
Chinese General Practice ›› 2025, Vol. 28 ›› Issue (18): 2234-2240.DOI: 10.12114/j.issn.1007-9572.2024.0383
• Article • Previous Articles Next Articles
Received:2024-06-11
Revised:2024-12-25
Published:2025-06-20
Online:2025-04-25
Contact:
LI Guoxin, LI Yunze
通讯作者:
李国信, 李昀泽
作者简介:作者贡献:
李国信进行文章的构思和设计;李昀泽进行结果的分析和解释;刘容进行研究数据的收集整理和统计学处理;梁丽喆和陆飞进行论文的修订,对文章整体监督管理;党世竟、吴红江、刘晓颐负责论文的校对。
CLC Number:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2024.0383
| 人群 | 例数 | 血小板计数[M(P25,P75),×109/L] | 淋巴细胞计数[M(P25,P75),×109/L] | 单核细胞计数[M(P25,P75),×109/L] | 中性粒细胞计数[M(P25,P75),×109/L] | HDL-C[M(P25,P75),mmol/L] | LDL-C(mmol/L) | PIV[M(P25,P75)] |
|---|---|---|---|---|---|---|---|---|
| 正常人群 | 200 | 185.00(167.00,210.00) | 1.66(1.41,2.10) | 0.36(0.28,0.44) | 3.33(2.82,3.87) | 1.26(1.12,1.42) | 3.01±0.56 | 138.84(98.45,171.61) |
| ASO患者 | 600 | 219.00(183.00,259.00) | 1.66(1.29,2.12) | 0.40(0.31,0.51) | 3.95(3.29,4.92) | 1.12(0.95,1.34) | 3.32±0.98 | 204.28(132.91,331.71) |
| Z(t)值 | -7.727 | -1.195 | -4.406 | -7.731 | -6.971 | -4.298a | -10.034 | |
| P值 | <0.001 | 0.232 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| 人群 | SIRI[M(P25,P75)] | SII[M(P25,P75)] | MHR[M(P25,P75)] | NLR[M(P25,P75)] | SIRI/HDL-C[M(P25,P75)] | SIRI×LDL-C[M(P25,P75)] | PIV/HDL-C[M(P25,P75)] | PIV×LDL-C[M(P25,P75)] |
| 正常人群 | 0.72(0.50,0.94) | 374.82(303.12,440.94) | 0.28(0.22,0.35) | 2.01(1.54,2.39) | 0.55(0.39,0.73) | 2.07(1.43,2.84) | 108.44(74.04,137.25) | 405.86(274.97,523.57) |
| ASO患者 | 0.94(0.63,1.42) | 527.00(380.19,724.31) | 0.35(0.25,0.51) | 2.34(1.80,3.21) | 0.86(0.53,1.37) | 2.96(2.04,4.60) | 179.75(109.54,311.40) | 644.78(426.67,1 088.64) |
| Z(t)值 | -7.755 | -10.140 | -6.635 | -6.499 | -9.050 | -8.920 | -11.051 | -10.942 |
| P值 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
Table 1 Comparison of routine blood data,blood lipid data and comprehensive indexes between ASO patients and normal population
| 人群 | 例数 | 血小板计数[M(P25,P75),×109/L] | 淋巴细胞计数[M(P25,P75),×109/L] | 单核细胞计数[M(P25,P75),×109/L] | 中性粒细胞计数[M(P25,P75),×109/L] | HDL-C[M(P25,P75),mmol/L] | LDL-C(mmol/L) | PIV[M(P25,P75)] |
|---|---|---|---|---|---|---|---|---|
| 正常人群 | 200 | 185.00(167.00,210.00) | 1.66(1.41,2.10) | 0.36(0.28,0.44) | 3.33(2.82,3.87) | 1.26(1.12,1.42) | 3.01±0.56 | 138.84(98.45,171.61) |
| ASO患者 | 600 | 219.00(183.00,259.00) | 1.66(1.29,2.12) | 0.40(0.31,0.51) | 3.95(3.29,4.92) | 1.12(0.95,1.34) | 3.32±0.98 | 204.28(132.91,331.71) |
| Z(t)值 | -7.727 | -1.195 | -4.406 | -7.731 | -6.971 | -4.298a | -10.034 | |
| P值 | <0.001 | 0.232 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| 人群 | SIRI[M(P25,P75)] | SII[M(P25,P75)] | MHR[M(P25,P75)] | NLR[M(P25,P75)] | SIRI/HDL-C[M(P25,P75)] | SIRI×LDL-C[M(P25,P75)] | PIV/HDL-C[M(P25,P75)] | PIV×LDL-C[M(P25,P75)] |
| 正常人群 | 0.72(0.50,0.94) | 374.82(303.12,440.94) | 0.28(0.22,0.35) | 2.01(1.54,2.39) | 0.55(0.39,0.73) | 2.07(1.43,2.84) | 108.44(74.04,137.25) | 405.86(274.97,523.57) |
| ASO患者 | 0.94(0.63,1.42) | 527.00(380.19,724.31) | 0.35(0.25,0.51) | 2.34(1.80,3.21) | 0.86(0.53,1.37) | 2.96(2.04,4.60) | 179.75(109.54,311.40) | 644.78(426.67,1 088.64) |
| Z(t)值 | -7.755 | -10.140 | -6.635 | -6.499 | -9.050 | -8.920 | -11.051 | -10.942 |
| P值 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| 组别 | 例数 | 性别(男/女) | 年龄[M(P25,P75),岁] | 高血压[例(%)] | 糖尿病[例(%)] | 吸烟[例(%)] | 饮酒[例(%)] | 血小板计数[M(P25,P75),×109/L] | 淋巴细胞计数[M(P25,P75),×109/L] |
|---|---|---|---|---|---|---|---|---|---|
| 轻度组 | 200 | 108/92 | 68.00(61.25,77.75) | 114(57.0) | 127(63.5) | 50(25.0) | 28(14.0) | 200.00(165.25,236.75) | 1.76(1.42,2.18) |
| 中度组 | 200 | 115/85 | 67.00(60.00,75.00) | 141(70.5)a | 141(70.5) | 55(27.5) | 43(21.5)a | 221.50(189.00,262.00)a | 1.75(1.42,2.15) |
| 重度组 | 200 | 153/47ab | 70.00(63.00,79.75)b | 154(77.0)ab | 128(64.0) | 74(37.0)ab | 45(22.5)a | 232.50(194.25,274.50)a | 1.43(1.07,1.88)ab |
| 检验统计量值 | 25.062c | 8.161 | 19.186c | 2.718c | 7.659c | 5.536c | 35.72 | 31.68 | |
| P值 | <0.001 | 0.017 | <0.001 | 0.257 | 0.022 | 0.063 | <0.001 | <0.001 | |
| 组别 | 单核细胞计数[M(P25,P75),×109/L] | 中性粒细胞计数[M(P25,P75),×109/L] | HDL-C[M(P25,P75),mmol/L] | LDL-C(mmol/L) | PIV[M(P25,P75)] | SIRI[M(P25,P75)] | SII[M(P25,P75)] | ||
| 轻度组 | 0.33(0.27,0.42) | 3.29(2.73,3.78) | 1.20(1.04,1.42) | 3.45±0.96 | 125.08(100.58,155.77) | 0.60(0.49,0.76) | 370.62(284.23,458.94) | ||
| 中度组 | 0.39(0.32,0.47)a | 3.95(3.39,4.61)a | 1.13(1.00,1.31)a | 3.37±0.92 | 199.29(152.24,257.55)a | 0.89(0.69,1.15)a | 512.89(413.72,627.89)a | ||
| 重度组 | 0.51(0.41,0.66)ab | 5.02(4.29,6.43)ab | 1.01(0.87,1.23)ab | 3.13±1.02ab | 396.25(307.58,535.36)ab | 1.75(1.35,2.30)ab | 787.41(615.46,1 137.28)ab | ||
| 检验统计量值 | 135.30 | 230.02 | 42.63 | 5.84d | 392.30 | 372.32 | 271.83 | ||
| P值 | <0.001 | <0.001 | <0.001 | 0.003 | <0.001 | <0.001 | <0.001 | ||
| 组别 | MHR[M(P25,P75)] | NLR[M(P25,P75)] | SIRI/HDL-C[M(P25,P75)] | SIRI×LDL-C[M(P25,P75)] | PIV/HDL-C[M(P25,P75)] | PIV×LDL-C[M(P25,P75)] | |||
| 轻度组 | 0.27(0.19,0.36) | 1.81(1.44,2.31) | 0.50(0.35,0.67) | 2.01(1.51,2.66) | 102.62(75.32,131.26) | 401.29(295.49,550.68) | |||
| 中度组 | 0.34(0.25,0.45)a | 2.24(1.87,2.87)a | 0.82(0.60,1.06)a | 2.89(2.23,3.79)a | 177.57(125.54,230.52)a | 638.50(463.13,892.23)a | |||
| 重度组 | 0.51(0.36,0.72)ab | 3.46(2.61,4.84)ab | 1.70(1.25,2.56)ab | 5.44(3.65,7.72)ab | 376.60(294.16,564.60)ab | 1 249.18(844.13,1 801.21)ab | |||
| 检验统计量值 | 137.15 | 219.57 | 336.57 | 270.03 | 370.52 | 279.45 | |||
| P值 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
Table 2 Comparison of general information and comprehensive indicators among patients in different Rutherford staging groups
| 组别 | 例数 | 性别(男/女) | 年龄[M(P25,P75),岁] | 高血压[例(%)] | 糖尿病[例(%)] | 吸烟[例(%)] | 饮酒[例(%)] | 血小板计数[M(P25,P75),×109/L] | 淋巴细胞计数[M(P25,P75),×109/L] |
|---|---|---|---|---|---|---|---|---|---|
| 轻度组 | 200 | 108/92 | 68.00(61.25,77.75) | 114(57.0) | 127(63.5) | 50(25.0) | 28(14.0) | 200.00(165.25,236.75) | 1.76(1.42,2.18) |
| 中度组 | 200 | 115/85 | 67.00(60.00,75.00) | 141(70.5)a | 141(70.5) | 55(27.5) | 43(21.5)a | 221.50(189.00,262.00)a | 1.75(1.42,2.15) |
| 重度组 | 200 | 153/47ab | 70.00(63.00,79.75)b | 154(77.0)ab | 128(64.0) | 74(37.0)ab | 45(22.5)a | 232.50(194.25,274.50)a | 1.43(1.07,1.88)ab |
| 检验统计量值 | 25.062c | 8.161 | 19.186c | 2.718c | 7.659c | 5.536c | 35.72 | 31.68 | |
| P值 | <0.001 | 0.017 | <0.001 | 0.257 | 0.022 | 0.063 | <0.001 | <0.001 | |
| 组别 | 单核细胞计数[M(P25,P75),×109/L] | 中性粒细胞计数[M(P25,P75),×109/L] | HDL-C[M(P25,P75),mmol/L] | LDL-C(mmol/L) | PIV[M(P25,P75)] | SIRI[M(P25,P75)] | SII[M(P25,P75)] | ||
| 轻度组 | 0.33(0.27,0.42) | 3.29(2.73,3.78) | 1.20(1.04,1.42) | 3.45±0.96 | 125.08(100.58,155.77) | 0.60(0.49,0.76) | 370.62(284.23,458.94) | ||
| 中度组 | 0.39(0.32,0.47)a | 3.95(3.39,4.61)a | 1.13(1.00,1.31)a | 3.37±0.92 | 199.29(152.24,257.55)a | 0.89(0.69,1.15)a | 512.89(413.72,627.89)a | ||
| 重度组 | 0.51(0.41,0.66)ab | 5.02(4.29,6.43)ab | 1.01(0.87,1.23)ab | 3.13±1.02ab | 396.25(307.58,535.36)ab | 1.75(1.35,2.30)ab | 787.41(615.46,1 137.28)ab | ||
| 检验统计量值 | 135.30 | 230.02 | 42.63 | 5.84d | 392.30 | 372.32 | 271.83 | ||
| P值 | <0.001 | <0.001 | <0.001 | 0.003 | <0.001 | <0.001 | <0.001 | ||
| 组别 | MHR[M(P25,P75)] | NLR[M(P25,P75)] | SIRI/HDL-C[M(P25,P75)] | SIRI×LDL-C[M(P25,P75)] | PIV/HDL-C[M(P25,P75)] | PIV×LDL-C[M(P25,P75)] | |||
| 轻度组 | 0.27(0.19,0.36) | 1.81(1.44,2.31) | 0.50(0.35,0.67) | 2.01(1.51,2.66) | 102.62(75.32,131.26) | 401.29(295.49,550.68) | |||
| 中度组 | 0.34(0.25,0.45)a | 2.24(1.87,2.87)a | 0.82(0.60,1.06)a | 2.89(2.23,3.79)a | 177.57(125.54,230.52)a | 638.50(463.13,892.23)a | |||
| 重度组 | 0.51(0.36,0.72)ab | 3.46(2.61,4.84)ab | 1.70(1.25,2.56)ab | 5.44(3.65,7.72)ab | 376.60(294.16,564.60)ab | 1 249.18(844.13,1 801.21)ab | |||
| 检验统计量值 | 137.15 | 219.57 | 336.57 | 270.03 | 370.52 | 279.45 | |||
| P值 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| 指标 | rs值 | P值 |
|---|---|---|
| PIV | 0.806 | <0.001 |
| SIRI | 0.780 | <0.001 |
| SII | 0.672 | <0.001 |
| MHR | 0.474 | <0.001 |
| NLR | 0.598 | <0.001 |
| SIRI/HDL-C | 0.742 | <0.001 |
| SIRI×LDL-C | 0.667 | <0.001 |
| PIV/HDL-C | 0.784 | <0.001 |
| PIV×LDL-C | 0.682 | <0.001 |
Table 3 Correlation of complex indexes with different Rutherford staging groups
| 指标 | rs值 | P值 |
|---|---|---|
| PIV | 0.806 | <0.001 |
| SIRI | 0.780 | <0.001 |
| SII | 0.672 | <0.001 |
| MHR | 0.474 | <0.001 |
| NLR | 0.598 | <0.001 |
| SIRI/HDL-C | 0.742 | <0.001 |
| SIRI×LDL-C | 0.667 | <0.001 |
| PIV/HDL-C | 0.784 | <0.001 |
| PIV×LDL-C | 0.682 | <0.001 |
| 指标 | B | SE | Wald χ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| PIV | 0.051 | 0.023 | 5.207 | 0.022 | 1.053 | 1.007~1.100 |
| SIRI | -13.181 | 4.493 | 8.607 | 0.003 | 0.000 | 0.000~0.013 |
| SII | -0.003 | 0.003 | 0.827 | 0.363 | 0.997 | 0.991~1.003 |
| MHR | 0.491 | 1.830 | 0.072 | 0.788 | 1.634 | 0.045~58.996 |
| NLR | 1.021 | 0.615 | 2.755 | 0.097 | 2.777 | 0.831~9.274 |
| SIRI/HDL-C | 9.682 | 3.229 | 8.993 | 0.003 | 16 025.753 | 28.614~8 975 503.286 |
| SIRI×LDL-C | 0.220 | 0.681 | 0.108 | 0.743 | 1.250 | 0.330~4.750 |
| PIV/HDL-C | -0.030 | 0.015 | 4.578 | 0.032 | 0.970 | 0.940~1.000 |
| PIV×LDL-C | 0.000 | 0.003 | 0.262 | 0.609 | 1.000 | 1.000~1.010 |
Table 4 Multivariate Logistic regression analysis of factors affecting ASO
| 指标 | B | SE | Wald χ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| PIV | 0.051 | 0.023 | 5.207 | 0.022 | 1.053 | 1.007~1.100 |
| SIRI | -13.181 | 4.493 | 8.607 | 0.003 | 0.000 | 0.000~0.013 |
| SII | -0.003 | 0.003 | 0.827 | 0.363 | 0.997 | 0.991~1.003 |
| MHR | 0.491 | 1.830 | 0.072 | 0.788 | 1.634 | 0.045~58.996 |
| NLR | 1.021 | 0.615 | 2.755 | 0.097 | 2.777 | 0.831~9.274 |
| SIRI/HDL-C | 9.682 | 3.229 | 8.993 | 0.003 | 16 025.753 | 28.614~8 975 503.286 |
| SIRI×LDL-C | 0.220 | 0.681 | 0.108 | 0.743 | 1.250 | 0.330~4.750 |
| PIV/HDL-C | -0.030 | 0.015 | 4.578 | 0.032 | 0.970 | 0.940~1.000 |
| PIV×LDL-C | 0.000 | 0.003 | 0.262 | 0.609 | 1.000 | 1.000~1.010 |
| 指标 | B | SE | Wald χ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| PIV | 0.010 | 0.008 | 1.390 | 0.238 | 1.010 | 0.994~1.026 |
| SIRI | -4.659 | 1.504 | 9.589 | 0.002 | 0.009 | 0.000~0.181 |
| SII | 0.001 | 0.003 | 0.001 | 0.975 | 1.000 | 0.994~1.006 |
| MHR | 1.605 | 1.670 | 0.924 | 0.337 | 4.979 | 0.189~131.530 |
| NLR | 0.549 | 0.560 | 0.959 | 0.327 | 1.731 | 0.577~5.188 |
| SIRI×LDL-C | 0.510 | 0.142 | 12.835 | 0.001 | 1.665 | 1.260~2.201 |
| PIV/HDL-C | 0.014 | 0.005 | 6.653 | 0.005 | 1.014 | 1.003~1.024 |
Table 5 Multivariate Logistic regression analysis of the influencing factors of ASO occurrence after the elimination of collinear indicators
| 指标 | B | SE | Wald χ2值 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| PIV | 0.010 | 0.008 | 1.390 | 0.238 | 1.010 | 0.994~1.026 |
| SIRI | -4.659 | 1.504 | 9.589 | 0.002 | 0.009 | 0.000~0.181 |
| SII | 0.001 | 0.003 | 0.001 | 0.975 | 1.000 | 0.994~1.006 |
| MHR | 1.605 | 1.670 | 0.924 | 0.337 | 4.979 | 0.189~131.530 |
| NLR | 0.549 | 0.560 | 0.959 | 0.327 | 1.731 | 0.577~5.188 |
| SIRI×LDL-C | 0.510 | 0.142 | 12.835 | 0.001 | 1.665 | 1.260~2.201 |
| PIV/HDL-C | 0.014 | 0.005 | 6.653 | 0.005 | 1.014 | 1.003~1.024 |
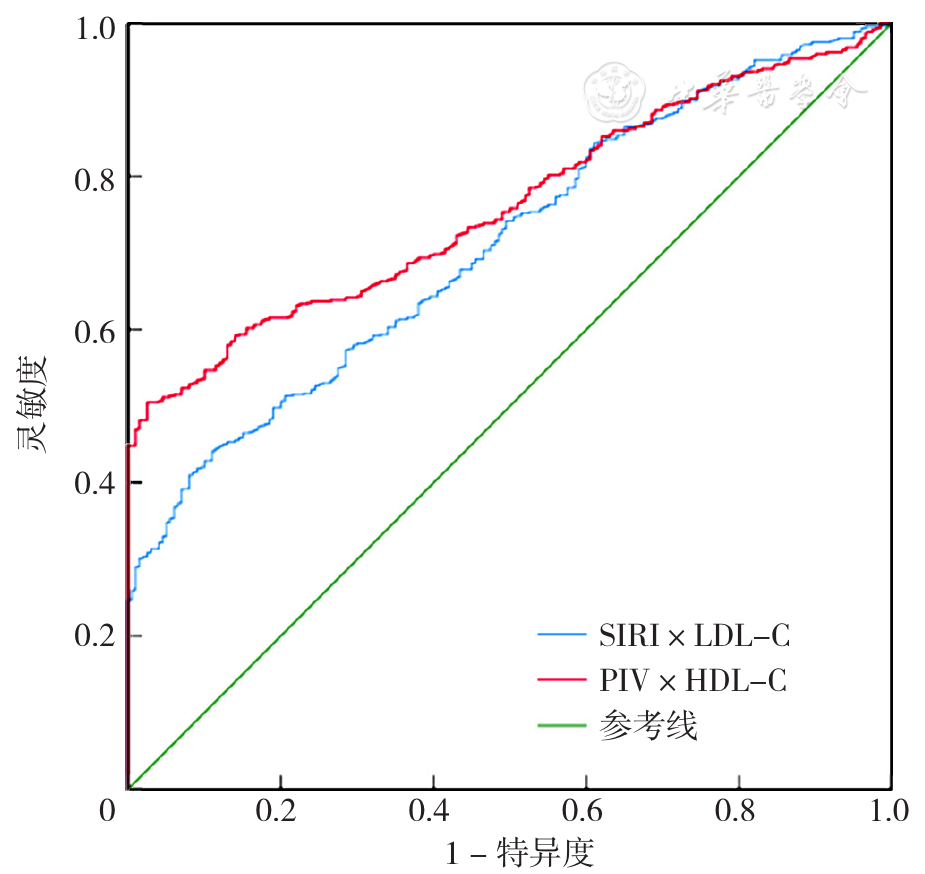
Figure 1 ROC curves for predicting the occurrence of ASO using SIRI×LDL-C and PIV/HDL-C
| 指标 | AUC | 95%CI | P值 | 灵敏度 | 特异度 | 最佳截断值 |
|---|---|---|---|---|---|---|
| SIRI×LDL-C | 0.710 | 0.673~0.748 | <0.001 | 0.442 | 0.890 | 3.23 |
| PIV/HDL-C | 0.761 | 0.728~0.793 | <0.001 | 0.505 | 0.975 | 177.17 |
Table 6 Results of ROC curve analysis for predicting the occurrence of ASO using SIRI×LDL-C and PIV/HDL-C
| 指标 | AUC | 95%CI | P值 | 灵敏度 | 特异度 | 最佳截断值 |
|---|---|---|---|---|---|---|
| SIRI×LDL-C | 0.710 | 0.673~0.748 | <0.001 | 0.442 | 0.890 | 3.23 |
| PIV/HDL-C | 0.761 | 0.728~0.793 | <0.001 | 0.505 | 0.975 | 177.17 |
| [1] |
中华医学会外科学分会血管外科学组. 下肢动脉硬化闭塞症诊治指南[J]. 中华普通外科学文献(电子版),2016,10(1):1-18. DOI:10.3877/cma.j.issn.1674-0793.2016.01.001.
|
| [2] |
任娇,吴少虹,郭莉莉. 下肢动脉硬化闭塞症的足部CT灌注成像的应用研究[J]. 实用放射学杂志,2023,39(9):1426-1430.
|
| [3] |
林印胜,陈梅,郭坚东,等. Viabahn覆膜支架与旁路途径治疗下肢动脉硬化闭塞症有效性的系统评价及Meta分析[J]. 介入放射学杂志,2023,32(8):774-781. DOI:10.3969/j.issn.1008-794X.2023.08.010.
|
| [4] |
马洁,刘毅,欧金鹏,等. 免疫调控及靶向治疗在动脉粥样硬化斑块炎症反应中的研究进展[J]. 临床神经病学杂志,2024,37(2):157-160. DOI:10.3969/j.issn.1004-1648.2024.02.027.
|
| [5] |
高扬,张哲林. 动脉粥样硬化形成机制及诊疗技术的研究进展[J]. 心脑血管病防治,2024,24(3):45-49. DOI:10.3969/j.issn.1009-816x.2024.03.011.
|
| [6] |
叶雪瑞,万秋华,杨鑫伟,等. 单核细胞/高密度脂蛋白胆固醇比值与冠心病相关性的研究进展[J]. 中国医药科学,2024,14(8):37-40,117. DOI:10.20116/j.issn2095-0616.2024.08.09.
|
| [7] |
陈佳美,季优苗. 单核细胞/高密度脂蛋白胆固醇比值对急性脑桥梗死早期神经功能恶化的预测意义[J]. 中南医学科学杂志,2024,52(1):102-105. DOI:10.15972/j.cnki.43-1509/r.2024.01.024.
|
| [8] |
辛浩宇.不同时段中性粒细胞比淋巴细胞比值对机械取栓术后临床结果的预测作用[D]. 大连:大连医科大学,2023.
|
| [9] |
鲁明,蒋学俊,陶波,等. 中性粒细胞和淋巴细胞比与动脉粥样硬化研究进展[J]. 中国心血管病研究,2016,14(5):392-396. DOI:10.3969/j.issn.1672-5301.2016.05.003.
|
| [10] |
|
| [11] |
|
| [12] |
黄小宇,张丽晖,王静,等. 全身免疫炎症指数与心血管疾病相关性的研究进展[J]. 中西医结合心脑血管病杂志,2024,22(7):1266-1269. DOI:10.12102/j.issn.1672-1349.2024.07.018.
|
| [13] |
陈云,刘璐瑶,刘新灿 等. SII、SIRI和AISI对高血压颈动脉斑块形成的预测价值[J].郑州大学学报(医学版),2024,(3):369-372.
|
| [14] |
王婷. NLR、PLR、SIRI在大动脉粥样硬化型脑梗死中的相关研究[D]. 太原:山西医科大学,2023.
|
| [15] |
和军辉,万大国,董静,等. 泛免疫炎症值、全身免疫炎症指数与急性冠脉综合征患者易损斑块的相关性研究[J]. 中国全科医学,2024,27(24):2976-2981. DOI:10.12114/j.issn.1007-9572.2023.0679.
|
| [16] |
|
| [17] |
徐敏敏. 泛免疫炎症值与早发冠心病及其冠脉病变严重程度的相关性分析[D]. 大连:大连医科大学,2023.
|
| [18] |
|
| [19] |
钟毅.下肢动脉硬化闭塞与冠状动脉病变关系的相关性研究. 广西壮族自治区,南宁市第一人民医院,2020-04-20.
|
| [20] |
褚启龙. 医学统计中常用的χ2检验在SPSS软件中的实现途径[J]. 卫生职业教育,2016,34(17):42-44.
|
| [21] |
裴磊磊,赵亚玲,康轶君,等. 医用多因素分析及SPSS操作课程教学经验探讨[J]. 医学教育研究与实践,2023,31(5):603-607. DOI:10.13555/j.cnki.c.m.e.2023.05.018.
|
| [22] |
周慧超,孙珂,许聿新,等. 基于Logistic回归模型及ROC曲线的糖尿病足溃疡复发的危险因素分析[J]. 西部医学,2024,36(5):744-748. DOI:10.3969/j.issn.1672-3511.2024.05.022.
|
| [23] |
厉倬学,林富,李归宿,等. 基于Logistic回归及ROC曲线研究卒中患者120急救入院的影响因素[J]. 临床医学研究与实践,2024,9(9):25-29. DOI:10.19347/j.cnki.2096-1413.202409007.
|
| [24] | |
| [25] |
栾鑫,李国歌,丁耀威,等. 全身免疫炎症指数和凋亡相关斑点样蛋白对脑卒中诊断的价值研究[J]. 国际检验医学杂志,2023,44(23):2817-2821. DOI:10.3969/j.issn.1673-4130.2023.23.001.
|
| [26] |
郭慧娟,李天艺,李媛媛. 全身免疫炎症指数与中老年2型糖尿病患者颈动脉不稳定斑块的相关性及其预测价值[J]. 河南医学研究,2023,32(2):222-226. DOI:10.3969/j.issn.1004-437X.2023.02.007.
|
| [27] |
吕超,韩兵,刘兴华,等. 下肢动脉硬化闭塞症的病理机制及治疗进展研究[J]. 医学理论与实践,2022,35(18):3088-3090. DOI:10.19381/j.issn.1001-7585.2022.18.009.
|
| [28] |
杜以龙.下肢动脉硬化闭塞症的发病机制、诊断和治疗进展[C]//榆林市医学会.第三届全国医药研究论坛论文集(三). 沂南县人民医院,2023:6. DOI:10.26914/c.cnkihy.2023.050105.
|
| [29] |
王洁,龙霖梓,曲华,等. 系统免疫炎症指数与冠心病预后关系的Meta分析[J]. 中国循证医学杂志,2023,23(10):1143-1147.
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||