
Chinese General Practice ›› 2022, Vol. 25 ›› Issue (09): 1054-1061.DOI: 10.12114/j.issn.1007-9572.2022.02.022
Special Issue: 内分泌代谢性疾病最新文章合辑
• Article • Previous Articles Next Articles
Reducing the Risk of Adverse Events in Patients with Type 2 Diabetes Who are Poorly Treated with Metformin Combined with Acarbose:Dipeptidyl Peptidase-4 Inhibitor is Better Than Insulin
SU Peng1,LIU Yukun2,LIANG Xiaohua3,LIU Xin3,YU Yaohui1,HUANG Pengfei1,BAI Yuru3,HE Xiaoyan3,SHEN Zhihong3,MA Dong1*
Received:2021-11-22
Revised:2022-01-10
Published:2022-03-20
Online:2022-03-01
通讯作者:
马冬
基金资助:CLC Number:
SU Peng, LIU Yukun, LIANG Xiaohua, LIU Xin, YU Yaohui, HUANG Pengfei, BAI Yuru, HE Xiaoyan, SHEN Zhihong, MA Dong.
Reducing the Risk of Adverse Events in Patients with Type 2 Diabetes Who are Poorly Treated with Metformin Combined with Acarbose:Dipeptidyl Peptidase-4 Inhibitor is Better Than Insulin [J]. Chinese General Practice, 2022, 25(09): 1054-1061.
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2022.02.022
| 项目 | 倾向性评分匹配前 | 倾向性评分匹配后 | 标准化差异值 | |||||
|---|---|---|---|---|---|---|---|---|
| Met+Aca+Ins组(n=1 089) | Met+Aca+DPP-4i组(n=481) | Met+Aca+Ins组(n=434) | Met+Aca+DPP-4i组(n=434) | 倾向性评分匹配前 | 倾向性评分匹配后 | 加权后 | ||
| 性别〔n(%)〕 | ||||||||
| 男 | 633(58.13) | 287(59.67) | 252(58.06) | 254(58.53) | 0.031 | 0.009 | 0.012 | |
| 女 | 456(41.87) | 194(40.33) | 182(41.93) | 180(41.47) | 0.031 | 0.009 | 0.012 | |
年龄( ±s,岁) ±s,岁) | 60.6±12.8 | 61.2±11.2 | 61.6±11.4 | 61.3±11.1 | 0.057 | 0.032 | 0.020 | |
| 年龄〔n(%)〕 | ||||||||
| 18~45岁 | 120(11.02) | 21(4.37) | 19(4.38) | 20(4.61) | 0.252 | 0.011 | 0.003 | |
| 46~64岁 | 372(34.16) | 194(40.33) | 165(38.02) | 172(39.63) | 0.128 | 0.033 | 0.001 | |
| ≥65岁 | 597(54.82) | 266(55.30) | 250(57.60) | 242(55.76) | 0.010 | 0.037 | 0.001 | |
身高( ±s,m) ±s,m) | 1.67±0.08 | 1.67±0.08 | 1.67±0.08 | 1.67±0.08 | 0.060 | 0.007 | 0.018 | |
体质量( ±s,kg) ±s,kg) | 73.2±10.6 | 71.8±11.4 | 72.2±10.7 | 71.8±11.3 | 0.123 | 0.026 | 0.020 | |
BMI( ±s,kg/m2) ±s,kg/m2) | 26.2±3.2 | 25.6±3.1 | 25.7±3.1 | 25.6±3.1 | 0.198 | 0.032 | 0.032 | |
| BMI〔n(%)〕 | ||||||||
| 18.5~<24.0 kg/m2 | 222(20.39) | 139(28.90) | 118(27.19) | 119(27.42) | 0.199 | 0.005 | 0.010 | |
| 24.0~<28.0 kg/m2 | 582(53.44) | 242(50.31) | 222(51.15) | 224(51.61) | 0.063 | 0.009 | 0.012 | |
| ≥28.0 kg/m2 | 285(26.17) | 100(20.79) | 94(21.66) | 91(20.97) | 0.127 | 0.017 | 0.024 | |
收缩压( ±s,mm Hg) ±s,mm Hg) | 134±18 | 133±17 | 134±18 | 133±17 | 0.067 | 0.040 | 0.022 | |
舒张压( ±s,mm Hg) ±s,mm Hg) | 80±11 | 80±10 | 80±10 | 80±10 | 0.025 | 0.005 | 0.024 | |
总胆固醇( ±s,mmol/L) ±s,mmol/L) | 4.75±1.23 | 4.72±1.21 | 4.75±1.23 | 4.75±1.23 | 0.025 | 0.004 | 0.007 | |
高密度脂蛋白( ±s,mmol/L) ±s,mmol/L) | 1.18±0.29 | 1.20±0.28 | 1.20±0.30 | 1.19±0.28 | 0.042 | 0.024 | 0.014 | |
低密度脂蛋白( ±s,mmol/L) ±s,mmol/L) | 2.68±0.89 | 2.60±0.85 | 2.66±0.83 | 2.62±0.86 | 0.100 | 0.048 | 0.019 | |
载脂蛋白A1( ±s,mmol/L) ±s,mmol/L) | 1.15±0.61 | 1.15±0.30 | 1.15±0.29 | 1.15±0.30 | 0.013 | 0.004 | 0.013 | |
载脂蛋白B( ±s,mmol/L) ±s,mmol/L) | 0.81±0.40 | 0.80±0.33 | 0.81±0.36 | 0.80±0.34 | 0.031 | 0.014 | 0.004 | |
尿素氮( ±s,mmol/L) ±s,mmol/L) | 5.40±1.69 | 5.44±1.87 | 5.49±1.80 | 5.42±1.66 | 0.022 | 0.039 | 0.006 | |
尿酸( ±s,μmol/L) ±s,μmol/L) | 283.23±89.12 | 287.56±91.65 | 289.09±91.29 | 284.61±89.85 | 0.048 | 0.049 | 0.002 | |
血清白蛋白( ±s,g/L) ±s,g/L) | 41.67±4.72 | 42.27±4.60 | 42.27±4.25 | 42.08±4.62 | 0.130 | 0.042 | 0.028 | |
血清免疫球蛋白( ±s,g/L) ±s,g/L) | 26.47±4.77 | 26.27±4.82 | 26.35±4.63 | 26.30±4.87 | 0.042 | 0.010 | 0.001 | |
内生肌酐清除率( ±s,ml/min) ±s,ml/min) | 93.99±31.52 | 94.74±33.81 | 93.47±31.00 | 92.49±27.57 | 0.023 | 0.033 | 0.021 | |
糖化血红蛋白( ±s,%) ±s,%) | 9.46±2.01 | 8.89±1.91 | 9.03±1.84 | 9.05±1.90 | 0.291 | 0.006 | 0.020 | |
糖尿病病程( ±s,年) ±s,年) | 9.82±7.25 | 9.50±7.10 | 9.58±7.21 | 9.74±7.25 | 0.045 | 0.021 | 0.020 | |
| 糖尿病病程〔n(%)〕 | ||||||||
| ≤5年 | 376(34.53) | 158(32.85) | 149(34.33) | 138(31.80) | 0.036 | 0.054 | 0.012 | |
| >5~≤10年 | 306(28.10) | 162(33.68) | 138(31.80) | 142(32.72) | 0.121 | 0.020 | 0.015 | |
| >10年 | 407(37.37) | 161(33.47) | 147(33.87) | 154(35.48) | 0.082 | 0.034 | 0.026 | |
睡眠时间( ±s,h) ±s,h) | 6.81±1.21 | 7.07±2.79 | 6.98±1.18 | 7.05±2.93 | 0.123 | 0.031 | 0.002 | |
| 睡眠时间〔n(%)〕 | ||||||||
| <7 h/d | 455(41.78) | 136(28.27) | 140(32.26) | 134(30.88) | 0.286 | 0.030 | 0.007 | |
| ≥7 h/d | 634(58.22) | 345(71.73) | 294(67.74) | 300(69.12) | 0.286 | 0.030 | 0.007 | |
| 吸烟〔n(%)〕 | 264(24.24) | 98(20.37) | 345(79.50) | 341(78.57) | 0.093 | 0.023 | 0.028 | |
| 药物使用情况〔n(%)〕 | ||||||||
| 仅使用降压药 | 606(55.65) | 345(71.73) | 258(59.45) | 252(58.06) | 0.052 | 0.028 | 0.012 | |
| 仅使用降脂药 | 324(29.75) | 142(29.52) | 132(30.41) | 123(28.34) | 0.005 | 0.046 | 0.015 | |
| 同时使用降压、降脂药 | 408(37.47) | 192(39.92) | 178(41.01) | 165(38.02) | 0.050 | 0.061 | 0.034 | |
| 合并症 | ||||||||
| 高脂血症〔n(%)〕 | 217(19.93) | 80(16.63) | 70(16.13) | 79(18.20) | 0.085 | 0.055 | 0.020 | |
| 冠心病〔n(%)〕 | 364(33.43) | 157(32.64) | 145(33.41) | 147(33.87) | 0.017 | 0.010 | 0.002 | |
| 下肢动脉硬化栓塞〔n(%)〕 | 40(3.67) | 14(2.91) | 15(3.46) | 13(3.00) | 0.043 | 0.026 | 0.022 | |
| 低蛋白血症〔n(%)〕 | 6(0.55) | 5(1.04) | 2(0.46) | 4(0.92) | 0.055 | 0.056 | 0.006 | |
| 心力衰竭〔n(%)〕 | 3(0.28) | 1(0.21) | 1(0.23) | 1(0.23) | 0.014 | <0.001 | 0.026 | |
| 心血管疾病家族史〔n(%)〕 | 64(5.88) | 30(6.24) | 23(5.30) | 27(6.22) | 0.015 | 0.040 | 0.003 | |
Table 1 Comparison of clinical data of patients in two groups before and after PSM
| 项目 | 倾向性评分匹配前 | 倾向性评分匹配后 | 标准化差异值 | |||||
|---|---|---|---|---|---|---|---|---|
| Met+Aca+Ins组(n=1 089) | Met+Aca+DPP-4i组(n=481) | Met+Aca+Ins组(n=434) | Met+Aca+DPP-4i组(n=434) | 倾向性评分匹配前 | 倾向性评分匹配后 | 加权后 | ||
| 性别〔n(%)〕 | ||||||||
| 男 | 633(58.13) | 287(59.67) | 252(58.06) | 254(58.53) | 0.031 | 0.009 | 0.012 | |
| 女 | 456(41.87) | 194(40.33) | 182(41.93) | 180(41.47) | 0.031 | 0.009 | 0.012 | |
| 年龄(±s,岁) | 60.6±12.8 | 61.2±11.2 | 61.6±11.4 | 61.3±11.1 | 0.057 | 0.032 | 0.020 | |
| 年龄〔n(%)〕 | ||||||||
| 18~45岁 | 120(11.02) | 21(4.37) | 19(4.38) | 20(4.61) | 0.252 | 0.011 | 0.003 | |
| 46~64岁 | 372(34.16) | 194(40.33) | 165(38.02) | 172(39.63) | 0.128 | 0.033 | 0.001 | |
| ≥65岁 | 597(54.82) | 266(55.30) | 250(57.60) | 242(55.76) | 0.010 | 0.037 | 0.001 | |
| 身高(±s,m) | 1.67±0.08 | 1.67±0.08 | 1.67±0.08 | 1.67±0.08 | 0.060 | 0.007 | 0.018 | |
| 体质量(±s,kg) | 73.2±10.6 | 71.8±11.4 | 72.2±10.7 | 71.8±11.3 | 0.123 | 0.026 | 0.020 | |
| BMI(±s,kg/m2) | 26.2±3.2 | 25.6±3.1 | 25.7±3.1 | 25.6±3.1 | 0.198 | 0.032 | 0.032 | |
| BMI〔n(%)〕 | ||||||||
| 18.5~<24.0 kg/m2 | 222(20.39) | 139(28.90) | 118(27.19) | 119(27.42) | 0.199 | 0.005 | 0.010 | |
| 24.0~<28.0 kg/m2 | 582(53.44) | 242(50.31) | 222(51.15) | 224(51.61) | 0.063 | 0.009 | 0.012 | |
| ≥28.0 kg/m2 | 285(26.17) | 100(20.79) | 94(21.66) | 91(20.97) | 0.127 | 0.017 | 0.024 | |
| 收缩压(±s,mm Hg) | 134±18 | 133±17 | 134±18 | 133±17 | 0.067 | 0.040 | 0.022 | |
| 舒张压(±s,mm Hg) | 80±11 | 80±10 | 80±10 | 80±10 | 0.025 | 0.005 | 0.024 | |
| 总胆固醇(±s,mmol/L) | 4.75±1.23 | 4.72±1.21 | 4.75±1.23 | 4.75±1.23 | 0.025 | 0.004 | 0.007 | |
| 高密度脂蛋白(±s,mmol/L) | 1.18±0.29 | 1.20±0.28 | 1.20±0.30 | 1.19±0.28 | 0.042 | 0.024 | 0.014 | |
| 低密度脂蛋白(±s,mmol/L) | 2.68±0.89 | 2.60±0.85 | 2.66±0.83 | 2.62±0.86 | 0.100 | 0.048 | 0.019 | |
| 载脂蛋白A1(±s,mmol/L) | 1.15±0.61 | 1.15±0.30 | 1.15±0.29 | 1.15±0.30 | 0.013 | 0.004 | 0.013 | |
| 载脂蛋白B(±s,mmol/L) | 0.81±0.40 | 0.80±0.33 | 0.81±0.36 | 0.80±0.34 | 0.031 | 0.014 | 0.004 | |
| 尿素氮(±s,mmol/L) | 5.40±1.69 | 5.44±1.87 | 5.49±1.80 | 5.42±1.66 | 0.022 | 0.039 | 0.006 | |
| 尿酸(±s,μmol/L) | 283.23±89.12 | 287.56±91.65 | 289.09±91.29 | 284.61±89.85 | 0.048 | 0.049 | 0.002 | |
| 血清白蛋白(±s,g/L) | 41.67±4.72 | 42.27±4.60 | 42.27±4.25 | 42.08±4.62 | 0.130 | 0.042 | 0.028 | |
| 血清免疫球蛋白(±s,g/L) | 26.47±4.77 | 26.27±4.82 | 26.35±4.63 | 26.30±4.87 | 0.042 | 0.010 | 0.001 | |
| 内生肌酐清除率(±s,ml/min) | 93.99±31.52 | 94.74±33.81 | 93.47±31.00 | 92.49±27.57 | 0.023 | 0.033 | 0.021 | |
| 糖化血红蛋白(±s,%) | 9.46±2.01 | 8.89±1.91 | 9.03±1.84 | 9.05±1.90 | 0.291 | 0.006 | 0.020 | |
| 糖尿病病程(±s,年) | 9.82±7.25 | 9.50±7.10 | 9.58±7.21 | 9.74±7.25 | 0.045 | 0.021 | 0.020 | |
| 糖尿病病程〔n(%)〕 | ||||||||
| ≤5年 | 376(34.53) | 158(32.85) | 149(34.33) | 138(31.80) | 0.036 | 0.054 | 0.012 | |
| >5~≤10年 | 306(28.10) | 162(33.68) | 138(31.80) | 142(32.72) | 0.121 | 0.020 | 0.015 | |
| >10年 | 407(37.37) | 161(33.47) | 147(33.87) | 154(35.48) | 0.082 | 0.034 | 0.026 | |
| 睡眠时间(±s,h) | 6.81±1.21 | 7.07±2.79 | 6.98±1.18 | 7.05±2.93 | 0.123 | 0.031 | 0.002 | |
| 睡眠时间〔n(%)〕 | ||||||||
| <7 h/d | 455(41.78) | 136(28.27) | 140(32.26) | 134(30.88) | 0.286 | 0.030 | 0.007 | |
| ≥7 h/d | 634(58.22) | 345(71.73) | 294(67.74) | 300(69.12) | 0.286 | 0.030 | 0.007 | |
| 吸烟〔n(%)〕 | 264(24.24) | 98(20.37) | 345(79.50) | 341(78.57) | 0.093 | 0.023 | 0.028 | |
| 药物使用情况〔n(%)〕 | ||||||||
| 仅使用降压药 | 606(55.65) | 345(71.73) | 258(59.45) | 252(58.06) | 0.052 | 0.028 | 0.012 | |
| 仅使用降脂药 | 324(29.75) | 142(29.52) | 132(30.41) | 123(28.34) | 0.005 | 0.046 | 0.015 | |
| 同时使用降压、降脂药 | 408(37.47) | 192(39.92) | 178(41.01) | 165(38.02) | 0.050 | 0.061 | 0.034 | |
| 合并症 | ||||||||
| 高脂血症〔n(%)〕 | 217(19.93) | 80(16.63) | 70(16.13) | 79(18.20) | 0.085 | 0.055 | 0.020 | |
| 冠心病〔n(%)〕 | 364(33.43) | 157(32.64) | 145(33.41) | 147(33.87) | 0.017 | 0.010 | 0.002 | |
| 下肢动脉硬化栓塞〔n(%)〕 | 40(3.67) | 14(2.91) | 15(3.46) | 13(3.00) | 0.043 | 0.026 | 0.022 | |
| 低蛋白血症〔n(%)〕 | 6(0.55) | 5(1.04) | 2(0.46) | 4(0.92) | 0.055 | 0.056 | 0.006 | |
| 心力衰竭〔n(%)〕 | 3(0.28) | 1(0.21) | 1(0.23) | 1(0.23) | 0.014 | <0.001 | 0.026 | |
| 心血管疾病家族史〔n(%)〕 | 64(5.88) | 30(6.24) | 23(5.30) | 27(6.22) | 0.015 | 0.040 | 0.003 | |
| 终点事件 | 倾向性评分匹配前 | 倾向性评分匹配后 | |||
|---|---|---|---|---|---|
| Met+Aca+Ins组(n=1 089) | Met+Aca+DPP-4i组(n=481) | Met+Aca+Ins组(n=434) | Met+Aca+DPP-4i组(n=434) | ||
| 综合结局事件 | |||||
| 发生人数(人) | 233 | 35 | 96 | 35 | |
| 总生存时间(年) | 1 266.34 | 584.38 | 501.46 | 536.00 | |
| 中位随访时间(年) | 1.030 | 1.140 | 1.030 | 1.170 | |
| 发病密度(/100人年) | 18.40 | 5.99 | 19.14 | 6.53 | |
| 复合非致命性心血管疾病 | |||||
| 发生人数(人) | 147 | 27 | 54 | 27 | |
| 总生存时间(年) | 1 323.60 | 584.90 | 521.69 | 536.52 | |
| 中位随访时间(年) | 1.120 | 1.140 | 1.120 | 1.170 | |
| 发病密度(/100人年) | 11.11 | 4.62 | 10.35 | 5.03 | |
| 全因死亡 | |||||
| 发生人数(人) | 33 | 4 | 22 | 4 | |
| 总生存时间(年) | 1 478.8 | 595.36 | 580.99 | 546.98 | |
| 中位随访时间(年) | 1.310 | 1.140 | 1.250 | 1.200 | |
| 发病密度(/100人年) | 2.23 | 0.67 | 3.79 | 0.73 | |
| 严重低血糖事件 | |||||
| 发生人数(人) | 53 | 4 | 20 | 4 | |
| 总生存时间(年) | 1 421.6 | 594.84 | 560.76 | 546.46 | |
| 中位随访时间(年) | 1.250 | 1.140 | 1.295 | 1.200 | |
| 发病密度(/100人年) | 3.73 | 0.67 | 3.57 | 0.73 | |
Table 2 Outcome events,overall survival,median follow-up and incidence density of patients in two groups before and after PSM
| 终点事件 | 倾向性评分匹配前 | 倾向性评分匹配后 | |||
|---|---|---|---|---|---|
| Met+Aca+Ins组(n=1 089) | Met+Aca+DPP-4i组(n=481) | Met+Aca+Ins组(n=434) | Met+Aca+DPP-4i组(n=434) | ||
| 综合结局事件 | |||||
| 发生人数(人) | 233 | 35 | 96 | 35 | |
| 总生存时间(年) | 1 266.34 | 584.38 | 501.46 | 536.00 | |
| 中位随访时间(年) | 1.030 | 1.140 | 1.030 | 1.170 | |
| 发病密度(/100人年) | 18.40 | 5.99 | 19.14 | 6.53 | |
| 复合非致命性心血管疾病 | |||||
| 发生人数(人) | 147 | 27 | 54 | 27 | |
| 总生存时间(年) | 1 323.60 | 584.90 | 521.69 | 536.52 | |
| 中位随访时间(年) | 1.120 | 1.140 | 1.120 | 1.170 | |
| 发病密度(/100人年) | 11.11 | 4.62 | 10.35 | 5.03 | |
| 全因死亡 | |||||
| 发生人数(人) | 33 | 4 | 22 | 4 | |
| 总生存时间(年) | 1 478.8 | 595.36 | 580.99 | 546.98 | |
| 中位随访时间(年) | 1.310 | 1.140 | 1.250 | 1.200 | |
| 发病密度(/100人年) | 2.23 | 0.67 | 3.79 | 0.73 | |
| 严重低血糖事件 | |||||
| 发生人数(人) | 53 | 4 | 20 | 4 | |
| 总生存时间(年) | 1 421.6 | 594.84 | 560.76 | 546.46 | |
| 中位随访时间(年) | 1.250 | 1.140 | 1.295 | 1.200 | |
| 发病密度(/100人年) | 3.73 | 0.67 | 3.57 | 0.73 | |
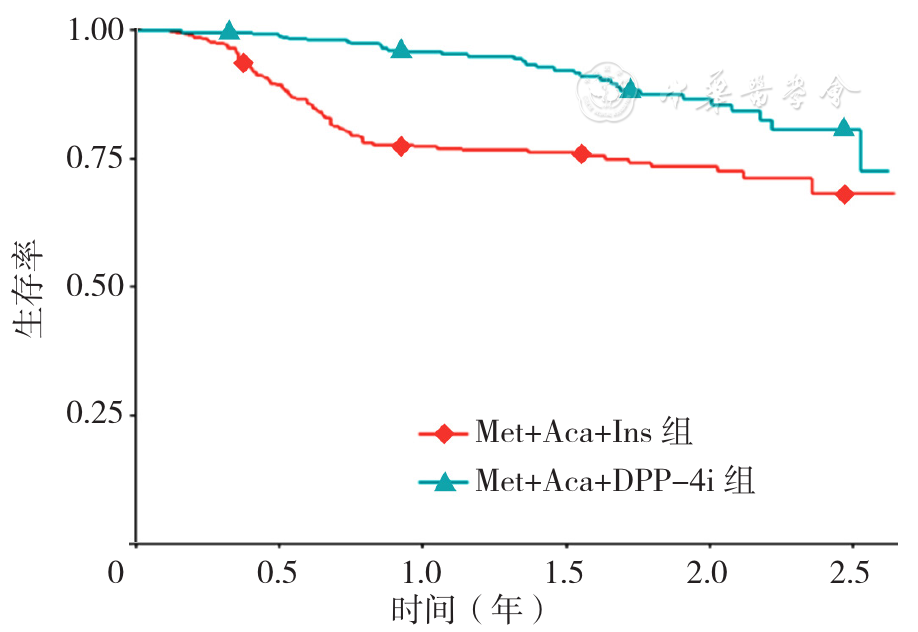
Figure 1 Survival curves of two groups of patients after PSM
| [1] | MINGRONE G,PANUNZI S,DE GAETANO A,et al. Metabolic surgery versus conventional medical therapy in patients with type 2 diabetes:10-year follow-up of an open-label,single-centre,randomised controlled trial[J]. Lancet,2021,397(10271):293-304. DOI:10.1016/S0140-6736(20)32649-0. |
| [2] | FU L Y,ZHOU Y,SUN J X,et al. Atherogenic index of plasma is associated with major adverse cardiovascular events in patients with type 2 diabetes mellitus[J]. Cardiovasc Diabetol,2021,20(1):201. DOI:10.1186/s12933-021-01393-5. |
| [3] | INZUCCHI S E,BERGENSTAL R M,BUSE J B,et al. Management of hyperglycemia in type 2 diabetes,2015:a patient-centered approach:update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes[J]. Diabetes Care,2015,38(1):140-149. DOI:10.2337/dc14-2441. |
| [4] | 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华糖尿病杂志,2021,13(4):315-409. DOI:10.3760/cma.j.cn115791-20210221-00095. |
| [5] | WORKGROUP ON HYPOGLYCEMIA A D A. Defining and reporting hypoglycemia in diabetes:a report from the American Diabetes Association Workgroup on Hypoglycemia[J]. Diabetes Care,2005,28(5):1245-1249. DOI:10.2337/diacare.28.5.1245. |
| [6] | AUSTIN P C. The use of propensity score methods with survival or time-to-event outcomes:reporting measures of effect similar to those used in randomized experiments[J]. Stat Med,2014,33(7):1242-1258. DOI:10.1002/sim.5984. |
| [7] | HAVILAND A,NAGIN D S,ROSENBAUM P R. Combining propensity score matching and group-based trajectory analysis in an observational study[J]. Psychol Methods,2007,12(3):247-267. DOI:10.1037/1082-989X.12.3.247. |
| [8] | LIU Z J,ZHAO X D,SUN W W,et al. Metformin combined with acarbose vs. single medicine in the treatment of type 2 diabetes:a meta-analysis[J]. Exp Ther Med,2017,13(6):3137-3145. DOI:10.3892/etm.2017.4333. |
| [9] | HOLLANDER P,SUGIMOTO D,VLAJNIC A,et al. Combination therapy with insulin glargine plus metformin but not insulin glargine plus sulfonylurea provides similar glycemic control to triple oral combination therapy in patients with type 2 diabetes uncontrolled with dual oral agent therapy[J]. J Diabetes Complications,2015,29(8):1266-1271. DOI:10.1016/j.jdiacomp.2015.05.022. |
| [10] | MARÍN-PEÑALVER J J,MARTÍN-TIMÓN I,DEL CAÑIZO-GÓMEZ F J. Management of hospitalized type 2 diabetes mellitus patients[J]. J Transl Int Med,2016,4(4):155-161. DOI:10.1515/jtim-2016-0027. |
| [11] | HOME P,ITZHAK B. Is insulin therapy safe? [J]. Am J Ther,2020,27(1):e106-114. DOI:10.1097/mjt.0000000000001077. |
| [12] | HOLLANDER P,SUGIMOTO D,VLAJNIC A,et al. Combination therapy with insulin glargine plus metformin but not insulin glargine plus sulfonylurea provides similar glycemic control to triple oral combination therapy in patients with type 2 diabetes uncontrolled with dual oral agent therapy[J]. J Diabetes Complications,2015,29(8):1266-1271. DOI:10.1016/j.jdiacomp.2015.05.022. |
| [13] | HERMAN M E,O'KEEFE J H,BELL D S H,et al. Insulin therapy increases cardiovascular risk in type 2 diabetes[J]. Prog Cardiovasc Dis,2017,60(3):422-434. DOI:10.1016/j.pcad.2017.09.001. |
| [14] | LIU D,JIN B,CHEN W,et al. Dipeptidyl peptidase 4 (DPP-4) inhibitors and cardiovascular outcomes in patients with type 2 diabetes mellitus (T2DM):a systematic review and meta-analysis[J]. BMC Pharmacol Toxicol,2019,20(1):15. DOI:10.1186/s40360-019-0293-y. |
| [15] | ZENG D K,XIAO Q,LI F Q,et al. Cardiovascular risk of sitagliptin in treating patients with type 2 diabetes mellitus[J]. Biosci Rep,2019,39(7):BSR20190980. DOI:10.1042/BSR20190980. |
| [16] | CONSENSUS CONFERENCE PANEL,WATSON N F,BADR M S,et al. Joint consensus statement of the American academy of sleep medicine and sleep research society on the recommended amount of sleep for a healthy adult:methodology and discussion[J]. J Clin Sleep Med,2015,11(8):931-952. DOI:10.5664/jcsm.4950. |
| [17] | KNUTSON K L,VAN CAUTER E. Associations between sleep loss and increased risk of obesity and diabetes[J]. Ann N Y Acad Sci,2008,1129:287-304. DOI:10.1196/annals.1417.033. |
| [18] | SPIEGEL K,LEPROULT R,VAN CAUTER E. Impact of sleep debt on metabolic and endocrine function[J]. Lancet,1999,354(9188):1435-1439. DOI:10.1016/S0140-6736(99)01376-8. |
| [19] | SPIEGEL K,TASALI E,PENEV P,et al. Brief communication:sleep curtailment in healthy young men is associated with decreased leptin levels,elevated ghrelin levels,and increased hunger and appetite[J]. Ann Intern Med,2004,141(11):846-850. DOI:10.7326/0003-4819-141-11-200412070-00008. |
| [20] | JHA P,RAMASUNDARAHETTIGE C,LANDSMAN V,et al. 21st-century hazards of smoking and benefits of cessation in the United States[J]. N Engl J Med,2013,368(4):341-350. DOI:10.1056/NEJMsa1211128. |
| [21] | DUNCAN M S,FREIBERG M S,GREEVY R A Jr,et al. Association of smoking cessation with subsequent risk of cardiovascular disease[J]. JAMA,2019,322(7):642-650. DOI:10.1001/jama.2019.10298. |
| [22] | CHAMBERLAIN J J,JOHNSON E L,LEAL S,et al. Cardiovascular disease and risk management:review of the American diabetes association standards of medical care in diabetes 2018[J]. Ann Intern Med,2018,168(9):640-650. DOI:10.7326/M18-0222. |
| [23] | AL-DELAIMY W K,MANSON J E,SOLOMON C G,et al. Smoking and risk of coronary heart disease among women with type 2 diabetes mellitus[J]. Arch Intern Med,2002,162(3):273-279. DOI:10.1001/archinte.162.3.273. |
| [1] | QIU Yanli, GAO Yongyin, BIAN Xueyan, WANG Xue, LI Yue. The Predictive Value of Estimated Pulse Wave Velocity for All-cause and Cardiovascular-related Mortality in Cancer Patients [J]. Chinese General Practice, 2026, 29(14): 1890-1897. |
| [2] | LIU Dianchun, CHEN Xiaoying, WANG Qianyun, PAN Xingru, WEI Xuehan, WANG Bohong, WANG Ying, XUE Xue, LU Chunli. Evidence-based Pharmacological Investigation of the Clinical Practice and Rational Use of Metformin in Pre-diabetes Mellitus [J]. Chinese General Practice, 2026, 29(08): 1057-1068. |
| [3] | ZHONG Lanfang, YU Xinyu, PI Zheyu, LI Bin. Drug-induced Cardiotoxicity in the Chinese Population: Current Analysis and Considerations [J]. Chinese General Practice, 2026, 29(06): 767-776. |
| [4] | ZHU Chenrui, LI Na, WU Yuntao, ZHAO Haiyan, HUANG Zhe, LIU Yan, JI Chunpeng, WU Shouling. The Impact of Serum Uric Acid Levels on New-onset Atrioventricular Block: a Prospective Cohort Study [J]. Chinese General Practice, 2026, 29(05): 583-590. |
| [5] | ZENG Minghui, KUAI Wentao, CHEN Lin, HAN Jiaxin, XU Lianxin, GE Liying, DAI Rongrong, MI Yuqiang, XU Liang. Effect of Type 2 Diabetes Mellitus on the Efficacy of Nucleoside (Acid) Analogues in the Treatment of Chronic Hepatitis B [J]. Chinese General Practice, 2025, 28(35): 4414-4420. |
| [6] | DENG Jie, QI Qi, WU Xinyu, HAN Quanle, LI Lei, JIANG Yue, YU Jing, WU Ruojie, WU Shouling, LI Kangbo. Cohort Study on the Association between the Atherogenic Index of Plasma and the Risk of Incident Heart Failure in a Physical Examination Population [J]. Chinese General Practice, 2025, 28(29): 3645-3652. |
| [7] | SU Qing, XU Yao, LI Yihang, WANG Liyan, CAI Yefeng, NI Xiaojia. Quality Evaluation of Methodology on the Changes in Traditional Chinese Medicine Syndromes of Stroke and Risk Population [J]. Chinese General Practice, 2025, 28(29): 3694-3702. |
| [8] | DING Xiang, LIU Jian, CHEN Xiaolu, ZHANG Xianheng. Chinese Herbal Medicine may be Associated with Lower Readmissions in Rheumatoid Arthritis Patients with Streptococcal Infection: a Matched Cohort Study [J]. Chinese General Practice, 2025, 28(24): 3005-3012. |
| [9] | YANG Ji, ZHANG Yao, ZHAO Yingqiang, ZHANG Qiuyue. Evaluation of the Effectiveness of TCM Three-level Prevention and Control Model in the Management of Patients with Coronary Heart Disease and Stroke: a Single-center, Prospective Cohort Study [J]. Chinese General Practice, 2025, 28(22): 2750-2761. |
| [10] | CHEN Qiaoqiao, SU Ping, ZHAO Yingying, PANG Jinhong, SHI Jie, WANG Yaqian, LI Qiuchun, HE Ruiyan, WANG Yue, CHEN Xueyu, QIAO Junpeng, CHI Weiwei. Association between Triglyceride-Glucose Index and Incident Cardiometabolic Multimorbidity in the Elderly: a Prospective Cohort Study [J]. Chinese General Practice, 2025, 28(18): 2270-2277. |
| [11] | LI Dongxing, NIU Zimin, WANG Haoxiang. A Retrospective Cohort Study on Health Examination of Elderly Population in Huangpu District, Guangzhou [J]. Chinese General Practice, 2025, 28(13): 1635-1641. |
| [12] | WANG Jiangtao, DU Yu, ZHU Ling, ZHAO Fouxi, HU Yuandong, LIU Tao. Correlation between Lipid Accumulation Product and the Incidence of Hypertension in Adults: a Prospective Cohort Study [J]. Chinese General Practice, 2025, 28(12): 1433-1438. |
| [13] | WANG Dexiang, YUAN Jiawen, LU Qinyun, HANG Yuhao, LU Jun, CHENG Lu. Influences of Treatment Timing of the TCM prescription Qingfei Huayu Tongfu Formula on the Therapeutic Effect and Prognosis of Sepsis-related Acute Respiratory Distress Syndrome [J]. Chinese General Practice, 2025, 28(12): 1500-1505. |
| [14] | LOU Xianzhe, MIAO Tongguo, ZHANG Shiya, MA Dong, NAN Yuemin. The Impact of the Monocyte-to-High-Density Lipoprotein Cholesterol Ratio on the Prognosis of Patients with Non-Viral, Non-Alcoholic Hepatocellular Carcinoma: a Retrospective Cohort Study [J]. Chinese General Practice, 2025, 28(09): 1092-1099. |
| [15] | TIAN Ke, LENG Qiufeng, LYU Jing, MIAO Guoying, WANG Xinhui, XIE Hui, LIU Qu, YAO Chunxia. Bidirectional Regulation of Keratinocyte Proliferation and Apoptosis by Metformin via NLRP3 Inflammasome Pathway [J]. Chinese General Practice, 2025, 28(06): 742-750. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||