
| ≥21 | 83 | 26.9 |
| 在本单位工作年限(年) | ||
| 0~5 | 117 | 37.9 |
| 6~10 | 70 | 22.7 |
| 11~15 | 48 | 15.5 |
| 16~20 | 19 | 6.1 |
| ≥21 | 55 | 17.8 |
| 以家庭医生团队成员身份提供家庭医生服务的年限(年) | ||
| 1~5 | 183 | 59.2 |
| 6~10 | 95 | 30.7 |
| 11~15 | 17 | 5.5 |
| 16~20 | 8 | 2.6 |
| ≥21 | 6 | 1.9 |
| 技术职称 | ||
| 无 | 30 | 9.7 |
| 初级 | 127 | 41.1 |
| 中级 | 133 | 43.0 |
| 副高级 | 18 | 5.8 |
| 正高级 | 1 | 0.3 |
Table 1 General information for the respondents
| 项目 | 人数 | 构成比(%) |
|---|---|---|
| 性别 | ||
| 男 | 70 | 22.7 |
| 女 | 239 | 77.3 |
| 年龄(岁) | ||
| 20~30 | 63 | 20.4 |
| 31~40 | 126 | 40.8 |
| 41~50 | 91 | 29.4 |
| ≥51 | 29 | 9.4 |
| 工作岗位a | ||
| 家庭医生团队长 | 74 | 23.9 |
| 家庭医生助理 | 18 | 5.8 |
| 护士 | 109 | 35.3 |
| 医师 | 69 | 22.3 |
| 其他 | 39 | 12.6 |
| 工作年限(年) | ||
| 1~5 | 49 | 15.9 |
| 6~10 | 69 | 22.3 |
| 11~15 | 85 | 27.5 |
| 16~20 | 23 | 7.4 |
| ≥21 | 83 | 26.9 |
| 在本单位工作年限(年) | ||
| 0~5 | 117 | 37.9 |
| 6~10 | 70 | 22.7 |
| 11~15 | 48 | 15.5 |
| 16~20 | 19 | 6.1 |
| ≥21 | 55 | 17.8 |
| 以家庭医生团队成员身份提供家庭医生服务的年限(年) | ||
| 1~5 | 183 | 59.2 |
| 6~10 | 95 | 30.7 |
| 11~15 | 17 | 5.5 |
| 16~20 | 8 | 2.6 |
| ≥21 | 6 | 1.9 |
| 技术职称 | ||
| 无 | 30 | 9.7 |
| 初级 | 127 | 41.1 |
| 中级 | 133 | 43.0 |
| 副高级 | 18 | 5.8 |
| 正高级 | 1 | 0.3 |
| 条目 | 得分( | 条目鉴别度 | 条目得分与总分相关性 | ||
|---|---|---|---|---|---|
| CR值 | P值 | r值 | P值 | ||
| 1.我所在的团队中,团队成员稳定,不会频繁变动 | 2.13±1.13 | -7.545 | <0.001 | 0.426 | <0.001 |
| 2.我所在的团队中,团队成员拥有不同的学科背景,可以为我们的工作提供多样的视角和经验 | 2.09±1.04 | -11.691 | <0.001 | 0.648 | <0.001 |
| 3.我所在的团队有明确的团队成员行为准则 | 1.86±0.97 | -13.914 | <0.001 | 0.775 | <0.001 |
| 4.机构鼓励团队成员间开展良好合作 | 1.69±0.95 | -12.624 | <0.001 | 0.797 | <0.001 |
| 5.我们团队有明确且合适的目标 | 1.76±0.96 | -15.422 | <0.001 | 0.832 | <0.001 |
| 6.团队成员会主动向团队内其他成员寻求合作 | 1.74±0.92 | -14.100 | <0.001 | 0.820 | <0.001 |
| 7.团队成员对自己和他人的分工有清楚的认知 | 1.72±0.98 | -12.921 | <0.001 | 0.808 | <0.001 |
| 8.团队成员会鼓励签约对象积极参与他们自己的诊疗方案的制定 | 1.77±0.99 | -13.324 | <0.001 | 0.824 | <0.001 |
| 9.团队成员会帮助签约对象清楚地了解他们自己的诊疗方案 | 1.81±0.99 | -13.540 | <0.001 | 0.814 | <0.001 |
| 10.团队成员在提供服务的过程中非常重视签约对象的需求与偏好 | 1.86±0.98 | -13.123 | <0.001 | 0.789 | <0.001 |
| 11.团队内有明确的岗位责任制度 | 1.68±0.90 | -14.156 | <0.001 | 0.848 | <0.001 |
| 12.团队成员会及时共享签约对象的治疗目标并达成一致 | 1.74±0.92 | -14.243 | <0.001 | 0.868 | <0.001 |
| 13.团队成员会及时更新签约对象的现况或诊疗方案 | 1.79±0.96 | -14.625 | <0.001 | 0.835 | <0.001 |
| 14.团队成员会将签约对象的健康档案作为成员间沟通的工具 | 1.85±0.95 | -13.189 | <0.001 | 0.820 | <0.001 |
| 15.团队内会通过团队会议有效解决签约对象的问题 | 1.87±0.98 | -14.881 | <0.001 | 0.835 | <0.001 |
| 16.团队会议氛围轻松,团队成员可以畅所欲言 | 1.79±1.03 | -14.595 | <0.001 | 0.837 | <0.001 |
| 17.当团队成员对决策有异议时,团队成员会在做出最终决定前考虑每一个方案 | 1.87±1.07 | -16.680 | <0.001 | 0.823 | <0.001 |
| 18.团队内有完善的团队冲突管理方式 | 2.05±1.10 | -17.876 | <0.001 | 0.786 | <0.001 |
| 19.团队成员间互相尊重彼此的角色和专业知识 | 1.76±0.95 | -16.320 | <0.001 | 0.868 | <0.001 |
| 20.团队成员互相依赖于对方的专业知识与技能 | 1.82±1.00 | -15.196 | <0.001 | 0.781 | <0.001 |
| 21.团队成员在签约对象相关的工作上各司其职,协调有度 | 1.76±0.93 | -16.339 | <0.001 | 0.859 | <0.001 |
| 22.团队成员互相信任彼此所做的工作 | 1.69±0.91 | -14.697 | <0.001 | 0.851 | <0.001 |
| 23.我会定期与团队内其他成员沟通 | 1.69±0.92 | -13.526 | <0.001 | 0.802 | <0.001 |
| 24.团队成员会根据我提供的信息开展行动 | 1.70±0.92 | -15.063 | <0.001 | 0.819 | <0.001 |
| 25.团队成员间的相互合作提升了我们团队的服务效率 | 1.65±0.87 | -14.043 | <0.001 | 0.839 | <0.001 |
| 26.团队成员间的相互合作提升了我们团队的服务质量 | 1.65±0.86 | -13.841 | <0.001 | 0.836 | <0.001 |
| 27.团队成员对自己的工作充满热情和兴趣 | 1.79±0.93 | -14.557 | <0.001 | 0.805 | <0.001 |
| 28.我觉得我是团队中不可或缺的一员 | 1.81±0.95 | -8.816 | <0.001 | 0.627 | <0.001 |
| 29.我与我的团队成员精诚合作 | 1.57±0.84 | -13.416 | <0.001 | 0.798 | <0.001 |
Table 2 Item analysis of the Chinese version of PCTDS
| 条目 | 得分( | 条目鉴别度 | 条目得分与总分相关性 | ||
|---|---|---|---|---|---|
| CR值 | P值 | r值 | P值 | ||
| 1.我所在的团队中,团队成员稳定,不会频繁变动 | 2.13±1.13 | -7.545 | <0.001 | 0.426 | <0.001 |
| 2.我所在的团队中,团队成员拥有不同的学科背景,可以为我们的工作提供多样的视角和经验 | 2.09±1.04 | -11.691 | <0.001 | 0.648 | <0.001 |
| 3.我所在的团队有明确的团队成员行为准则 | 1.86±0.97 | -13.914 | <0.001 | 0.775 | <0.001 |
| 4.机构鼓励团队成员间开展良好合作 | 1.69±0.95 | -12.624 | <0.001 | 0.797 | <0.001 |
| 5.我们团队有明确且合适的目标 | 1.76±0.96 | -15.422 | <0.001 | 0.832 | <0.001 |
| 6.团队成员会主动向团队内其他成员寻求合作 | 1.74±0.92 | -14.100 | <0.001 | 0.820 | <0.001 |
| 7.团队成员对自己和他人的分工有清楚的认知 | 1.72±0.98 | -12.921 | <0.001 | 0.808 | <0.001 |
| 8.团队成员会鼓励签约对象积极参与他们自己的诊疗方案的制定 | 1.77±0.99 | -13.324 | <0.001 | 0.824 | <0.001 |
| 9.团队成员会帮助签约对象清楚地了解他们自己的诊疗方案 | 1.81±0.99 | -13.540 | <0.001 | 0.814 | <0.001 |
| 10.团队成员在提供服务的过程中非常重视签约对象的需求与偏好 | 1.86±0.98 | -13.123 | <0.001 | 0.789 | <0.001 |
| 11.团队内有明确的岗位责任制度 | 1.68±0.90 | -14.156 | <0.001 | 0.848 | <0.001 |
| 12.团队成员会及时共享签约对象的治疗目标并达成一致 | 1.74±0.92 | -14.243 | <0.001 | 0.868 | <0.001 |
| 13.团队成员会及时更新签约对象的现况或诊疗方案 | 1.79±0.96 | -14.625 | <0.001 | 0.835 | <0.001 |
| 14.团队成员会将签约对象的健康档案作为成员间沟通的工具 | 1.85±0.95 | -13.189 | <0.001 | 0.820 | <0.001 |
| 15.团队内会通过团队会议有效解决签约对象的问题 | 1.87±0.98 | -14.881 | <0.001 | 0.835 | <0.001 |
| 16.团队会议氛围轻松,团队成员可以畅所欲言 | 1.79±1.03 | -14.595 | <0.001 | 0.837 | <0.001 |
| 17.当团队成员对决策有异议时,团队成员会在做出最终决定前考虑每一个方案 | 1.87±1.07 | -16.680 | <0.001 | 0.823 | <0.001 |
| 18.团队内有完善的团队冲突管理方式 | 2.05±1.10 | -17.876 | <0.001 | 0.786 | <0.001 |
| 19.团队成员间互相尊重彼此的角色和专业知识 | 1.76±0.95 | -16.320 | <0.001 | 0.868 | <0.001 |
| 20.团队成员互相依赖于对方的专业知识与技能 | 1.82±1.00 | -15.196 | <0.001 | 0.781 | <0.001 |
| 21.团队成员在签约对象相关的工作上各司其职,协调有度 | 1.76±0.93 | -16.339 | <0.001 | 0.859 | <0.001 |
| 22.团队成员互相信任彼此所做的工作 | 1.69±0.91 | -14.697 | <0.001 | 0.851 | <0.001 |
| 23.我会定期与团队内其他成员沟通 | 1.69±0.92 | -13.526 | <0.001 | 0.802 | <0.001 |
| 24.团队成员会根据我提供的信息开展行动 | 1.70±0.92 | -15.063 | <0.001 | 0.819 | <0.001 |
| 25.团队成员间的相互合作提升了我们团队的服务效率 | 1.65±0.87 | -14.043 | <0.001 | 0.839 | <0.001 |
| 26.团队成员间的相互合作提升了我们团队的服务质量 | 1.65±0.86 | -13.841 | <0.001 | 0.836 | <0.001 |
| 27.团队成员对自己的工作充满热情和兴趣 | 1.79±0.93 | -14.557 | <0.001 | 0.805 | <0.001 |
| 28.我觉得我是团队中不可或缺的一员 | 1.81±0.95 | -8.816 | <0.001 | 0.627 | <0.001 |
| 29.我与我的团队成员精诚合作 | 1.57±0.84 | -13.416 | <0.001 | 0.798 | <0.001 |
| 条目 | 公因子1 | 公因子2 | 公因子3 | 公因子4 |
|---|---|---|---|---|
| 1 | 0.802 | — | — | — |
| 2 | 0.775 | — | — | — |
| 3 | 0.727 | — | — | — |
| 4 | 0.579 | 0.507 | — | — |
| 5 | — | 0.669 | — | — |
| 6 | — | 0.737 | — | — |
| 7 | — | 0.749 | — | — |
| 8 | — | 0.753 | — | — |
| 9 | — | 0.738 | — | — |
| 10 | — | 0.687 | — | — |
| 11 | — | — | — | — |
| 12 | — | — | 0.561 | — |
| 13 | — | — | 0.670 | — |
| 14 | — | — | 0.692 | — |
| 15 | — | — | 0.679 | — |
| 16 | — | — | 0.664 | — |
| 17 | — | — | 0.662 | — |
| 18 | — | — | 0.690 | — |
| 19 | — | — | 0.549 | 0.606 |
| 20 | — | — | 0.651 | — |
| 21 | — | — | 0.592 | 0.530 |
| 22 | — | — | — | 0.741 |
| 23 | — | — | — | 0.684 |
| 24 | — | — | — | 0.756 |
| 25 | — | — | — | 0.770 |
| 26 | — | — | — | 0.761 |
| 27 | — | — | — | 0.658 |
| 28 | — | — | — | 0.671 |
| 29 | — | — | — | 0.767 |
Table 3 The factor loading values for every item in the Chinese version of PCTDS
| 条目 | 公因子1 | 公因子2 | 公因子3 | 公因子4 |
|---|---|---|---|---|
| 1 | 0.802 | — | — | — |
| 2 | 0.775 | — | — | — |
| 3 | 0.727 | — | — | — |
| 4 | 0.579 | 0.507 | — | — |
| 5 | — | 0.669 | — | — |
| 6 | — | 0.737 | — | — |
| 7 | — | 0.749 | — | — |
| 8 | — | 0.753 | — | — |
| 9 | — | 0.738 | — | — |
| 10 | — | 0.687 | — | — |
| 11 | — | — | — | — |
| 12 | — | — | 0.561 | — |
| 13 | — | — | 0.670 | — |
| 14 | — | — | 0.692 | — |
| 15 | — | — | 0.679 | — |
| 16 | — | — | 0.664 | — |
| 17 | — | — | 0.662 | — |
| 18 | — | — | 0.690 | — |
| 19 | — | — | 0.549 | 0.606 |
| 20 | — | — | 0.651 | — |
| 21 | — | — | 0.592 | 0.530 |
| 22 | — | — | — | 0.741 |
| 23 | — | — | — | 0.684 |
| 24 | — | — | — | 0.756 |
| 25 | — | — | — | 0.770 |
| 26 | — | — | — | 0.761 |
| 27 | — | — | — | 0.658 |
| 28 | — | — | — | 0.671 |
| 29 | — | — | — | 0.767 |
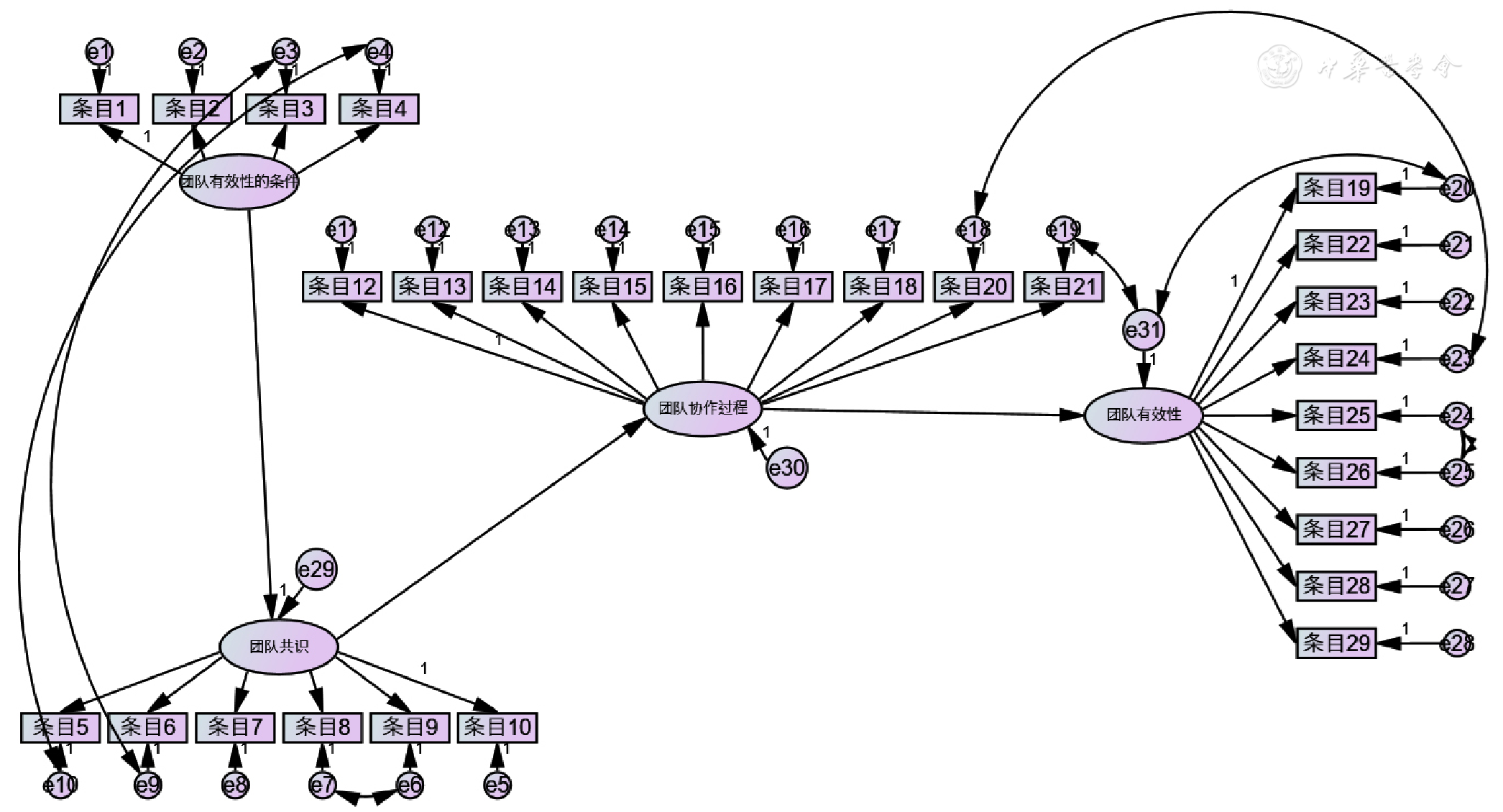
Figure 1 Estimated parameters of the model of confirmatory factor analysis of Chinese version of PCTDS
| 拟合指标 | 推荐值 | 模型1 | 模型2 |
|---|---|---|---|
| χ2值 | 越小越好 | 994.355 | 786.538 |
| χ2/df | <3.000 | 2.866 | 2.313 |
| RMSEA | <0.080 | 0.108 | 0.091 |
| GFI | >0.900 | 0.694 | 0.748 |
| AGFI | >0.900 | 0.642 | 0.699 |
| NFI | >0.900 | 0.830 | 0.866 |
| IFI | >0.900 | 0.883 | 0.919 |
| CFI | >0.900 | 0.882 | 0.919 |
Table 4 The fit indices and recommended values of modified Chinese version of PCTDS
| 拟合指标 | 推荐值 | 模型1 | 模型2 |
|---|---|---|---|
| χ2值 | 越小越好 | 994.355 | 786.538 |
| χ2/df | <3.000 | 2.866 | 2.313 |
| RMSEA | <0.080 | 0.108 | 0.091 |
| GFI | >0.900 | 0.694 | 0.748 |
| AGFI | >0.900 | 0.642 | 0.699 |
| NFI | >0.900 | 0.830 | 0.866 |
| IFI | >0.900 | 0.883 | 0.919 |
| CFI | >0.900 | 0.882 | 0.919 |
| [1] |
曲振翔. 推行家庭医生签约服务工作问题研究[D]. 郑州:郑州大学,2019.
|
| [2] | |
| [3] | |
| [4] |
王艺园,孙艳春,王伟,等. 基于供方视角的家庭医生团队签约服务工作感知及其相关因素研究[J]. 中国全科医学,2021,24(10):1218-1223,1230. DOI:10.12114/j.issn.1007-9572.2021.00.123.
|
| [5] |
马文翰,史大桢,赵亚利. 国内外家庭医生签约服务团队评估指标研究进展[J]. 中国全科医学,2022,25(7):791-796. DOI:10.12114/j.issn.1007-9572.2021.00.192.
|
| [6] |
国务院医改办,国家卫生计生委,国家发展改革委,等. 关于印发推进家庭医生签约服务指导意见的通知[A/OL]. (2016-06-06)[2022-04-11].
|
| [7] |
邓诗姣,刘心怡,陈文,等. 家庭医生签约服务工作现状与满意度分析[J]. 卫生经济研究,2022,39(2):78-80,84. DOI:10.14055/j.cnki.33-1056/f.2022.02.045.
|
| [8] |
王海霞. 团队互动过程对团队效能的影响研究[D]. 天津:天津财经大学,2008.
|
| [9] |
|
| [10] |
|
| [11] |
李康源,崔慧霞,孟迪,等. 护士人性化护理能力量表汉化及信效度检验[J]. 护理学杂志,2020,35(23):55-58. DOI:10.3870/j.issn.1001-4152.2020.23.055.
|
| [12] |
吴明隆. 问卷统计分析实务:SPSS操作与应用[M].重庆:重庆大学出版社,2010.
|
| [13] |
窦雄,郑传芬,武书兴,等. 我国家庭医生签约服务现状问题及对策研究进展[J]. 现代医药卫生,2021,37(2):229-232.
|
| [14] |
李兴春,李华. 我国家庭医生签约服务现状及存在问题研究进展[J]. 中国社区医师,2018,34(22):11-13,15.
|
| [15] |
蔡利强,盛清,龚思浩. 运用团队效能模型分析家庭医生签约服务团队存在问题及对策研究[J]. 中国初级卫生保健,2020,34(2):23-26.
|
| [16] |
|
| [17] |
|
| [18] |
|
| [1] | WANG Jiannan, SUN Jinming. The Chinese Version of Inventory of Motivations for Hospice Palliative Care Volunteerism (IMHPCV) : Reliability and Validity Assessment [J]. Chinese General Practice, 2023, 26(36): 4595-4601. |
| [2] | WANG Shiyue, DONG Chen, CHANG Chudi, NAN Yuemin. Opportunities and Challenges of Surveillance for Liver Cancer in Primary Care Institutions in China [J]. Chinese General Practice, 2023, 26(36): 4498-4504. |
| [3] | LUO Na, RUAN Yanqin, LEI Pingguang, WAN Chonghua, WAN Keyan, SONG Ying, CHEN Ying. Analysis of the Measurement Characteristics of Inflammatory Bowel Disease Patient-reported Outcomes Measurement Scale [J]. Chinese General Practice, 2023, 26(36): 4602-4607. |
| [4] | LU Lixia, WANG Rongqi. Advances in Liver Cancer Screening and Health Surveillance Management in Primary Care Institutions [J]. Chinese General Practice, 2023, 26(36): 4505-4509. |
| [5] | HAO Aihua, ZENG Weilin, LI Guanhai, XIA Yinghua, CHEN Liang. Current Situation of the Construction of Family Doctor Team: an Investigation Based on the Perspective of General Practitioners [J]. Chinese General Practice, 2023, 26(34): 4261-4268. |
| [6] | HUANG Jinling, ZENG Zhirong. The Logic and Trend of Urban Community Health Service Policies in China [J]. Chinese General Practice, 2023, 26(34): 4239-4245. |
| [7] | LIAN Lu, CHEN Jiaying, WANG Xuanxuan, LI Yahui, ZHU Ya. Current Situation and Countermeasure of Medical Service Capacity of Primary Care Physicians in China [J]. Chinese General Practice, 2023, 26(34): 4246-4253. |
| [8] | YANG Hui, HU Ruwei, LIU Ruqing, LU Junfeng, WU Jinglan. Relationship between Community Health Service Experience and Glycemic Control Outcomes in Patients with Diabetes Mellitus [J]. Chinese General Practice, 2023, 26(34): 4290-4295. |
| [9] | XU Jian, DAI Fangfang, PAN Wenlei, HUANG Qian, LU Ping, WANG Jianfeng, JIA Huan, YANG Yuqi, HUANG Jiaoling. Visual Analysis of Hotspots and Cutting-edge Trends of Community TCM Service Research in China in the Context of Healthy China [J]. Chinese General Practice, 2023, 26(34): 4343-4350. |
| [10] | LI Dianjiang, PAN Enchun, SUN Zhongming, WEN Jinbo, WANG Miaomiao, WU Ming, SHEN Chong. The Current Status and Influencing Factors of Clinical Inertia in Type 2 Diabetes Patients in Community [J]. Chinese General Practice, 2023, 26(34): 4296-4301. |
| [11] | QIN Fengyin, ZHANG Qishan, LAI Jinjia, HUANG Yimin, HAN Guoyin, SUN Xinglan, WANG Fen, TAN Yibing. Current Status and Influencing Factors of the Intention to Screen for High-risk Stroke among Community Residents in Guangdong [J]. Chinese General Practice, 2023, 26(34): 4283-4289. |
| [12] | YAO Yuzhong, MA Xiaojun, SONG Huan, ZHONG Yu. The Management Effect of Diabetes "1358 model" on Community Diabetes Patients Based on "Precision Management Combining General Care and Specialty Care" [J]. Chinese General Practice, 2023, 26(34): 4308-4314. |
| [13] | LI Qianqian, CHEN Xunrui, ZHANG Wenying, YUAN Haihua, ZHANG Yanjie, JIANG Bin, LIU Feng. Demand and Influencing Factors for Community Health Services during Chemotherapy of Patients with Advanced Cancer [J]. Chinese General Practice, 2023, 26(33): 4173-4180. |
| [14] | YIN Zhaoxia, MAO Lidong, ZHANG Baoshuang, HUANG Yin, FENG Yang, WANG Yunfei. Spectrum of Outpatient Illnesses in Children Contracting Family Doctor Services in Shenzhen's Community Settings and Related Implications for Standardized Residency Training of General Practitioners [J]. Chinese General Practice, 2023, 26(33): 4218-4224. |
| [15] | YU Dehua. Scientific Research Conception Guided by General Practice Thinking [J]. Chinese General Practice, 2023, 26(31): 3872-3876. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||