
Chinese General Practice ›› 2022, Vol. 25 ›› Issue (27): 3395-3403.DOI: 10.12114/j.issn.1007-9572.2022.0201
Special Issue: 泌尿系统疾病最新文章合辑; 高血压最新文章合辑; 中医最新文章合辑
• Article • Previous Articles Next Articles
Received:2022-03-22
Revised:2022-04-28
Published:2022-09-20
Online:2022-05-26
Contact:
Xiangmei CHEN
About author:
通讯作者:
陈香美
作者简介:基金资助:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2022.0201
Figure 1 Flow chart of participants selection
| 组别 | 例数 | 男性〔n(%)〕 | 年龄( | BMI( | 吸烟史〔n(%)〕 | 饮酒史〔n(%)〕 | 首发临床症状〔n(%)〕 | 高血压史〔n(%)〕 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 尿检异常 | 肉眼血尿 | 水肿 | 头痛头晕或恶心呕吐 | ||||||||
| IgAN组 | 85 | 47(55.3) | 38.0±10.9 | 24.7±3.8 | 27(31.8) | 32(37.6) | 63(74.1) | 12(14.1) | 9(10.6) | 5(5.9) | 35(41.2) |
| IgAN-MHT组 | 17 | 11(64.7) | 33.4±11.0 | 24.2±4.0 | 3(17.6) | 5(29.4) | 7(41.2) | 0 | 4(23.5) | 7(41.2) | 2(11.8) |
| 检验统计量值 | 0.512a | 1.560b | 0.553b | 1.360a | 0.416a | 7.140a | 1.530a | 1.128a | 13.770a | 5.301a | |
| P值 | 0.474 | 0.122 | 0.581 | 0.244 | 0.519 | 0.008 | 0.216 | 0.288 | <0.001 | 0.021 | |
| 组别 | 临床诊断〔n(%)〕 | 入院时平均动脉压〔M(P25,P75),mm Hg〕 | 最高收缩压〔M(P25,P75),mm Hg〕d | 最高舒张压〔M(P25,P75),mm Hg〕d | 丙氨酸氨基转移酶〔M(P25,P75),U/L〕 | ||||||
| 慢性肾炎综合征 | 肾病综合征 | 急性肾损伤 | |||||||||
| IgAN组 | 84(98.8) | 1(1.2) | 0 | 97(89,105) | 160(147,175) | 100(100,110) | 14.2(10.3,20.8) | ||||
| IgAN-MHT组 | 10(58.8) | 4(23.5) | 1(5.9) | 101(93,113) | 200(185,215) | 140(130,145) | 11.5(9.9,19.5) | ||||
| 检验统计量值 | 26.070a | —c | —c | -2.017 | -5.041 | -5.599 | -0.799 | ||||
| P值 | <0.001 | 0.003 | 0.167 | 0.044 | <0.001 | <0.001 | 0.424 | ||||
| 组别 | 天冬氨酸氨基转移酶〔M(P25,P75),U/L〕 | 血清总蛋白〔M(P25,P75),g/L〕 | 白蛋白〔M(P25,P75),g/L〕 | 血葡萄糖( | 血尿素氮〔M(P25,P75),mmol/L〕 | 血肌酐〔M(P25,P75),μmol/L〕 | 血尿酸〔M(P25,P75),μmol/L〕 | 总胆固醇〔M(P25,P75),mmol/L〕 | |||
| IgAN组 | 15.0(12.4,18.8) | 65.1(62.1,71.0) | 39.3(36.0,42.3) | 5.1±1.0 | 5.6(4.4,6.8) | 98.2(74.3,123.3) | 374.5(295.7,447.0) | 4.4(3.6,5.0) | |||
| IgAN-MHT组 | 12.3(11.5,16.6) | 60.3(56.7,69.9) | 38.0(34.3,41.2) | 4.6±0.7 | 8.0(6.4,15.6) | 171.4(105.7,391.2) | 428.4(357.7,451.2) | 4.2(3.6,4.7) | |||
| 检验统计量值 | -1.747 | -1.670 | -1.280 | 1.956b | -4.117 | -3.637 | -1.863 | -0.144 | |||
| P值 | 0.081 | 0.095 | 0.201 | 0.053 | <0.001 | <0.001 | 0.062 | 0.886 | |||
| 组别 | 三酰甘油〔M(P25,P75),mmol/L〕 | 高密度脂蛋白〔M(P25,P75),mmol/L〕 | 低密度脂蛋白〔M(P25,P75),mmol/L〕 | 钙( | 无机磷〔M(P25,P75),mmol/L〕 | 镁〔M(P25,P75),mmol/L〕 | 钾( | 钠( | 补体C3〔M(P25,P75),mg/dl〕 | ||
| IgAN组 | 1.7(1.3,2.5) | 1.0(0.8,1.3) | 2.8(2.3,3.2) | 2.2±0.1 | 1.2(1.0,1.3) | 0.8(0.8,0.9) | 4.0±0.3 | 141.1±2.1 | 106.0(94.6,120.0) | ||
| IgAN-MHT组 | 1.6(1.2,2.0) | 0.8(0.7,1.2) | 2.7(2.2,3.3) | 2.2±0.1 | 1.3(1.1,1.7) | 0.9(0.9,0.9) | 4.2±0.6 | 140.7±2.7 | 109.0(82.9,122.0) | ||
| 检验统计量值 | -0.804 | -1.280 | -0.260 | 0.511b | -2.048 | -2.366 | -1.847b | 0.564b | -0.445 | ||
| P值 | 0.422 | 0.201 | 0.795 | 0.610 | 0.041 | 0.018 | 0.068 | 0.574 | 0.657 | ||
| 组别 | 补体C4( | 血IgA〔M(P25,P75),mg/dl〕 | 血IgE〔M(P25,P75),IU/ml〕 | 血IgG〔M(P25,P75),mg/dl〕 | 血IgM〔M(P25,P75),mg/dl〕 | 24 h尿蛋白定量〔M(P25,P75),g/24 h〕 | 24 h尿蛋白定量分级〔n(%)〕 | ||||
| <1 g/24 h | 1~3.5 g/24 h | ≥3.5 g/24 h | |||||||||
| IgAN组 | 25.6±7.0 | 291.0(221.0,361.0) | 45.8(19.8,93.2) | 1 130.0(951.0,1 275.0) | 103.0(67.1,146.0) | 1.0(0.6,1.9) | 40(47.1) | 43(50.6) | 2(2.4) | ||
| IgAN-MHT组 | 27.2±8.4 | 314.0(246.0,374.5) | 75.3(30.8,230.0) | 959.0(716.5,1 135.0) | 65.4(40.2,107.3) | 2.0(1.4,3.9) | 2(11.8) | 9(52.9) | 6(35.3) | ||
| 检验统计量值 | -0.808b | -0.673 | -1.598 | -2.155 | -2.492 | -3.444 | 18.920a | ||||
| P值 | 0.421 | 0.501 | 0.110 | 0.031 | 0.013 | 0.001 | <0.001 | ||||
| 组别 | 血红蛋白( | 血小板计数( | 尿红细胞检查(镜检)〔M(P25,P75),/HPF〕 | eGFR〔M(P25,P75),ml·min-1·(1.73 m2)-1〕 | CKD分期〔n(%)〕 | ||||||
| 1 | 2 | 3a | 3b | 4 | 5 | ||||||
| IgAN组 | 131.0±17.7 | 243.7±54.8 | 6.5(3.0,18.3) | 80.5(57.3,105.4) | 33(38.8) | 28(32.9) | 13(15.3) | 9(10.6) | 2(2.4) | 0 | |
| IgAN-MHT组 | 129.4±23.3 | 225.1±55.6 | 4.0(0.5,11.8) | 46.7(19.1,76.9) | 1(5.9) | 5(29.4) | 3(17.6) | 3(17.6) | 2(11.8) | 3(17.6) | |
| 检验统计量值 | 0.310b | 1.277b | -1.130 | -3.722 | 19.122c | ||||||
| P值 | 0.757 | 0.205 | 0.259 | <0.001 | 0.001 | ||||||
Table 1 Comparison of clinical data of IgA nephropathy patients with and without malignant hypertension
| 组别 | 例数 | 男性〔n(%)〕 | 年龄( | BMI( | 吸烟史〔n(%)〕 | 饮酒史〔n(%)〕 | 首发临床症状〔n(%)〕 | 高血压史〔n(%)〕 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 尿检异常 | 肉眼血尿 | 水肿 | 头痛头晕或恶心呕吐 | ||||||||
| IgAN组 | 85 | 47(55.3) | 38.0±10.9 | 24.7±3.8 | 27(31.8) | 32(37.6) | 63(74.1) | 12(14.1) | 9(10.6) | 5(5.9) | 35(41.2) |
| IgAN-MHT组 | 17 | 11(64.7) | 33.4±11.0 | 24.2±4.0 | 3(17.6) | 5(29.4) | 7(41.2) | 0 | 4(23.5) | 7(41.2) | 2(11.8) |
| 检验统计量值 | 0.512a | 1.560b | 0.553b | 1.360a | 0.416a | 7.140a | 1.530a | 1.128a | 13.770a | 5.301a | |
| P值 | 0.474 | 0.122 | 0.581 | 0.244 | 0.519 | 0.008 | 0.216 | 0.288 | <0.001 | 0.021 | |
| 组别 | 临床诊断〔n(%)〕 | 入院时平均动脉压〔M(P25,P75),mm Hg〕 | 最高收缩压〔M(P25,P75),mm Hg〕d | 最高舒张压〔M(P25,P75),mm Hg〕d | 丙氨酸氨基转移酶〔M(P25,P75),U/L〕 | ||||||
| 慢性肾炎综合征 | 肾病综合征 | 急性肾损伤 | |||||||||
| IgAN组 | 84(98.8) | 1(1.2) | 0 | 97(89,105) | 160(147,175) | 100(100,110) | 14.2(10.3,20.8) | ||||
| IgAN-MHT组 | 10(58.8) | 4(23.5) | 1(5.9) | 101(93,113) | 200(185,215) | 140(130,145) | 11.5(9.9,19.5) | ||||
| 检验统计量值 | 26.070a | —c | —c | -2.017 | -5.041 | -5.599 | -0.799 | ||||
| P值 | <0.001 | 0.003 | 0.167 | 0.044 | <0.001 | <0.001 | 0.424 | ||||
| 组别 | 天冬氨酸氨基转移酶〔M(P25,P75),U/L〕 | 血清总蛋白〔M(P25,P75),g/L〕 | 白蛋白〔M(P25,P75),g/L〕 | 血葡萄糖( | 血尿素氮〔M(P25,P75),mmol/L〕 | 血肌酐〔M(P25,P75),μmol/L〕 | 血尿酸〔M(P25,P75),μmol/L〕 | 总胆固醇〔M(P25,P75),mmol/L〕 | |||
| IgAN组 | 15.0(12.4,18.8) | 65.1(62.1,71.0) | 39.3(36.0,42.3) | 5.1±1.0 | 5.6(4.4,6.8) | 98.2(74.3,123.3) | 374.5(295.7,447.0) | 4.4(3.6,5.0) | |||
| IgAN-MHT组 | 12.3(11.5,16.6) | 60.3(56.7,69.9) | 38.0(34.3,41.2) | 4.6±0.7 | 8.0(6.4,15.6) | 171.4(105.7,391.2) | 428.4(357.7,451.2) | 4.2(3.6,4.7) | |||
| 检验统计量值 | -1.747 | -1.670 | -1.280 | 1.956b | -4.117 | -3.637 | -1.863 | -0.144 | |||
| P值 | 0.081 | 0.095 | 0.201 | 0.053 | <0.001 | <0.001 | 0.062 | 0.886 | |||
| 组别 | 三酰甘油〔M(P25,P75),mmol/L〕 | 高密度脂蛋白〔M(P25,P75),mmol/L〕 | 低密度脂蛋白〔M(P25,P75),mmol/L〕 | 钙( | 无机磷〔M(P25,P75),mmol/L〕 | 镁〔M(P25,P75),mmol/L〕 | 钾( | 钠( | 补体C3〔M(P25,P75),mg/dl〕 | ||
| IgAN组 | 1.7(1.3,2.5) | 1.0(0.8,1.3) | 2.8(2.3,3.2) | 2.2±0.1 | 1.2(1.0,1.3) | 0.8(0.8,0.9) | 4.0±0.3 | 141.1±2.1 | 106.0(94.6,120.0) | ||
| IgAN-MHT组 | 1.6(1.2,2.0) | 0.8(0.7,1.2) | 2.7(2.2,3.3) | 2.2±0.1 | 1.3(1.1,1.7) | 0.9(0.9,0.9) | 4.2±0.6 | 140.7±2.7 | 109.0(82.9,122.0) | ||
| 检验统计量值 | -0.804 | -1.280 | -0.260 | 0.511b | -2.048 | -2.366 | -1.847b | 0.564b | -0.445 | ||
| P值 | 0.422 | 0.201 | 0.795 | 0.610 | 0.041 | 0.018 | 0.068 | 0.574 | 0.657 | ||
| 组别 | 补体C4( | 血IgA〔M(P25,P75),mg/dl〕 | 血IgE〔M(P25,P75),IU/ml〕 | 血IgG〔M(P25,P75),mg/dl〕 | 血IgM〔M(P25,P75),mg/dl〕 | 24 h尿蛋白定量〔M(P25,P75),g/24 h〕 | 24 h尿蛋白定量分级〔n(%)〕 | ||||
| <1 g/24 h | 1~3.5 g/24 h | ≥3.5 g/24 h | |||||||||
| IgAN组 | 25.6±7.0 | 291.0(221.0,361.0) | 45.8(19.8,93.2) | 1 130.0(951.0,1 275.0) | 103.0(67.1,146.0) | 1.0(0.6,1.9) | 40(47.1) | 43(50.6) | 2(2.4) | ||
| IgAN-MHT组 | 27.2±8.4 | 314.0(246.0,374.5) | 75.3(30.8,230.0) | 959.0(716.5,1 135.0) | 65.4(40.2,107.3) | 2.0(1.4,3.9) | 2(11.8) | 9(52.9) | 6(35.3) | ||
| 检验统计量值 | -0.808b | -0.673 | -1.598 | -2.155 | -2.492 | -3.444 | 18.920a | ||||
| P值 | 0.421 | 0.501 | 0.110 | 0.031 | 0.013 | 0.001 | <0.001 | ||||
| 组别 | 血红蛋白( | 血小板计数( | 尿红细胞检查(镜检)〔M(P25,P75),/HPF〕 | eGFR〔M(P25,P75),ml·min-1·(1.73 m2)-1〕 | CKD分期〔n(%)〕 | ||||||
| 1 | 2 | 3a | 3b | 4 | 5 | ||||||
| IgAN组 | 131.0±17.7 | 243.7±54.8 | 6.5(3.0,18.3) | 80.5(57.3,105.4) | 33(38.8) | 28(32.9) | 13(15.3) | 9(10.6) | 2(2.4) | 0 | |
| IgAN-MHT组 | 129.4±23.3 | 225.1±55.6 | 4.0(0.5,11.8) | 46.7(19.1,76.9) | 1(5.9) | 5(29.4) | 3(17.6) | 3(17.6) | 2(11.8) | 3(17.6) | |
| 检验统计量值 | 0.310b | 1.277b | -1.130 | -3.722 | 19.122c | ||||||
| P值 | 0.757 | 0.205 | 0.259 | <0.001 | 0.001 | ||||||
| 组别 | 例数 | 主证 | 兼证 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 肺脾气虚证 | 气阴两虚证 | 肝肾阴虚证 | 脾肾阳虚证 | 水湿 | 痰湿 | 湿热 | 寒湿 | 血瘀 | 肝郁 | 浊毒 | ||
| IgAN组 | 85 | 15(17.6) | 39(45.9) | 18(21.2) | 13(15.3) | 9(10.6) | 10(11.8) | 22(25.9) | 1(1.2) | 20(23.5) | 16(18.8) | 7(8.2) |
| IgAN-MHT组 | 17 | 4(23.5) | 7(41.2) | 3(17.6) | 3(17.6) | 3(17.6) | 1(5.9) | 5(29.4) | 0 | 9(52.9) | 3(17.6) | 0 |
| χ2值 | 0.052 | 0.127 | 0 | 0 | 0.170 | 0.082 | 0 | — | 4.664 | 0 | 0.491 | |
| P值 | 0.820 | 0.722 | 1 | 1 | 0.680 | 0.775 | 1 | 1 | 0.031 | 1 | 0.484 | |
Table 2 Comparison of main syndromes and concurrent syndromes of TCM in IgA nephropathy patients with and without malignant hypertension
| 组别 | 例数 | 主证 | 兼证 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 肺脾气虚证 | 气阴两虚证 | 肝肾阴虚证 | 脾肾阳虚证 | 水湿 | 痰湿 | 湿热 | 寒湿 | 血瘀 | 肝郁 | 浊毒 | ||
| IgAN组 | 85 | 15(17.6) | 39(45.9) | 18(21.2) | 13(15.3) | 9(10.6) | 10(11.8) | 22(25.9) | 1(1.2) | 20(23.5) | 16(18.8) | 7(8.2) |
| IgAN-MHT组 | 17 | 4(23.5) | 7(41.2) | 3(17.6) | 3(17.6) | 3(17.6) | 1(5.9) | 5(29.4) | 0 | 9(52.9) | 3(17.6) | 0 |
| χ2值 | 0.052 | 0.127 | 0 | 0 | 0.170 | 0.082 | 0 | — | 4.664 | 0 | 0.491 | |
| P值 | 0.820 | 0.722 | 1 | 1 | 0.680 | 0.775 | 1 | 1 | 0.031 | 1 | 0.484 | |
| 组别 | 例数 | 气虚证 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 易感冒 | 神疲乏力 | 少气懒言 | 自汗 | 四肢倦怠 | 胫酸腿软 | 头目眩晕 | 头痛 | 恶心 | 呕吐 | 便溏 | ||
| IgAN组 | 85 | 30(35.3) | 40(47.1) | 17(20.0) | 33(38.8) | 14(16.5) | 4(4.7) | 22(25.9) | 18(21.2) | 7(8.2) | 3(3.5) | 10(11.8) |
| IgAN-MHT组 | 17 | 4(23.5) | 13(76.5) | 7(41.2) | 5(29.4) | 7(41.2) | 5(29.4) | 10(58.8) | 12(70.6) | 5(29.4) | 4(23.5) | 4(23.5) |
| χ2值 | 0.882 | 4.910 | 2.452 | 0.537 | 3.886 | 7.897 | 7.140 | 16.66 | 4.250 | 6.013 | 0.811 | |
| P值 | 0.348 | 0.027 | 0.117 | 0.464 | 0.049 | 0.005 | 0.008 | <0.001 | 0.039 | 0.014 | 0.368 | |
| 组别 | 阴虚证 | 血瘀证 | ||||||||||
| 视物模糊 | 飞蚊症 | 耳聋 | 手足心热 | 盗汗 | 口干/咽燥 | 舌苔干燥 | 面色黧黑 | 爪甲青紫 | 定位刺痛、夜间加重 | 舌色紫暗 | ||
| IgAN组 | 21(24.7) | 3(3.5) | 6(7.1) | 34(40.0) | 18(21.2) | 28(32.9) | 7(8.2) | 16(18.8) | 2(2.4) | 7(8.2) | 17(20.0) | |
| IgAN-MHT组 | 12(70.6) | 6(35.3) | 5(29.4) | 7(41.2) | 4(23.5) | 7(41.2) | 5(29.4) | 5(29.4) | 4(23.5) | 2(11.8) | 8(47.1) | |
| χ2值 | 13.627 | 14.039 | 5.217 | 0.008 | 0 | 0.426 | 4.25 | 0.432 | 7.969 | 0 | 4.239 | |
| P值 | <0.001 | <0.001 | 0.022 | 0.928 | 1 | 0.514 | 0.039 | 0.511 | 0.005 | 1 | 0.040 | |
Table 3 Comparison of TCM symptoms in IgA nephropathy patients with and without malignant hypertension
| 组别 | 例数 | 气虚证 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 易感冒 | 神疲乏力 | 少气懒言 | 自汗 | 四肢倦怠 | 胫酸腿软 | 头目眩晕 | 头痛 | 恶心 | 呕吐 | 便溏 | ||
| IgAN组 | 85 | 30(35.3) | 40(47.1) | 17(20.0) | 33(38.8) | 14(16.5) | 4(4.7) | 22(25.9) | 18(21.2) | 7(8.2) | 3(3.5) | 10(11.8) |
| IgAN-MHT组 | 17 | 4(23.5) | 13(76.5) | 7(41.2) | 5(29.4) | 7(41.2) | 5(29.4) | 10(58.8) | 12(70.6) | 5(29.4) | 4(23.5) | 4(23.5) |
| χ2值 | 0.882 | 4.910 | 2.452 | 0.537 | 3.886 | 7.897 | 7.140 | 16.66 | 4.250 | 6.013 | 0.811 | |
| P值 | 0.348 | 0.027 | 0.117 | 0.464 | 0.049 | 0.005 | 0.008 | <0.001 | 0.039 | 0.014 | 0.368 | |
| 组别 | 阴虚证 | 血瘀证 | ||||||||||
| 视物模糊 | 飞蚊症 | 耳聋 | 手足心热 | 盗汗 | 口干/咽燥 | 舌苔干燥 | 面色黧黑 | 爪甲青紫 | 定位刺痛、夜间加重 | 舌色紫暗 | ||
| IgAN组 | 21(24.7) | 3(3.5) | 6(7.1) | 34(40.0) | 18(21.2) | 28(32.9) | 7(8.2) | 16(18.8) | 2(2.4) | 7(8.2) | 17(20.0) | |
| IgAN-MHT组 | 12(70.6) | 6(35.3) | 5(29.4) | 7(41.2) | 4(23.5) | 7(41.2) | 5(29.4) | 5(29.4) | 4(23.5) | 2(11.8) | 8(47.1) | |
| χ2值 | 13.627 | 14.039 | 5.217 | 0.008 | 0 | 0.426 | 4.25 | 0.432 | 7.969 | 0 | 4.239 | |
| P值 | <0.001 | <0.001 | 0.022 | 0.928 | 1 | 0.514 | 0.039 | 0.511 | 0.005 | 1 | 0.040 | |
| 组别 | 例数 | M病变 | E病变 | S病变 | T病变 | C病变 | 肾内动脉硬化 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M0 | M1 | E0 | E1 | S0 | S1 | T0 | T1 | T2 | C0 | C1 | C2 | |||
| IgAN组 | 85 | 48(56.5) | 37(43.5) | 66(77.6) | 19(22.4) | 27(31.8) | 58(68.2) | 40(47.1) | 34(40.0) | 11(12.9) | 60(70.6) | 24(28.2) | 1(1.2) | 55(64.7) |
| IgAN-MHT组 | 17 | 11(64.7) | 6(35.3) | 16(94.1) | 1(5.9) | 1(5.9) | 16(94.1) | 3(17.6) | 4(23.5) | 10(58.8) | 11(64.7) | 6(35.3) | 0 | 16(94.1) |
| χ2值 | 0.394 | 1.505 | 3.554 | 15.515 | — | 5.793 | ||||||||
| P值 | 0.530 | 0.220 | 0.059 | <0.001 | 0.644 | 0.016 | ||||||||
Table 4 Comparison of Oxford classification of IgA nephropathy in IgA nephropathy patients with and without malignant hypertension
| 组别 | 例数 | M病变 | E病变 | S病变 | T病变 | C病变 | 肾内动脉硬化 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M0 | M1 | E0 | E1 | S0 | S1 | T0 | T1 | T2 | C0 | C1 | C2 | |||
| IgAN组 | 85 | 48(56.5) | 37(43.5) | 66(77.6) | 19(22.4) | 27(31.8) | 58(68.2) | 40(47.1) | 34(40.0) | 11(12.9) | 60(70.6) | 24(28.2) | 1(1.2) | 55(64.7) |
| IgAN-MHT组 | 17 | 11(64.7) | 6(35.3) | 16(94.1) | 1(5.9) | 1(5.9) | 16(94.1) | 3(17.6) | 4(23.5) | 10(58.8) | 11(64.7) | 6(35.3) | 0 | 16(94.1) |
| χ2值 | 0.394 | 1.505 | 3.554 | 15.515 | — | 5.793 | ||||||||
| P值 | 0.530 | 0.220 | 0.059 | <0.001 | 0.644 | 0.016 | ||||||||
| 指标 | IgAN-MHT | |
|---|---|---|
| rs值 | P值 | |
| 气虚证 | 0.009 | 0.928 |
| 阴虚证 | -0.065 | 0.519 |
| 水湿证 | 0.082 | 0.415 |
| 痰湿证 | -0.071 | 0.480 |
| 湿热证 | 0.030 | 0.766 |
| 寒湿证 | -0.044 | 0.657 |
| 血瘀证 | 0.664 | <0.001 |
| 肝郁证 | 0.044 | 0.659 |
| 浊毒证 | -0.121 | 0.224 |
Table 5 Correlation of malignant hypertension in IgA nephropathy with TCM syndromes
| 指标 | IgAN-MHT | |
|---|---|---|
| rs值 | P值 | |
| 气虚证 | 0.009 | 0.928 |
| 阴虚证 | -0.065 | 0.519 |
| 水湿证 | 0.082 | 0.415 |
| 痰湿证 | -0.071 | 0.480 |
| 湿热证 | 0.030 | 0.766 |
| 寒湿证 | -0.044 | 0.657 |
| 血瘀证 | 0.664 | <0.001 |
| 肝郁证 | 0.044 | 0.659 |
| 浊毒证 | -0.121 | 0.224 |
| 临床指标 | 气虚证 | 阴虚证 | 血瘀证 | |||
|---|---|---|---|---|---|---|
| rs值 | P值 | rs值 | P值 | rs值 | P值 | |
| 性别(以女性为参照) | 0.485 | 0.049 | 0.118 | 0.653 | -0.044 | 0.868 |
| 年龄 | -0.151 | 0.563 | 0.012 | 0.963 | -0.096 | 0.713 |
| 吸烟史 | 0.019 | 0.942 | -0.240 | 0.354 | -0.182 | 0.485 |
| 饮酒史 | 0.207 | 0.426 | -0.247 | 0.339 | -0.167 | 0.521 |
| 入院时收缩压 | -0.013 | 0.962 | 0.539 | 0.025 | 0.133 | 0.611 |
| 入院时舒张压 | 0.025 | 0.924 | 0.343 | 0.178 | 0.060 | 0.818 |
| 丙氨酸氨基转移酶 | 0.050 | 0.848 | 0.024 | 0.926 | 0.192 | 0.459 |
| 天冬氨酸氨基转移酶 | 0.138 | 0.597 | 0.232 | 0.370 | 0.132 | 0.612 |
| 血清总蛋白 | -0.176 | 0.499 | 0.293 | 0.254 | -0.072 | 0.783 |
| 白蛋白 | -0.151 | 0.564 | 0.293 | 0.254 | 0 | 1.000 |
| 血葡萄糖 | 0.025 | 0.924 | 0.110 | 0.675 | -0.193 | 0.459 |
| 血尿素氮 | 0.302 | 0.240 | -0.244 | 0.345 | -0.048 | 0.855 |
| 血肌酐 | 0.427 | 0.087 | -0.317 | 0.215 | -0.072 | 0.783 |
| 血尿酸 | 0.377 | 0.136 | -0.415 | 0.098 | -0.072 | 0.783 |
| 总胆固醇 | 0.151 | 0.564 | -0.244 | 0.345 | -0.313 | 0.222 |
| 三酰甘油 | 0.251 | 0.331 | -0.244 | 0.345 | -0.361 | 0.155 |
| 高密度脂蛋白 | 0.031 | 0.911 | 0.346 | 0.206 | 0.278 | 0.315 |
| 低密度脂蛋白 | 0.047 | 0.867 | -0.142 | 0.614 | -0.139 | 0.620 |
| 钙 | 0.038 | 0.886 | 0.244 | 0.345 | -0.096 | 0.713 |
| 无机磷 | 0.176 | 0.499 | -0.525 | 0.030 | 0.072 | 0.783 |
| 镁 | 0.417 | 0.096 | 0.012 | 0.963 | -0.012 | 0.963 |
| 钾 | 0.201 | 0.439 | -0.634 | 0.006 | -0.409 | 0.103 |
| 钠 | -0.226 | 0.383 | -0.305 | 0.234 | -0.144 | 0.580 |
| 24 h尿蛋白定量 | 0.503 | 0.040 | -0.366 | 0.149 | -0.361 | 0.155 |
| 血红蛋白 | 0.251 | 0.330 | -0.085 | 0.744 | -0.156 | 0.549 |
| 血小板计数 | -0.063 | 0.811 | -0.232 | 0.370 | -0.289 | 0.261 |
| 尿红细胞检查(镜检)/HPF | -0.202 | 0.436 | -0.147 | 0.572 | 0.085 | 0.746 |
| eGFR | -0.352 | 0.166 | 0.268 | 0.298 | 0.072 | 0.783 |
Table 6 Correlation analysis of Western medicine clinical indicators and TCM syndromes in IgA nephropathy patients with malignant hypertension
| 临床指标 | 气虚证 | 阴虚证 | 血瘀证 | |||
|---|---|---|---|---|---|---|
| rs值 | P值 | rs值 | P值 | rs值 | P值 | |
| 性别(以女性为参照) | 0.485 | 0.049 | 0.118 | 0.653 | -0.044 | 0.868 |
| 年龄 | -0.151 | 0.563 | 0.012 | 0.963 | -0.096 | 0.713 |
| 吸烟史 | 0.019 | 0.942 | -0.240 | 0.354 | -0.182 | 0.485 |
| 饮酒史 | 0.207 | 0.426 | -0.247 | 0.339 | -0.167 | 0.521 |
| 入院时收缩压 | -0.013 | 0.962 | 0.539 | 0.025 | 0.133 | 0.611 |
| 入院时舒张压 | 0.025 | 0.924 | 0.343 | 0.178 | 0.060 | 0.818 |
| 丙氨酸氨基转移酶 | 0.050 | 0.848 | 0.024 | 0.926 | 0.192 | 0.459 |
| 天冬氨酸氨基转移酶 | 0.138 | 0.597 | 0.232 | 0.370 | 0.132 | 0.612 |
| 血清总蛋白 | -0.176 | 0.499 | 0.293 | 0.254 | -0.072 | 0.783 |
| 白蛋白 | -0.151 | 0.564 | 0.293 | 0.254 | 0 | 1.000 |
| 血葡萄糖 | 0.025 | 0.924 | 0.110 | 0.675 | -0.193 | 0.459 |
| 血尿素氮 | 0.302 | 0.240 | -0.244 | 0.345 | -0.048 | 0.855 |
| 血肌酐 | 0.427 | 0.087 | -0.317 | 0.215 | -0.072 | 0.783 |
| 血尿酸 | 0.377 | 0.136 | -0.415 | 0.098 | -0.072 | 0.783 |
| 总胆固醇 | 0.151 | 0.564 | -0.244 | 0.345 | -0.313 | 0.222 |
| 三酰甘油 | 0.251 | 0.331 | -0.244 | 0.345 | -0.361 | 0.155 |
| 高密度脂蛋白 | 0.031 | 0.911 | 0.346 | 0.206 | 0.278 | 0.315 |
| 低密度脂蛋白 | 0.047 | 0.867 | -0.142 | 0.614 | -0.139 | 0.620 |
| 钙 | 0.038 | 0.886 | 0.244 | 0.345 | -0.096 | 0.713 |
| 无机磷 | 0.176 | 0.499 | -0.525 | 0.030 | 0.072 | 0.783 |
| 镁 | 0.417 | 0.096 | 0.012 | 0.963 | -0.012 | 0.963 |
| 钾 | 0.201 | 0.439 | -0.634 | 0.006 | -0.409 | 0.103 |
| 钠 | -0.226 | 0.383 | -0.305 | 0.234 | -0.144 | 0.580 |
| 24 h尿蛋白定量 | 0.503 | 0.040 | -0.366 | 0.149 | -0.361 | 0.155 |
| 血红蛋白 | 0.251 | 0.330 | -0.085 | 0.744 | -0.156 | 0.549 |
| 血小板计数 | -0.063 | 0.811 | -0.232 | 0.370 | -0.289 | 0.261 |
| 尿红细胞检查(镜检)/HPF | -0.202 | 0.436 | -0.147 | 0.572 | 0.085 | 0.746 |
| eGFR | -0.352 | 0.166 | 0.268 | 0.298 | 0.072 | 0.783 |
| 临床指标 | 气虚证 | 阴虚证 | 血瘀证 | |||
|---|---|---|---|---|---|---|
| rs值 | P值 | rs值 | P值 | rs值 | P值 | |
| M病变 | 0.288 | 0.263 | -0.132 | 0.612 | 0.203 | 0.434 |
| E病变 | 0.185 | 0.478 | -0.299 | 0.244 | 0.236 | 0.362 |
| S病变 | -0.185 | 0.478 | -0.209 | 0.420 | -0.236 | 0.362 |
| T病变 | 0.207 | 0.207 | 0.161 | 0.537 | 0.502 | 0.040 |
| C病变 | 0.030 | 0.908 | -0.132 | 0.612 | -0.044 | 0.868 |
Table 7 Correlation analysis of pathological indices and TCM syndromes in IgA nephropathy patients with malignant hypertension
| 临床指标 | 气虚证 | 阴虚证 | 血瘀证 | |||
|---|---|---|---|---|---|---|
| rs值 | P值 | rs值 | P值 | rs值 | P值 | |
| M病变 | 0.288 | 0.263 | -0.132 | 0.612 | 0.203 | 0.434 |
| E病变 | 0.185 | 0.478 | -0.299 | 0.244 | 0.236 | 0.362 |
| S病变 | -0.185 | 0.478 | -0.209 | 0.420 | -0.236 | 0.362 |
| T病变 | 0.207 | 0.207 | 0.161 | 0.537 | 0.502 | 0.040 |
| C病变 | 0.030 | 0.908 | -0.132 | 0.612 | -0.044 | 0.868 |
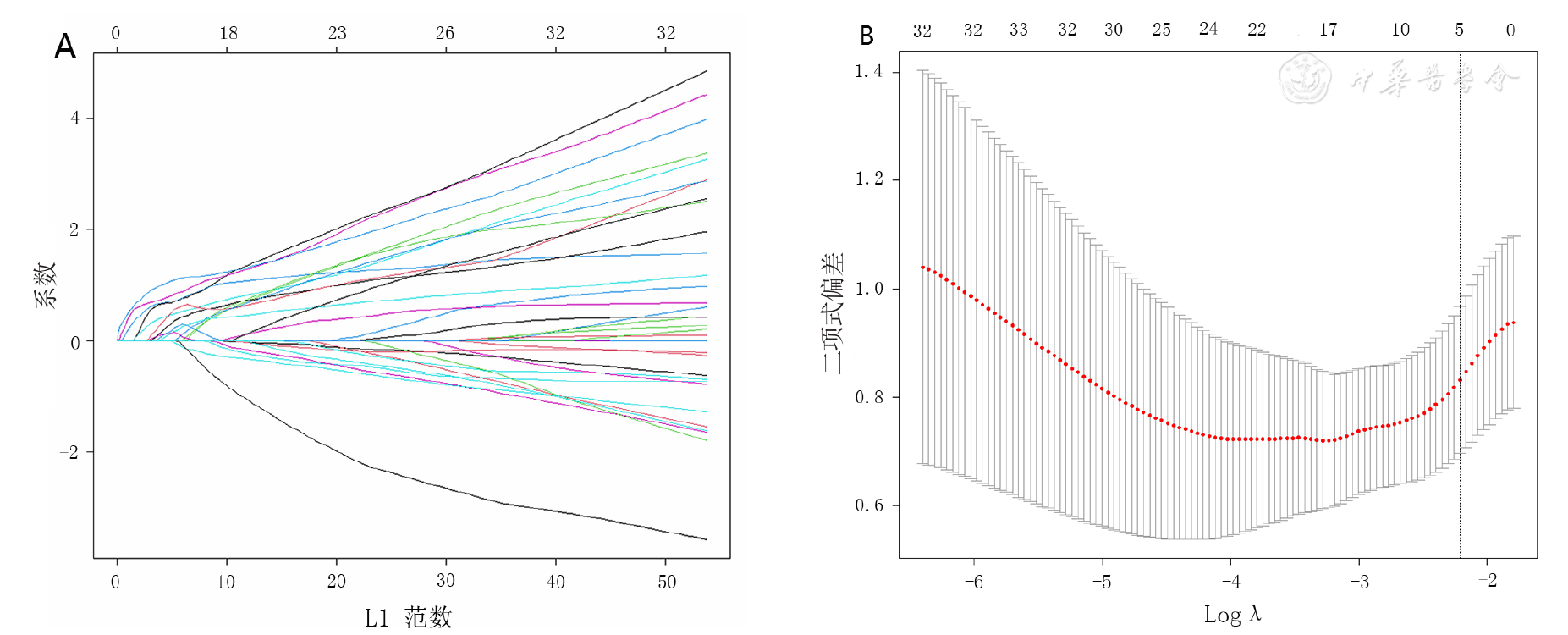
Figure 2 Screening TCM-related factors of malignant hypertension in IgA nephropathyby LASSO regression model
| 指标 | B | SE | Waldχ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 形寒肢冷 | -0.724 | 0.614 | 1.392 | 0.238 | 0.485 | (0.146,1.614) |
| 肌肤干燥 | -0.836 | 0.795 | 1.106 | 0.293 | 0.433 | (0.091,2.058) |
| 爪甲青紫 | 2.547 | 0.916 | 7.733 | 0.005 | 12.769 | (2.121,76.882) |
| 口唇青紫 | -0.414 | 0.617 | 0.450 | 0.502 | 0.661 | (0.197,2.217 ) |
| 面色晦暗 | -0.773 | 0.613 | 1.590 | 0.207 | 0.462 | (0.139,1.535) |
| 颧红 | 1.037 | 0.764 | 1.842 | 0.175 | 2.821 | (0.631,12.618) |
| 头痛 | 2.190 | 0.595 | 13.553 | <0.001 | 8.933 | (2.784,28.663) |
| 视物模糊 | 1.990 | 0.589 | 11.424 | 0.001 | 7.314 | (2.307,23.189) |
| 飞蚊症 | 2.702 | 0.777 | 12.105 | 0.001 | 14.909 | (3.254,68.311) |
| 耳聋 | 1.702 | 0.680 | 6.263 | 0.012 | 5.486 | (1.446,20.809) |
| 口干喜饮 | 2.416 | 0.604 | 16.022 | <0.001 | 11.200 | (3.431,36.557) |
| 喜热饮 | -0.934 | 0.675 | 1.913 | 0.167 | 0.393 | (0.105,1.476) |
| 恶心 | 1.535 | 0.663 | 5.369 | 0.020 | 4.643 | (1.267,17.013) |
| 胁肋胀满 | -0.967 | 1.077 | 0.806 | 0.369 | 0.380 | (0.046,3.138) |
| 四肢倦怠 | 1.267 | 0.573 | 4.888 | 0.027 | 3.550 | (1.155,10.914) |
| 肢体关节疼痛 | -0.629 | 0.800 | 0.617 | 0.432 | 0.533 | (0.111,2.559) |
| 泄泻 | 0.758 | 0.883 | 0.737 | 0.391 | 2.133 | (0.378,12.034) |
Table 8 Univariate Logistic regression analysis of TCM indicators associated with malignant hypertension in IgA nephropathy
| 指标 | B | SE | Waldχ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 形寒肢冷 | -0.724 | 0.614 | 1.392 | 0.238 | 0.485 | (0.146,1.614) |
| 肌肤干燥 | -0.836 | 0.795 | 1.106 | 0.293 | 0.433 | (0.091,2.058) |
| 爪甲青紫 | 2.547 | 0.916 | 7.733 | 0.005 | 12.769 | (2.121,76.882) |
| 口唇青紫 | -0.414 | 0.617 | 0.450 | 0.502 | 0.661 | (0.197,2.217 ) |
| 面色晦暗 | -0.773 | 0.613 | 1.590 | 0.207 | 0.462 | (0.139,1.535) |
| 颧红 | 1.037 | 0.764 | 1.842 | 0.175 | 2.821 | (0.631,12.618) |
| 头痛 | 2.190 | 0.595 | 13.553 | <0.001 | 8.933 | (2.784,28.663) |
| 视物模糊 | 1.990 | 0.589 | 11.424 | 0.001 | 7.314 | (2.307,23.189) |
| 飞蚊症 | 2.702 | 0.777 | 12.105 | 0.001 | 14.909 | (3.254,68.311) |
| 耳聋 | 1.702 | 0.680 | 6.263 | 0.012 | 5.486 | (1.446,20.809) |
| 口干喜饮 | 2.416 | 0.604 | 16.022 | <0.001 | 11.200 | (3.431,36.557) |
| 喜热饮 | -0.934 | 0.675 | 1.913 | 0.167 | 0.393 | (0.105,1.476) |
| 恶心 | 1.535 | 0.663 | 5.369 | 0.020 | 4.643 | (1.267,17.013) |
| 胁肋胀满 | -0.967 | 1.077 | 0.806 | 0.369 | 0.380 | (0.046,3.138) |
| 四肢倦怠 | 1.267 | 0.573 | 4.888 | 0.027 | 3.550 | (1.155,10.914) |
| 肢体关节疼痛 | -0.629 | 0.800 | 0.617 | 0.432 | 0.533 | (0.111,2.559) |
| 泄泻 | 0.758 | 0.883 | 0.737 | 0.391 | 2.133 | (0.378,12.034) |
| 指标 | B | SE | Waldχ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 头痛 | 2.066 | 0.801 | 6.658 | 0.010 | 7.895 | (1.643,37.935) |
| 视物模糊 | 1.705 | 0.774 | 4.853 | 0.028 | 5.499 | (1.207,25.053) |
| 口干喜饮 | 2.310 | 0.756 | 9.334 | 0.002 | 10.079 | (2.289,44.373) |
| 爪甲青紫 | 2.908 | 1.086 | 7.167 | 0.007 | 18.312 | (2.179,153.884) |
Table 9 Multivariate Logistic regression analysis of TCM indicators associated with malignant hypertension in IgA nephropathy
| 指标 | B | SE | Waldχ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 头痛 | 2.066 | 0.801 | 6.658 | 0.010 | 7.895 | (1.643,37.935) |
| 视物模糊 | 1.705 | 0.774 | 4.853 | 0.028 | 5.499 | (1.207,25.053) |
| 口干喜饮 | 2.310 | 0.756 | 9.334 | 0.002 | 10.079 | (2.289,44.373) |
| 爪甲青紫 | 2.908 | 1.086 | 7.167 | 0.007 | 18.312 | (2.179,153.884) |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
陈仆,陈香美,谢院生,等. 伴MHTIgA肾病的临床病理特征及其与肾血管病变的相关性[J]. 中华肾脏病杂志,2008,24(6):392-397. DOI:10.3321/j.issn:1001-7097.2008.06.005.
|
| [5] |
|
| [6] |
陈天新,陈波,陈薪薪,等. 伴与不伴原发性肾脏病的MHT肾损害临床病理特点及预后对比分析[J]. 中华高血压杂志,2020,28(9):900. DOI:10.16439/j.cnki.1673-7245.2020.09.030.
|
| [7] | |
| [8] |
|
| [9] |
|
| [10] |
中华急诊医学教育学院,北京市心肺脑复苏重点实验室,首都医科大学附属北京朝阳医院急诊医学临床研究中心,等. 中国高血压急症诊治规范[J]. 中华急诊医学杂志,2020,29(9):1154-1161. DOI:10.3760/cma.j.issn.1671-0282.2020.09.003.
|
| [11] |
|
| [12] |
陈香美,邓跃毅,谢院生. IgA肾病西医诊断和中医辨证分型的实践指南[J]. 中国中西医结合杂志,2013,33(5):583-585.
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
张惠雅,窦艳娜,刘栋,等. 血清IgM水平与IgA肾病疾病严重程度及预后的相关性[J]. 中华肾脏病杂志,2020,36(1):41-44. DOI:10.3760/cma.j.issn.1001-7097.2020.01.007.
|
| [19] |
温碧玉. 血清IgG与IgA肾病不良预后的相关性研究[D]. 太原:山西医科大学,2020.
|
| [20] |
|
| [21] |
徐迎华. 狼疮性肾炎肾小管间质损害相关分析[D]. 天津:天津医科大学,2018.
|
| [22] |
程小红,于小勇,毛加荣. IgA肾病的病理改变与中医微观辨证[J]. 中国中西医结合肾病杂志,2014,15(2):185-186.
|
| [23] | |
| [24] |
占永立,李秀英,李深,等. 17例肾性MHT临床与病理分析[J]. 中国中西医结合肾病杂志,2006,7(2):101-103. DOI:10.3969/j.issn.1009-587X.2006.02.014.
|
| [25] |
陈一峰,方寒蕊,王浩,等. 高血压200例脉象及病机分析[J]. 中国社区医师,2021,37(27):91-92. DOI:10.3969/j.issn.1007-614x.2021.27.045.
|
| [26] | |
| [27] |
廖辉,李丹萍,陈强,等. "泻南补北"法治疗阴虚阳亢型高血压病疗效观察[J]. 中国针灸,2006,26(2):91-93.
|
| [28] |
蔺晓源,杨晓丹,姚福胜,等. 原发性高血压病"本虚标实"的中医病机与治疗[J]. 中医药学报,2018,46(6):10-12. DOI:10.19664/j.cnki.1002-2392.180169.
|
| [29] |
杨晓萍,唐岚,张琪琳,等. 高血压性肾损害的中医症状证型分析[J]. 山东中医药大学学报,2014,38(1):28-30. DOI:10.16294/j.cnki.1007-659x.2014.01.008.
|
| [30] |
焦欣,蔺晓源,雍苏南. 基于名老中医经验的高血压病病名、病因、病机、证型研究[J]. 中医药信息,2020,37(4):31-35. DOI:10.19656/j.cnki.1002-2406.200095.
|
| [1] | BAI Jiaxin, CHEN Yu, ZHOU Yiheng, LIU Lidi, YANG Rong, YAO Yi, YUAN Bo, ZHANG Yonggang, LEI Yi, ZENG Rui, JIA Yu, LIAO Xiaoyang. Assessment and Treatment of Early-onset Hypertension: Position Statement of the British and Irish Hypertension Association and Its Implications for Clinical Management of Early-onset Hypertension in China [J]. Chinese General Practice, 2025, 28(30): 3741-3746. |
| [2] | WU Wenjun, WEI Jingjing, LI Xue, REN Hongjie, YU Rui, PENG Guangcao, ZHU Mingjun. Regularity of Prescriptions for Coronary Heart Disease with Hypertension Based on Latent Structure and Association Rules [J]. Chinese General Practice, 2025, 28(30): 3787-3795. |
| [3] | QIN Bangguo, SUN Jin, LI Man, QIU Jiaojiao, CHENG Bokai, ZHU Ping, WANG Shuxia. Relationship between Non-high-density Lipoprotein Cholesterol to High-density Lipoprotein Cholesterol Ratio and Left Ventricular Hypertrophy in a Community-based Hypertensive Population [J]. Chinese General Practice, 2025, 28(30): 3753-3760. |
| [4] | HU Jieman, TAN Feixiang, YUAN Anxin, CHEN Shiyu, TANG Chulei, YIN Yueheng, BA Lei, XU Qin. Analysis of the Trajectory of Postoperative Frailty and Influencing Factors in Patients with Colorectal Cancer [J]. Chinese General Practice, 2025, 28(26): 3276-3282. |
| [5] | WEI Jiaohua, PENG Huiru, PENG Jianye, TAN Wenting, HUANG Jine, FANG Li. Expression of the Serum MOTS-c and Its Correlation with Atrial Remodeling in Patients with Atrial Fibrillation [J]. Chinese General Practice, 2025, 28(26): 3271-3276. |
| [6] | CHOU Xintong, PENG Hanyu, MA Hui, ZHANG Zhen, SU Xian, QIU Hongyan. Maternal Preferences in Contraceptive Decision-making: an Analysis of Influencing Factors [J]. Chinese General Practice, 2025, 28(26): 3294-3299. |
| [7] | HAN Xiao, LI Qiyu, GE Pu, FAN Siyuan, LIU Diyue, WU Yibo, ZHANG Qingshuang. The Impact of Behavioral Lifestyle on Quality of Life in Hypertensive Patients [J]. Chinese General Practice, 2025, 28(26): 3248-3258. |
| [8] | YU Zizi, LIU Duli, LI Ximin, RUAN Chunyi, YIN Xiangyang, CAI Le. Analysis of the Prevalence and Self-management of Hypertension and Its Influencing Factors in Rural [J]. Chinese General Practice, 2025, 28(25): 3137-3143. |
| [9] | FAN Boyang, ZHANG Yu, SUN Wenning, ZHANG Huifang, WANG Yingjie, ZHANG Ao, ZHAO Yang, WANG Haipeng. Study of Behavioral Intention and Influencing Factors of Integrated Medical and Preventive Care Provided by Grassroots Doctors for Patients with Chronic Diseases [J]. Chinese General Practice, 2025, 28(25): 3144-3150. |
| [10] | TANG Shangfeng, HUANG Yangzhen, PAN Yangyang, ZHENG Yanxi, XIONG Zhongbao, ZHANG Kangkang, SONG Jia, WEI Yilin, WANG Chunying, DONG Heng, CHEN Manwei, QING Hua. Specification for the Integration of Healthcare and Prevention Services in Hypertension at the Primary Level [J]. Chinese General Practice, 2025, 28(25): 3089-3095. |
| [11] | HE Jinyu, ZHULIDUZI Jiesisibieke, ZHANG Ning, LIU Min, LIANG Wannian. Research on Blood Pressure Control and Its Determinants Among Hypertensive Patients Under Standardized Management in China: Status, Challenges, and Future Directions [J]. Chinese General Practice, 2025, 28(24): 2968-2971. |
| [12] | WANG Rupeng, NAN Jing, HU Yiran, YANG Shenghua, JIN Zening. Predictive Value of the Triglyceride-Glucose Body Mass Index for Slow Flow/No-reflow Phenomenon in Patients with Type 2 Diabetes Mellitus and Acute Myocardial Infarction Undergoing Emergency Percutaneous Coronary Intervention [J]. Chinese General Practice, 2025, 28(24): 2985-2992. |
| [13] | WEI Yunhong, YANG Li, WANG Yulu, YE Qiufang, DAI Anni, HE Yan. Study on Cardiopulmonary Function During Different Exercise Stages in Patients with Obesity-related Hypertension [J]. Chinese General Practice, 2025, 28(24): 2972-2978. |
| [14] | WU Yue, WANG Xuetong, KE Bilian. Evaluation of Vision-related Quality of Life in Myopic Macular Degeneration Patients with Low Vision and Associated Factors [J]. Chinese General Practice, 2025, 28(23): 2908-2914. |
| [15] | DING Zijun, ZHOU Nannan, LUO Xing, LUO Jieyu, HAO Wenjuan, ZHANG Chunjiang, JIN Xin, ZHAO Dan. Cognitive Impairment in Patients on Maintenance Hemodialysis and Its Influencing Factors: a Multicenter Cross-sectional Study [J]. Chinese General Practice, 2025, 28(23): 2885-2893. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||