
Chinese General Practice ›› 2025, Vol. 28 ›› Issue (11): 1376-1382.DOI: 10.12114/j.issn.1007-9572.2024.0158
Special Issue: 儿科最新文章合辑; 肾脏疾病最新文章合辑
• Original Research·Combination of Chinese and Western Medicine • Previous Articles Next Articles
Received:2024-04-09
Revised:2024-09-27
Published:2025-04-15
Online:2025-02-06
Contact:
XIA Zhengkun
通讯作者:
夏正坤
作者简介:作者贡献:
张沛负责研究设计和文章撰写;杨萌负责文章撰写和数据统计;高春林负责数据分析;夏正坤负责文章审校,对文章整体负责。
基金资助:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2024.0158
| 项目 | 治疗组(n=65) | 对照组(n=71) | 检验统计量值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 42/23 | 39/32 | 1.322 | 0.250 |
| 年龄(岁) | 13.6±4.3 | 12.1±4.7 | 0.685a | 0.604 |
| AKI分期[例(%)] | ||||
| 1期 | 20(30.8) | 18(25.4) | 0.495 | 0.482 |
| 2期 | 21(32.3) | 25(35.2) | 0.128 | 0.721 |
| 3期 | 24(36.9) | 28(39.4) | 0.091 | 0.763 |
| Scr[M(P25,P75),μmol/L] | 113.52(34.76,131.57) | 182.05(40.21,146.65) | -3.013b | 0.002 |
| BUN[M(P25,P75),mmol/L] | 9.69(6.89,17.35) | 12.47(7.45,20.53) | -2.285b | 0.018 |
| UA(μmol/L) | 413.25±92.74 | 488.46±110.16 | 1.296a | 0.023 |
| eGFR[mL·min-1·(1.73 m2)-1] | 84.25±18.14 | 68.67±15.75 | 2.881a | 0.004 |
| 尿NAG酶(U·g-1·Cr-1) | 18.24±3.37 | 24.53±4.62 | 2.854a | 0.006 |
| 尿RBP(mg/L) | 1.35±0.34 | 1.87±0.38 | 3.425a | <0.001 |
| 尿NGAL(μg/L) | 76.46±22.45 | 94.28±24.66 | 3.182a | 0.002 |
| 中医证候评分(分) | 7.78±2.13 | 10.49±2.56 | 2.876a | 0.005 |
| AKI完全恢复[例(%)] | 39(60.0) | 30(42.3) | 4.276 | 0.039 |
| CKD 3期[例(%)] | 7(10.8) | 19(26.8) | 5.612 | 0.018 |
| ESRD[例(%)] | 5(7.7) | 9(12.7) | 0.913 | 0.339 |
Table 1 General information and laboratory test results of children in the treatment group and the control group after treatment
| 项目 | 治疗组(n=65) | 对照组(n=71) | 检验统计量值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 42/23 | 39/32 | 1.322 | 0.250 |
| 年龄(岁) | 13.6±4.3 | 12.1±4.7 | 0.685a | 0.604 |
| AKI分期[例(%)] | ||||
| 1期 | 20(30.8) | 18(25.4) | 0.495 | 0.482 |
| 2期 | 21(32.3) | 25(35.2) | 0.128 | 0.721 |
| 3期 | 24(36.9) | 28(39.4) | 0.091 | 0.763 |
| Scr[M(P25,P75),μmol/L] | 113.52(34.76,131.57) | 182.05(40.21,146.65) | -3.013b | 0.002 |
| BUN[M(P25,P75),mmol/L] | 9.69(6.89,17.35) | 12.47(7.45,20.53) | -2.285b | 0.018 |
| UA(μmol/L) | 413.25±92.74 | 488.46±110.16 | 1.296a | 0.023 |
| eGFR[mL·min-1·(1.73 m2)-1] | 84.25±18.14 | 68.67±15.75 | 2.881a | 0.004 |
| 尿NAG酶(U·g-1·Cr-1) | 18.24±3.37 | 24.53±4.62 | 2.854a | 0.006 |
| 尿RBP(mg/L) | 1.35±0.34 | 1.87±0.38 | 3.425a | <0.001 |
| 尿NGAL(μg/L) | 76.46±22.45 | 94.28±24.66 | 3.182a | 0.002 |
| 中医证候评分(分) | 7.78±2.13 | 10.49±2.56 | 2.876a | 0.005 |
| AKI完全恢复[例(%)] | 39(60.0) | 30(42.3) | 4.276 | 0.039 |
| CKD 3期[例(%)] | 7(10.8) | 19(26.8) | 5.612 | 0.018 |
| ESRD[例(%)] | 5(7.7) | 9(12.7) | 0.913 | 0.339 |
| 项目 | AKD治疗亚组(n=26) | AKD对照亚组(n=41) | 检验统计量值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 17/9 | 25/16 | 0.132 | 0.716 |
| 年龄(岁) | 13.8±5.1 | 12.8±4.3 | 0.683a | 0.558 |
| AKD分期[例(%)] | 0.073 | 0.964 | ||
| 1期 | 7(26.9) | 12(29.3) | ||
| 2期 | 10(38.5) | 16(39.0) | ||
| 3期 | 9(34.6) | 13(31.7) | ||
| Scr[M(P25,P75),μmol/L] | 74.34(32.76,92.18) | 88.95(36.13,109.75) | -2.218b | 0.036 |
| BUN[M(P25,P75),mmol/L] | 8.15(4.65,9.87) | 7.87(5.14,8.89) | -1.024b | 0.357 |
| UA(μmol/L) | 335.76±75.56 | 326.35±82.14 | 0.679a | 0.535 |
| eGFR[mL·min-1·(1.73 m2)-1] | 89.35±15.58 | 90.22±16.38 | 0.694a | 0.602 |
| 尿NAG酶(U·g-1·Cr-1) | 12.57±3.47 | 17.32±3.68 | 3.194a | 0.002 |
| 尿RBP(mg/L) | 0.85±0.18 | 0.79±0.21 | 1.548a | 0.164 |
| 尿NGAL(μg/L) | 43.19±11.23 | 55.72±14.56 | 2.254a | 0.032 |
| 中医证候评分(分) | 6.43±1.38 | 6.75±1.42 | 1.192a | 0.348 |
| CKD 3期[例(%)] | 6(23.1) | 20(48.8) | 4.427 | 0.036 |
| ESRD[例(%)] | 2(7.7) | 12(29.3) | 4.481 | 0.034 |
Table 2 General information and laboratory test results of children in AKD treatment sub-group and AKD control sub-group after treatment
| 项目 | AKD治疗亚组(n=26) | AKD对照亚组(n=41) | 检验统计量值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 17/9 | 25/16 | 0.132 | 0.716 |
| 年龄(岁) | 13.8±5.1 | 12.8±4.3 | 0.683a | 0.558 |
| AKD分期[例(%)] | 0.073 | 0.964 | ||
| 1期 | 7(26.9) | 12(29.3) | ||
| 2期 | 10(38.5) | 16(39.0) | ||
| 3期 | 9(34.6) | 13(31.7) | ||
| Scr[M(P25,P75),μmol/L] | 74.34(32.76,92.18) | 88.95(36.13,109.75) | -2.218b | 0.036 |
| BUN[M(P25,P75),mmol/L] | 8.15(4.65,9.87) | 7.87(5.14,8.89) | -1.024b | 0.357 |
| UA(μmol/L) | 335.76±75.56 | 326.35±82.14 | 0.679a | 0.535 |
| eGFR[mL·min-1·(1.73 m2)-1] | 89.35±15.58 | 90.22±16.38 | 0.694a | 0.602 |
| 尿NAG酶(U·g-1·Cr-1) | 12.57±3.47 | 17.32±3.68 | 3.194a | 0.002 |
| 尿RBP(mg/L) | 0.85±0.18 | 0.79±0.21 | 1.548a | 0.164 |
| 尿NGAL(μg/L) | 43.19±11.23 | 55.72±14.56 | 2.254a | 0.032 |
| 中医证候评分(分) | 6.43±1.38 | 6.75±1.42 | 1.192a | 0.348 |
| CKD 3期[例(%)] | 6(23.1) | 20(48.8) | 4.427 | 0.036 |
| ESRD[例(%)] | 2(7.7) | 12(29.3) | 4.481 | 0.034 |
| 项目 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||
|---|---|---|---|---|
| HR(95%CI) | P值 | HR(95%CI) | P值 | |
| Scra | 1.142(1.128~1.454) | 0.135 | 1.153(1.134~1.423) | 0.216 |
| 尿NAG酶a | 2.670(1.645~4.333) | 0.001 | 2.724(1.886~4.519) | 0.007 |
| 尿NGALa | 1.645(1.011~2.676) | 0.045 | 1.829(1.035~3.268) | 0.076 |
| AKI 3期a | 1.175(1.114~2.147) | 0.255 | 1.184(1.131~2.249) | 0.316 |
| 中医证候评分a | 1.463(1.328~1.954) | 0.308 | 1.573(1.387~2.408) | 0.335 |
| 中药治疗 | 0.421(0.235~0.754) | 0.004 | 0.482(0.319~0.843) | 0.008 |
Table 3 Analysis of factors influencing the progression from AKI to AKD in pediatric patients
| 项目 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||
|---|---|---|---|---|
| HR(95%CI) | P值 | HR(95%CI) | P值 | |
| Scra | 1.142(1.128~1.454) | 0.135 | 1.153(1.134~1.423) | 0.216 |
| 尿NAG酶a | 2.670(1.645~4.333) | 0.001 | 2.724(1.886~4.519) | 0.007 |
| 尿NGALa | 1.645(1.011~2.676) | 0.045 | 1.829(1.035~3.268) | 0.076 |
| AKI 3期a | 1.175(1.114~2.147) | 0.255 | 1.184(1.131~2.249) | 0.316 |
| 中医证候评分a | 1.463(1.328~1.954) | 0.308 | 1.573(1.387~2.408) | 0.335 |
| 中药治疗 | 0.421(0.235~0.754) | 0.004 | 0.482(0.319~0.843) | 0.008 |
| 项目 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||
|---|---|---|---|---|
| HR(95%CI) | P值 | HR(95%CI) | P值 | |
| Scra | 1.107(1.008~1.121) | 0.105 | 1.112(1.012~1.325) | 0.432 |
| 尿NAG酶a | 1.016(1.008~1.057) | 0.039 | 1.025(1.004~1.073) | 0.057 |
| 尿NGALa | 1.213(1.002~1.586) | 0.043 | 1.247(1.026~1.748) | 0.124 |
| AKI 3期a | 2.586(2.042~3.289) | 0.003 | 2.865(2.213~3.619) | 0.011 |
| 中医证候评分a | 1.142(1.020~1.618) | 0.078 | 1.236(1.043~1.867) | 0.125 |
| 中药治疗 | 0.613(0.318~0.876) | 0.014 | 0.665(0.422~0.953) | 0.040 |
Table 4 Analysis of risk factors for progression to CKD stage 3 in children with AKD
| 项目 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||
|---|---|---|---|---|
| HR(95%CI) | P值 | HR(95%CI) | P值 | |
| Scra | 1.107(1.008~1.121) | 0.105 | 1.112(1.012~1.325) | 0.432 |
| 尿NAG酶a | 1.016(1.008~1.057) | 0.039 | 1.025(1.004~1.073) | 0.057 |
| 尿NGALa | 1.213(1.002~1.586) | 0.043 | 1.247(1.026~1.748) | 0.124 |
| AKI 3期a | 2.586(2.042~3.289) | 0.003 | 2.865(2.213~3.619) | 0.011 |
| 中医证候评分a | 1.142(1.020~1.618) | 0.078 | 1.236(1.043~1.867) | 0.125 |
| 中药治疗 | 0.613(0.318~0.876) | 0.014 | 0.665(0.422~0.953) | 0.040 |
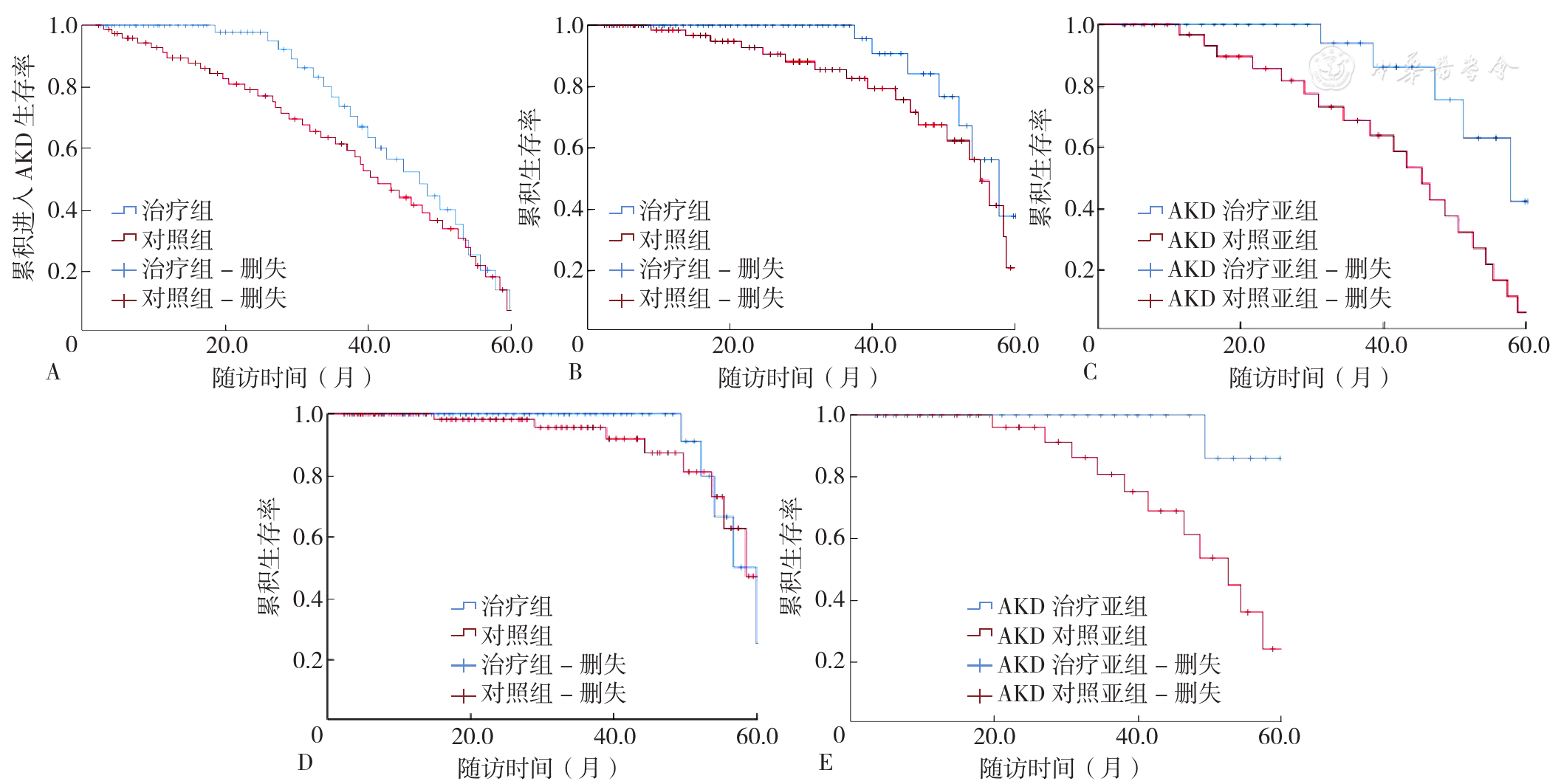
Figure 1 Survival Curves for Pediatric Patients with AKI and AKD
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
张沛,何旭,高春林,等. 加味升降散对儿童IgA肾病伴急性肾损伤的免疫调控作用及临床疗效观察[J]. 中医药学报,2023,51(1):62-66. DOI:10.19664/j.cnki.1002-2392.230013.
|
| [5] |
|
| [6] |
黎磊石,刘志红. 中国肾脏病学[M]. 北京:人民军医出版社,2008:442-464.
|
| [7] |
王卫平. 儿科学[M]. 8版. 北京:人民卫生出版社,2013:342.
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
张沛,何旭,姚俊,等. 加味升降散治疗气滞血瘀型儿童原发性肾病综合征合并急性肾损伤的临床疗效观察[J]. 中华中医药杂志,2021,36(9):5640-5644.
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [1] | FENG Yuxi, WANG Jinjin, CAI Yi, ZHU Runzhi, ZHU Qin. Research Progress on Protein Lactylation in Kidney Diseases [J]. Chinese General Practice, 2026, 29(21): 3056-3063. |
| [2] | HAN Congcong, QIU Xinyu, SHAN Chunfang, SONG Ning, CHEN Qingjie, MULADILI· Abudureheman, LI Xiaomei, YANG Yining, ZHAO Qian. Impact of Metabolic Obesity Phenotype on Long-term Prognosis after Percutaneous Coronary Intervention in Patients with Acute Coronary Syndrome [J]. Chinese General Practice, 2026, 29(21): 2950-2958. |
| [3] | LIU Yang, ZHOU Guoping, LI Xiaoshi, LI Ping, ZHANG Xin. Impact of Acute Respiratory Distress Syndrome Etiology on the Prognostic Value of Driving Pressure: a Prospective Cohort Study [J]. Chinese General Practice, 2026, 29(19): 2638-2647. |
| [4] | LUAN Xiaoqing, SUN Jingjing, LI Xiaoling, WANG Manxia. Research Progress on Potential Biomarkers of Neuromyelitis Optica Spectrum Disorder [J]. Chinese General Practice, 2026, 29(17): 2418-2424. |
| [5] | LIU Xiaoyu, ZHU Rongxin, ZHANG Bo, SU Hang, REN Xianqing. Defining Clinical Questions and Outcome Indicators in Guidelines for Diagnosis and Treatment of Nocturnal Enuresis in Children with Integrated Traditional Chinese and Western Medicine Based on Modified Delphi Method [J]. Chinese General Practice, 2026, 29(15): 2050-2055. |
| [6] | XIONG Siyu, LU Bing, JIANG Wenhong, YU Tingting. Study on the Relationship between Fructose-1, 6-Bisphosphate Aldolase A Expression before and after Targeted Drug Resistance in Lung Adenocarcinoma and Patient Prognosis [J]. Chinese General Practice, 2026, 29(14): 1883-1889. |
| [7] | CHEN Annan, YAN Zhixin, ZHANG Jian, SHEN Bo, DING Xiaoqiang, SONG Nana. Acidic Preconditioning Activates the Sodium-hydrogen Exchanger 1 to Regulate Intracellular pH Homeostasis and Reduce Renal Ischemia-reperfusion Injury [J]. Chinese General Practice, 2026, 29(12): 1607-1617. |
| [8] | YANG Jingran, MA Fang, WANG Yu, ZHANG Yimei, ZHOU Min. Summary of Best Evidence for Pain Management after Open-heart Surgery in Children with Congenital Heart Disease [J]. Chinese General Practice, 2026, 29(11): 1473-1480. |
| [9] | WANG Tingting, LIN Zehua, MA Yingchun, Committee of Kidney Disease Rehabilitation, Chinese Association of Rehabilitation Medicine. Specification of Rehabilitation Service for Elderly Patients with Comorbidity Complicated with Acute Kidney Injury [J]. Chinese General Practice, 2026, 29(11): 1361-1366. |
| [10] | SUN Xia, SHEN Wen, TANG Xiang, ZHONG Wei, WANG Kailin, DAI Zhiyin, ZHANG Chaopu, YUAN Wei, YUAN Guoyue. Analysis of Clinical Characteristics in Dilated Cardiomyopathy Patients with Different Weight Statuses and the Influence of Weight Management on the Prognosis [J]. Chinese General Practice, 2026, 29(11): 1448-1455. |
| [11] | XIA Ning, SHI Lan, DING Wanbao, ZHANG Jie, LONG Yi, DAI Hui, ZHANG Can, DAI Hailong. Clinical Characteristics and Prognosis of Patients with Amyloidosis [J]. Chinese General Practice, 2026, 29(09): 1161-1167. |
| [12] | GUAN Yanping, WU Yunxiao, XU Zhifei. Correlation between Obstructive Sleep Apnea Syndrome and Emotional-behavioural Problems in Preschool Children [J]. Chinese General Practice, 2026, 29(09): 1155-1160. |
| [13] | WANG Lina, LEI Jingshu, LI Kuibao, WANG Ruiying, LI Xinmiao, WANG Fangfang, GUO Xiaorong, NIU Ruihao, ZHAO Wei, ZHOU Fangfang, ZHAO Jingjing, LEE CHONGYOU. Review on Inflammatory Response in Patients with Acute Myocardial Infarction [J]. Chinese General Practice, 2026, 29(06): 790-801. |
| [14] | LEI Chunxin, ZHANG Xiya, ZHANG Yan, CHEN Jiaqi, LIU Zihan, LUO Jing, TAO Qingwen. Clinical Characteristics and Influencing Factors of Primary Sjögren's Disease with Dryness and Blood-stasis Syndrome [J]. Chinese General Practice, 2026, 29(06): 718-725. |
| [15] | WANG Xue, YANG Chengming, WANG Ziyun, ZHOU Zhong. Analysis on Prognosis and Influencing Factors in Patients with Post-tuberculosis Bronchiectasis [J]. Chinese General Practice, 2026, 29(05): 606-611. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||