
Chinese General Practice ›› 2025, Vol. 28 ›› Issue (05): 587-593.DOI: 10.12114/j.issn.1007-9572.2023.0924
• Original Research • Previous Articles Next Articles
Received:2024-04-10
Revised:2024-07-09
Published:2025-02-15
Online:2024-11-25
Contact:
MA Qing
通讯作者:
马清
作者简介:作者贡献:
石小天提出主要研究目标,负责研究的构思与设计,研究的实施,撰写论文;石小天、杨一帆、李旭、窦国泽进行数据的收集与整理,统计学处理,图、表的绘制与展示;王珊、杨华昱进行论文的修订;马清负责文章的质量控制与审查,对文章整体负责,监督管理。
基金资助:CLC Number:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2023.0924
| 组别 | 例数 | 性别[例(%)] | 年龄[M(P25,P75),岁] | BMI [M(P25,P75),kg/m2] | 文化程度[例(%)] | 多重用药[例(%)] | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 高中以下 | 高中 | 大学及以上 | 是 | 否 | ||||
| 无衰弱组 | 341 | 259(75.95) | 82(24.05) | 71.0(65.0,80.0) | 24.37(22.42,26.21) | 7(2.05) | 23(6.74) | 311(91.20) | 85(24.93) | 256(75.07) |
| 衰弱/衰弱前期组 | 213 | 154(72.30) | 59(25.70) | 79.0(68.0,86.0) | 23.91(21.92,26.10) | 12(5.63) | 14(6.57) | 187(87.79) | 103(48.36) | 110(51.64) |
| 检验统计量值 | 0.920a | -6.166 | -1.398 | 5.078a | 32.104a | |||||
| P值 | 0.337 | <0.001 | 0.162 | 0.079 | <0.001 | |||||
| 组别 | 独居[例(%)] | 吸烟[例(%)] | 饮酒[例(%)] | MNA-SF评分[M(P25,P75),分] | ACCI [M(P25,P75),分] | 糖化血红蛋白[M(P25,P75),%] | ||||
| 是 | 否 | 是 | 否 | 是 | 否 | |||||
| 无衰弱组 | 28(8.21) | 313(91.79) | 46(13.49) | 295(86.51) | 109(31.96) | 232(68.04) | 14.00(13.00,14.00) | 3.00(2.00,4.00) | 5.97(5.67,6.42) | |
| 衰弱/衰弱前期组 | 19(8.92) | 194(91.08) | 28(13.15) | 185(86.85) | 54(25.35) | 159(74.65) | 13.00(12.00,14.00) | 4.00(3.00,5.00) | 5.89(5.60,6.24) | |
| 检验统计量值 | 0.085a | 0.013a | 2.761a | -4.920 | -6.569 | -1.768 | ||||
| P值 | 0.771 | 0.908 | 0.097 | <0.001 | <.001 | 0.077 | ||||
| 组别 | 白蛋白(g/L) | 白细胞计数[M(P25,P75),×109/L] | 中性粒细胞绝对值[M(P25,P75),×109/L] | 淋巴细胞绝对值[M(P25,P75),×109/L] | 单核细胞绝对值[M(P25,P75),×109/L] | 红细胞[M(P25,P75),×1012/L] | 血红蛋白[M(P25,P75),g/L] | |||
| 无衰弱组 | 44.07±2.57 | 6.14(5.28,7.25) | 3.47(2.81,4.30) | 2.21(1.71,2.65) | 0.29(0.23,0.38) | 4.73(4.46,4.96) | 148.00(140.00,155.00) | |||
| 衰弱/衰弱前期组 | 42.96±2.91 | 6.21(5.23,7.38) | 3.52(2.87,4.39) | 2.10(1.62,2.51) | 0.29(0.23,0.35) | 4.61(4.22,4.83) | 142.00(132.00,151.00) | |||
| 检验统计量值 | 4.169b | -0.115 | -0.817 | -2.497 | -0.732 | -3.786 | -4.856 | |||
| P值 | <0.001 | 0.909 | 0.414 | 0.013 | 0.464 | <0.001 | <0.001 | |||
| 组别 | 红细胞体积分布宽度[M(P25,P75),fL] | 血小板计数[M(P25,P75),×109/L] | 血小板体积分布宽度[M(P25,P75),%] | 总胆固醇[M(P25,P75),μmol/L] | 三酰甘油[M(P25,P75),μmol/L] | 高密度脂蛋白[M(P25,P75),μmol/L] | ||||
| 无衰弱组 | 43.60(41.70,45.20) | 211.00(183.00,244.00) | 11.50(10.70,12.50) | 4.80(4.20,5.57) | 1.26(0.98,1.71) | 1.19(1.03,1.37) | ||||
| 衰弱/衰弱前期组 | 44.30(42.60,45.90) | 206.00(172.00,244.00) | 11.50(10.40,12.50) | 4.65(3.85,5.45) | 1.14(0.85,1.68) | 1.23(1.02,1.48) | ||||
| 检验统计量值 | -2.702 | -1.541 | -0.868 | -2.560 | -2.896 | -1.030 | ||||
| P值 | 0.007 | 0.123 | 0.386 | 0.010 | 0.004 | 0.303 | ||||
| 组别 | 低密度脂蛋白[M(P25,P75),μmol/L] | NLR [M(P25,P75)] | dNLR [M(P25,P75)] | HRR [M(P25,P75)] | MLR [M(P25,P75)] | PLR [M(P25,P75)] | PRP [M(P25,P75)] | |||
| 无衰弱组 | 2.93(2.51,3.47) | 1.54(1.19,2.06) | 1.74(1.39,2.35) | 3.41(3.16,3.61) | 0.14(0.10,0.18) | 96.70(77.25,118.22) | 0.21(0.18,0.24) | |||
| 衰弱/衰弱前期组 | 2.67(2.19,3.26) | 1.73(1.30,2.31) | 2.00(1.53,2.63) | 3.23(2.97,3.48) | 0.14(0.11,0.19) | 96.40(79.61,124.30) | 0.21(0.18,0.27) | |||
| 检验统计量值 | -4.220 | -2.681 | -2.955 | -4.942 | -1.340 | -0.905 | -2.037 | |||
| P值 | <0.001 | 0.007 | 0.003 | <0.001 | 0.180 | 0.365 | 0.042 | |||
Table 1 Clinical features in the elderly of non-frail group versus frail/pre-frail group
| 组别 | 例数 | 性别[例(%)] | 年龄[M(P25,P75),岁] | BMI [M(P25,P75),kg/m2] | 文化程度[例(%)] | 多重用药[例(%)] | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 高中以下 | 高中 | 大学及以上 | 是 | 否 | ||||
| 无衰弱组 | 341 | 259(75.95) | 82(24.05) | 71.0(65.0,80.0) | 24.37(22.42,26.21) | 7(2.05) | 23(6.74) | 311(91.20) | 85(24.93) | 256(75.07) |
| 衰弱/衰弱前期组 | 213 | 154(72.30) | 59(25.70) | 79.0(68.0,86.0) | 23.91(21.92,26.10) | 12(5.63) | 14(6.57) | 187(87.79) | 103(48.36) | 110(51.64) |
| 检验统计量值 | 0.920a | -6.166 | -1.398 | 5.078a | 32.104a | |||||
| P值 | 0.337 | <0.001 | 0.162 | 0.079 | <0.001 | |||||
| 组别 | 独居[例(%)] | 吸烟[例(%)] | 饮酒[例(%)] | MNA-SF评分[M(P25,P75),分] | ACCI [M(P25,P75),分] | 糖化血红蛋白[M(P25,P75),%] | ||||
| 是 | 否 | 是 | 否 | 是 | 否 | |||||
| 无衰弱组 | 28(8.21) | 313(91.79) | 46(13.49) | 295(86.51) | 109(31.96) | 232(68.04) | 14.00(13.00,14.00) | 3.00(2.00,4.00) | 5.97(5.67,6.42) | |
| 衰弱/衰弱前期组 | 19(8.92) | 194(91.08) | 28(13.15) | 185(86.85) | 54(25.35) | 159(74.65) | 13.00(12.00,14.00) | 4.00(3.00,5.00) | 5.89(5.60,6.24) | |
| 检验统计量值 | 0.085a | 0.013a | 2.761a | -4.920 | -6.569 | -1.768 | ||||
| P值 | 0.771 | 0.908 | 0.097 | <0.001 | <.001 | 0.077 | ||||
| 组别 | 白蛋白(g/L) | 白细胞计数[M(P25,P75),×109/L] | 中性粒细胞绝对值[M(P25,P75),×109/L] | 淋巴细胞绝对值[M(P25,P75),×109/L] | 单核细胞绝对值[M(P25,P75),×109/L] | 红细胞[M(P25,P75),×1012/L] | 血红蛋白[M(P25,P75),g/L] | |||
| 无衰弱组 | 44.07±2.57 | 6.14(5.28,7.25) | 3.47(2.81,4.30) | 2.21(1.71,2.65) | 0.29(0.23,0.38) | 4.73(4.46,4.96) | 148.00(140.00,155.00) | |||
| 衰弱/衰弱前期组 | 42.96±2.91 | 6.21(5.23,7.38) | 3.52(2.87,4.39) | 2.10(1.62,2.51) | 0.29(0.23,0.35) | 4.61(4.22,4.83) | 142.00(132.00,151.00) | |||
| 检验统计量值 | 4.169b | -0.115 | -0.817 | -2.497 | -0.732 | -3.786 | -4.856 | |||
| P值 | <0.001 | 0.909 | 0.414 | 0.013 | 0.464 | <0.001 | <0.001 | |||
| 组别 | 红细胞体积分布宽度[M(P25,P75),fL] | 血小板计数[M(P25,P75),×109/L] | 血小板体积分布宽度[M(P25,P75),%] | 总胆固醇[M(P25,P75),μmol/L] | 三酰甘油[M(P25,P75),μmol/L] | 高密度脂蛋白[M(P25,P75),μmol/L] | ||||
| 无衰弱组 | 43.60(41.70,45.20) | 211.00(183.00,244.00) | 11.50(10.70,12.50) | 4.80(4.20,5.57) | 1.26(0.98,1.71) | 1.19(1.03,1.37) | ||||
| 衰弱/衰弱前期组 | 44.30(42.60,45.90) | 206.00(172.00,244.00) | 11.50(10.40,12.50) | 4.65(3.85,5.45) | 1.14(0.85,1.68) | 1.23(1.02,1.48) | ||||
| 检验统计量值 | -2.702 | -1.541 | -0.868 | -2.560 | -2.896 | -1.030 | ||||
| P值 | 0.007 | 0.123 | 0.386 | 0.010 | 0.004 | 0.303 | ||||
| 组别 | 低密度脂蛋白[M(P25,P75),μmol/L] | NLR [M(P25,P75)] | dNLR [M(P25,P75)] | HRR [M(P25,P75)] | MLR [M(P25,P75)] | PLR [M(P25,P75)] | PRP [M(P25,P75)] | |||
| 无衰弱组 | 2.93(2.51,3.47) | 1.54(1.19,2.06) | 1.74(1.39,2.35) | 3.41(3.16,3.61) | 0.14(0.10,0.18) | 96.70(77.25,118.22) | 0.21(0.18,0.24) | |||
| 衰弱/衰弱前期组 | 2.67(2.19,3.26) | 1.73(1.30,2.31) | 2.00(1.53,2.63) | 3.23(2.97,3.48) | 0.14(0.11,0.19) | 96.40(79.61,124.30) | 0.21(0.18,0.27) | |||
| 检验统计量值 | -4.220 | -2.681 | -2.955 | -4.942 | -1.340 | -0.905 | -2.037 | |||
| P值 | <0.001 | 0.007 | 0.003 | <0.001 | 0.180 | 0.365 | 0.042 | |||
| 因素 | β | SE | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| MNA-SF评分 | -0.34 | 0.08 | -4.36 | <0.001 | 0.71(0.61~0.83) |
| ACCI | 0.35 | 0.08 | 4.33 | <0.001 | 1.42(1.21~1.66) |
| HRR | -0.81 | 0.34 | -2.40 | 0.016 | 0.44(0.23~0.86) |
| 多重用药(以是为参考) | |||||
| 否 | -0.62 | 0.21 | -2.93 | 0.003 | 0.54(0.36~0.81) |
Table 2 Multivariate Logistic regression analysis on influencing factors of frailty/pre-frailty in the elderly
| 因素 | β | SE | Wald χ2值 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| MNA-SF评分 | -0.34 | 0.08 | -4.36 | <0.001 | 0.71(0.61~0.83) |
| ACCI | 0.35 | 0.08 | 4.33 | <0.001 | 1.42(1.21~1.66) |
| HRR | -0.81 | 0.34 | -2.40 | 0.016 | 0.44(0.23~0.86) |
| 多重用药(以是为参考) | |||||
| 否 | -0.62 | 0.21 | -2.93 | 0.003 | 0.54(0.36~0.81) |
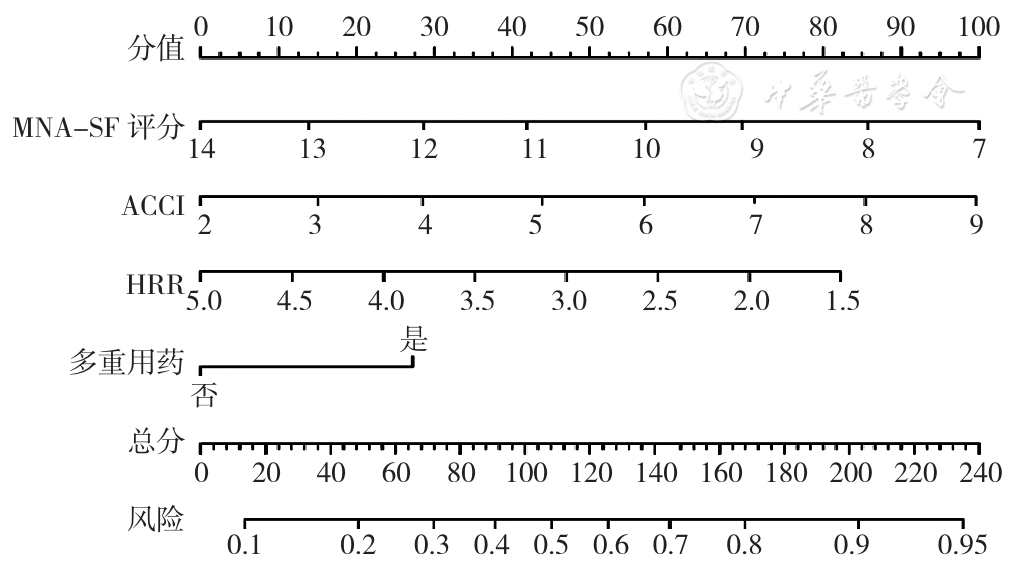
Figure 1 Nomogram for the risk of developing frailty/pre-frailty
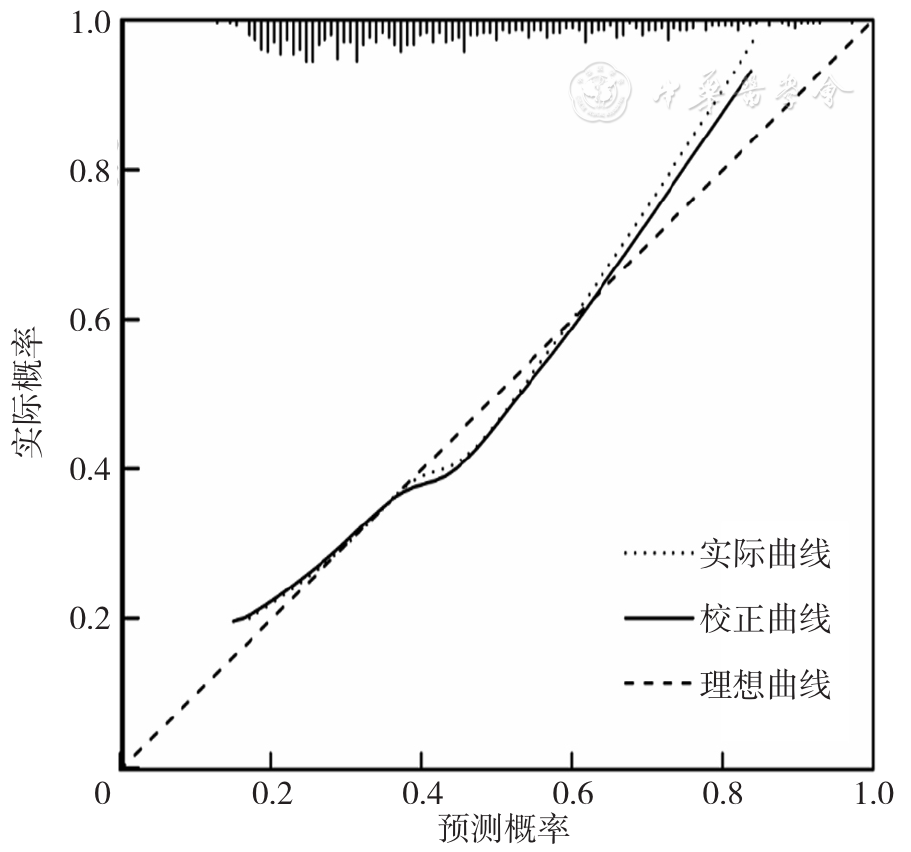
Figure 2 Hosmer-Lemeshow calibration curve of the nomogram
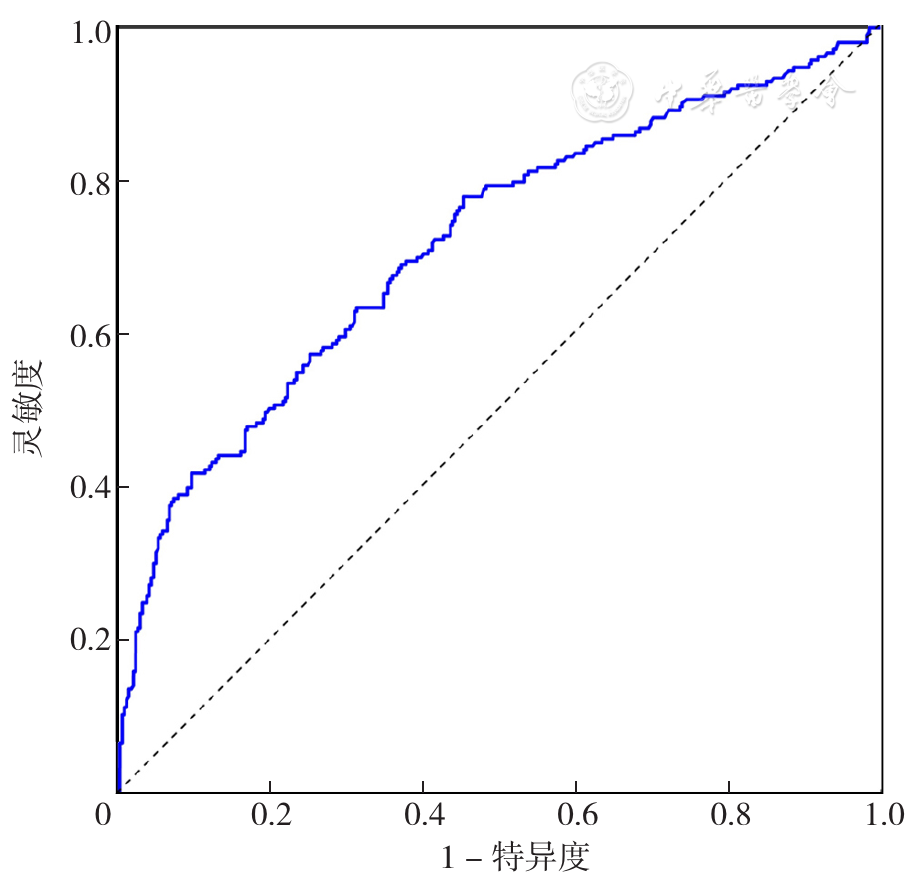
Figure 3 ROC curve of the nomogram to predict the risk of frailty/pre-frailty

Figure 4 DCA of the nomogram
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
中华医学会老年医学分会,《中华老年医学杂志》编辑委员会. 老年人衰弱预防中国专家共识(2022)[J]. 中华老年医学杂志,2022,41(5):503-511. DOI:10.3760/cma.j.issn.0254-9026.2022.05.001.
|
| [13] |
中国老年医学学会营养与食品安全分会,中国循证医学中心,《中国循证医学杂志》编辑委员会,等. 老年患者家庭营养管理中国专家共识(2017版)[J]. 中国循证医学杂志,2017,17(11):1251-1259. DOI:10.7507/1672-2531.201707095.
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [1] | ZOU Songyan, ZHANG Riyi, LI Xiaodong, MU Yinyu. Analysis of Clinical Characteristics and Risk Factors of Systemic Sclerosis Combined with Sjögren's Syndrome [J]. Chinese General Practice, 2025, 28(06): 737-741. |
| [2] | CHENG Lu, QIN Cun, BAI Pinqing, WANG Jianying, REN Yaping, HU Xiaojuan, ZHANG Baojun, ZHANG Lei, ZHOU Yixin. Correlation between Traditional Chinese Medicine Constitution and Blood Lipid Metabolism in Children: Based on the Shanghai Child and Adolescent Health Cohort [J]. Chinese General Practice, 2025, 28(06): 751-755. |
| [3] | DU Huijie, LIU Xingyu, XU Minghuan, YANG Xuezhi, ZHANG Huiqin, MO Jiali, LU Yi, KUANG Jie. Advances in the Prognostic Prediction of Acute Ischemic Stroke: Using Machine Learning Predictive Models as an Example [J]. Chinese General Practice, 2025, 28(05): 554-560. |
| [4] | YUE Haitao, HE Chanchan, CHENG Yuyou, ZHANG Sencheng, WU You, MA Jing. Coronary Heart Disease Risk Prediction Model Based on Machine Learning [J]. Chinese General Practice, 2025, 28(04): 499-509. |
| [5] | KONG Linghong, XIE Xiaoxin, FU Yanhua, GAN Lin, YANG Xiaoyan, MA Shujing, LONG Hai. Pre-treatment and Acquired Antiretroviral Drug Resistance among People Living with HIV in Southwest China [J]. Chinese General Practice, 2025, 28(02): 242-249. |
| [6] | LU Jing, SUN Guozhen, WANG Jie, GAO Min, YU Tianxi, SUN Shuyi, WANG Qin, WEN Gaoqin. Interpretable Analysis of Influencing Factors and the Current State of Social Frailty in Patients with Chronic Heart Failure [J]. Chinese General Practice, 2025, 28(02): 220-227. |
| [7] | ZHANG Gaoyu, WANG Zihan, GAO Xuefei, ZHANG Jin, DAI Tiangu, HE Qing, FAN Jiarong, HUANG Li, LI Lin. Research on the Development of a Risk Model for Coronary Heart Disease in Postmenopausal Hypertensive Women Based on the Triglyceride Glucose Index Combined with Vascular Elasticity Indicators [J]. Chinese General Practice, 2025, 28(01): 39-46. |
| [8] | LIU Mingbo, HE Xinye, YANG Xiaohong, WANG Zengwu. Interpretation of Report on Cardiovascular Health and Diseases in China 2023 [J]. Chinese General Practice, 2025, 28(01): 20-38. |
| [9] | TAO Jintao, WU Shouling, ZHAO Xiaohong. Prevalence and Risk Factors of Atrioventricular Block in the Population: a Study Based on the Kailuan Cohort [J]. Chinese General Practice, 2024, 27(36): 4534-4539. |
| [10] | GU Shanye, ZHOU Ziyi, CAI Yefeng. Study on Risk Prediction of Non-dementia Vascular Cognitive Impairment in Glycolipid Metabolic Diseases [J]. Chinese General Practice, 2024, 27(35): 4412-4416. |
| [11] | ZHOU Zhensen, HUANG Yan, CHENG Siwei, ZHANG Xiaoyu, ZHANG Xiaoyu, SUN Ting, YANG Xianjun, XIE Hui, MA Zuchang. Construction and Validation of a Screening Model for Early Atherosclerosis Risk in the Aorta [J]. Chinese General Practice, 2024, 27(33): 4147-4154. |
| [12] | ZHANG Bingqing, HU Xinyun, OUYANG Yuqin, XIANG Xinyue, TANG Wenjuan, FENG Wenhuan. Study on Nomogram Prediction Model for Risk Factors of Muscle Mass Loss in Non-obese Patients with Type 2 Diabetes [J]. Chinese General Practice, 2024, 27(33): 4139-4146. |
| [13] | Diabetes and Microcirculation Professional Committee of Chinese Society of Microcirculation, Primary Endocrine and Metabolic Diseases Group of the Chinese Society of Endocrinology. Expert Consensus on Screening and Prevention of Diabetic Microvascular Disease for Primary Care (2024) [J]. Chinese General Practice, 2024, 27(32): 3969-3986. |
| [14] | CHEN Muxin, LIANG Hao, ZHAO Yidi, YANG Xiaomin, FANG Jiamin, ZHOU Chunjiao, FU Xiuzhen, WEI Lin. Effectiveness Comparison of Different Frailty Assessment Tools in Preoperative Frailty Screening in the Elderly [J]. Chinese General Practice, 2024, 27(30): 3790-3796. |
| [15] | XU Yaolong, ZHAO Jiaxin, YANG Ligang. Epidemic Status and Risk Factors of Non-alcoholic Fatty Liver Disease [J]. Chinese General Practice, 2024, 27(30): 3825-3834. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||