中国全科医学 ›› 2024, Vol. 27 ›› Issue (25): 3108-3114.DOI: 10.12114/j.issn.1007-9572.2023.0415
所属专题: 全科医生最新文章合辑
曹德立1,2, 周巍2,*( ), 张修芳2, 姜琳2,3, 包兴2,4, 沈庆华2,5
), 张修芳2, 姜琳2,3, 包兴2,4, 沈庆华2,5
CAO Deli1,2, ZHOU Wei2,*(), ZHANG Xiufang2, JIANG Lin2,3, BAO Xing2,4, SHEN Qinghua2,5
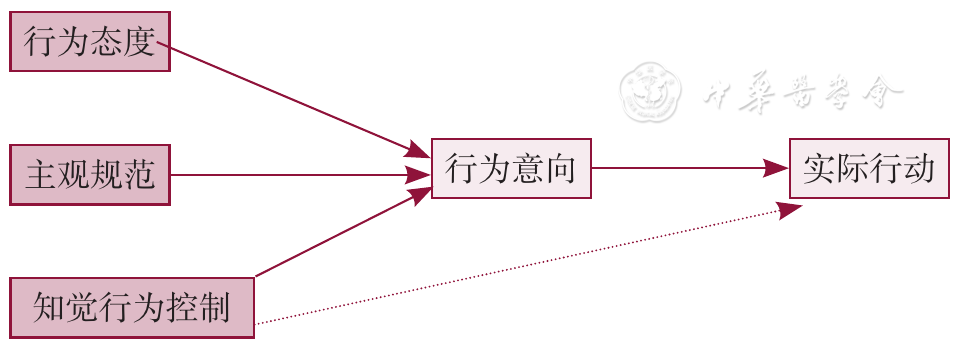
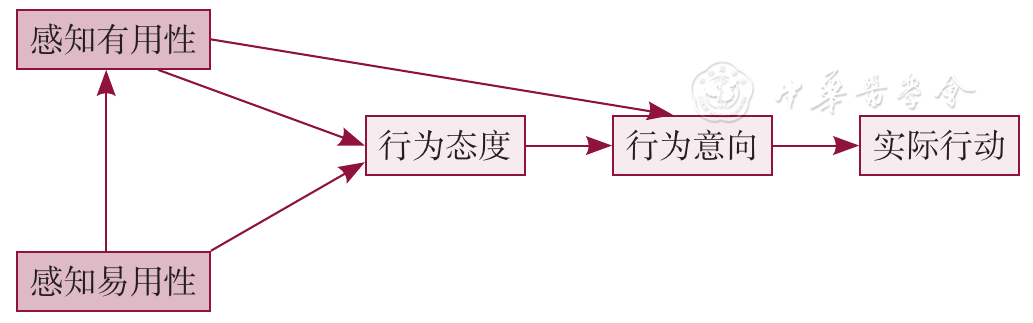
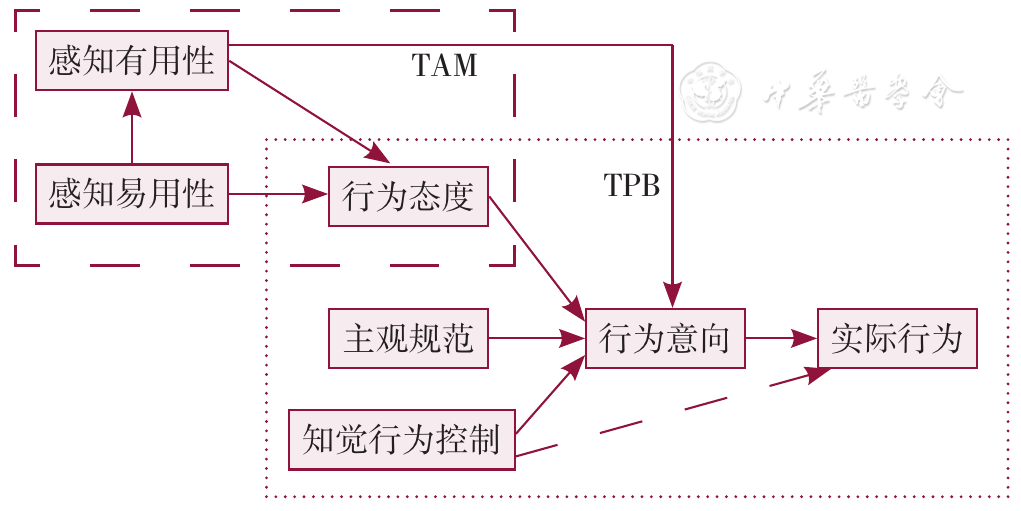
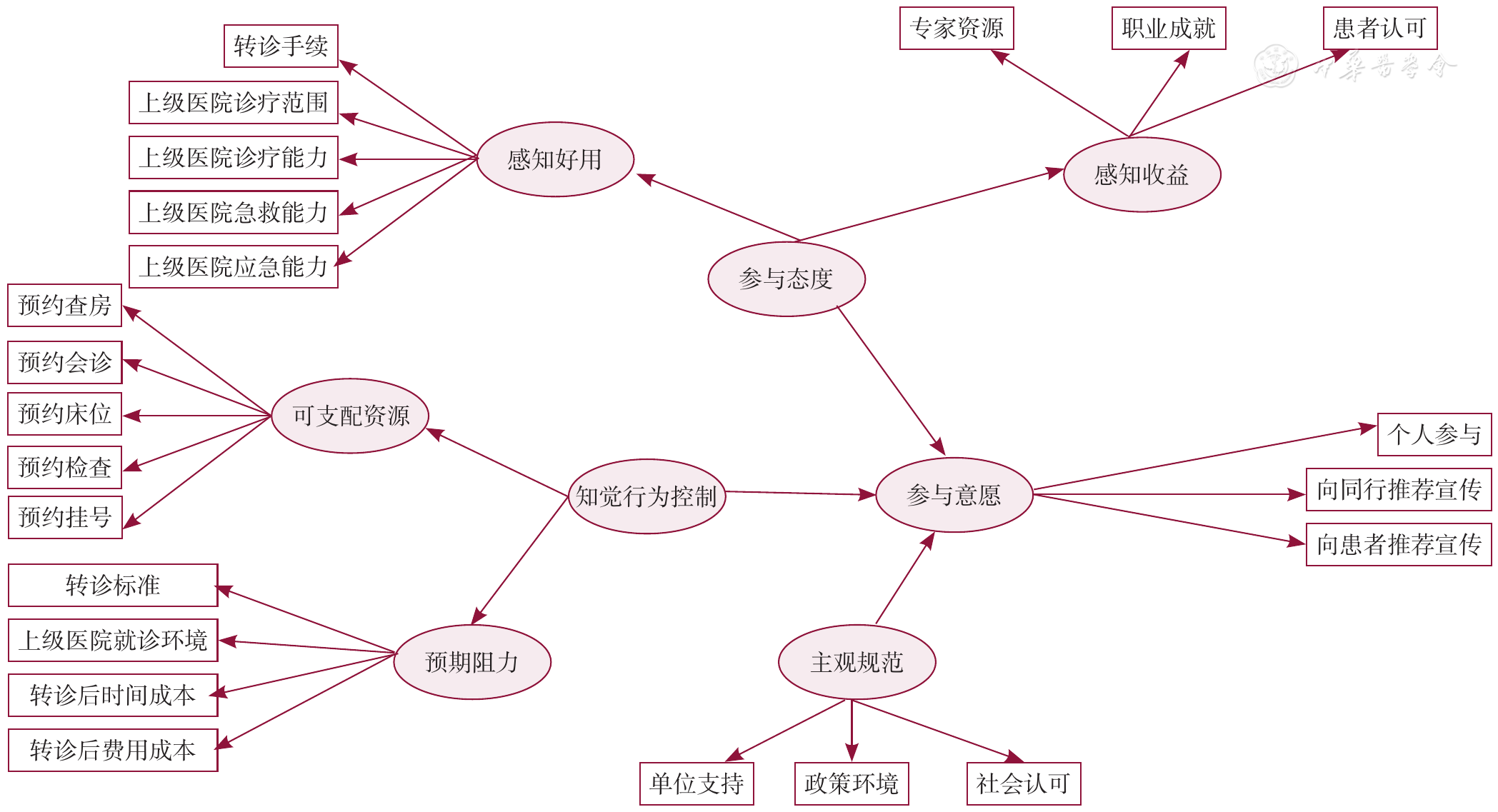
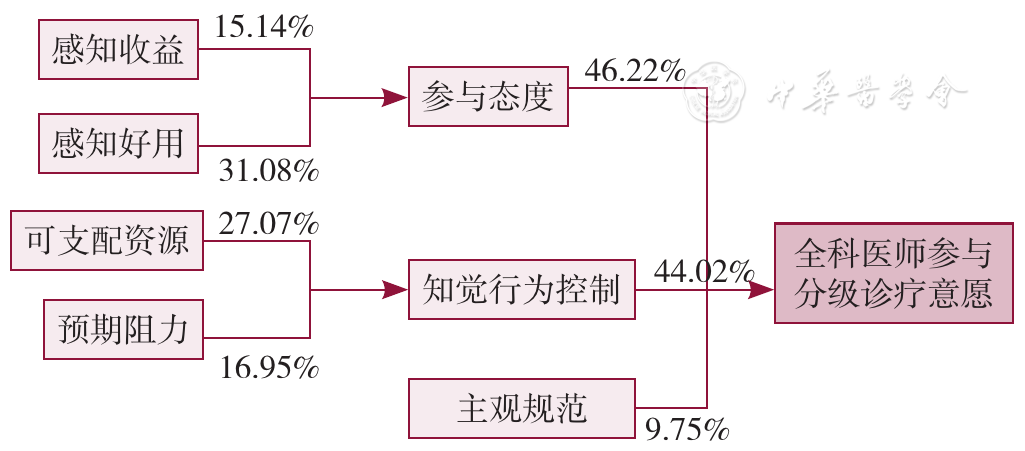
摘要: 背景 分级诊疗是医改的主要目标之一,2015年国务院办公厅发布的《关于推进分级诊疗制度建设的指导意见》(国办发〔2015〕70号)提出,2017年基层医疗卫生机构诊疗量占比要超过65.0%,但当年占比为54.2%,且近年来呈总体下降趋势。既往文献多针对需方(患者)开展研究,而作为分级诊疗的供方之一,全科医生参与分级诊疗意愿的调查研究较少。 目的 本文拟以苏州市为例,对全科医生参与分级诊疗意愿进行调查,对其影响因素进行分析,给出提高全科医生参与分级诊疗意愿的建议,为制定分级诊疗相关政策提供参考。 方法 于2022年6月,采取多阶段方便抽样方法,选取苏州市4县、6区175个基层医疗卫生机构的1 451名全科医生,采用自行编制的调查问卷展开调查。问卷内容包括全科医生的基本情况(人口学特征)调查、全科医生参与分级诊疗意愿调查(此部分问卷基于全科医生参与分级诊疗意愿影响因素拓展模型进行编制,此拓展模型为计划行为理论和技术接收模型的融合模型结合文献检索和访谈收集内容构建而成),根据问卷调查结果,使用结构方程模型检验全科医生参与分级诊疗意愿影响因素拓展模型拟合度,判定模型拟合效果;使用探索性因子分析计算全科医生参与分级诊疗意愿的各影响因素的权重(影响力),构建全科医生参与分级诊疗意愿影响因素影响关系模型。 结果 参与本次问卷调查的全科医生有1 451名,回收有效问卷1 302份,有效率89.73%。全科医生参与分级诊疗意愿影响因素拓展模型拟合良好。全科医生参与分级诊疗意愿影响因素影响关系中,参与态度、主观规范和知觉行为控制共同影响全科医生参与分级诊疗的意愿,三者权重分别为:46.22%、9.75%、44.02%;感知收益、感知好用共同解释参与态度,两者权重分别为15.14%、31.08%;可支配资源和预期阻力共同解释知觉行为控制,两者权重分别为27.07%、16.95%。 结论 全科医生对上级医院医疗服务能力认可程度、转诊手续繁简程度、上级医院医疗资源向全科医生放开程度,对全科医生参与分级诊疗意愿影响较大,建议从行政、组织、个人三个层面,采取加强医联体内人员交流互动、利用信息化手段简化转诊流程与手续、鼓励上级医院向全科医生定向定量放开门诊号源、病房床位等医疗资源的优先预约权限等多种措施,提高全科医生参与分级诊疗意愿。
中图分类号: